Article Text

Abstract
Objective To characterise the time window in which endovascular thrombectomy (EVT) is associated with good outcome, and to test the differential relationship between functional outcome and onset-to-reperfusion time (ORT), depending on collateral status.
Methods This was a retrospective analysis of clinical and imaging data of 554 consecutive patients, who had recanalisation success by EVT for anterior circulation large artery occlusion, from the prospectively maintained registries of 16 comprehensive stroke centres between September 2010 and December 2015. The patients were dichotomised into good and poor collateral groups, based on CT angiography. We tested whether the likelihood of good outcome (modified Rankin Scale, 0–2) by ORT was different between two groups.
Results ORT was 298 min±113 min (range, 81–665 min), and 84.5% of patients had good collaterals. Age, diabetes mellitus, previous infarction, National Institutes of Health Stroke Scale, good collaterals (OR 40.766; 95% CI 10.668 to 155.78; p<0.001) and ORT (OR 0.926 every 30 min delay; 95% CI 0.862 to 0.995; p=0.037) were independently associated with good outcome. The drop in likelihood of good outcome associated with longer ORT was significantly faster in poor collateral group (OR 0.305 for every 30 min; 95% CI 0.113 to 0.822) than in good collateral group (OR 0.926 for every 30 min; 95% CI 0.875 to 0.980).
Conclusions Earlier successful recanalisation was strongly associated with good outcome in poor collateral group; however, this association was weak during the tested time window in good collateral group. This suggests that the ORT window for good outcome can be adjusted according to collateral status.
Statistics from Altmetric.com
Introduction
Following successful randomised controlled trials, mechanical endovascular thrombectomy (EVT) is now recommended as the first-line treatment for acute stroke caused by anterior circulation large vessel occlusion (AC-LVO).1 2 Subgroup analysis of the primary endpoint showed no heterogeneity of treatment effect across prespecified subgroups in meta-analysis of individual patient data from five randomised trials.3 In general, the benefit of EVT decreases as onset-to-reperfusion time (ORT) increases across all randomised trials.3–9 Therefore, efforts to improve clinical outcomes have focused on reducing ORT and increasing recanalisation rate.10 11
On the other hand, there have been efforts to extend the time window for EVT depending on imaging evaluation, as certain imaging features (mismatch profile or collateral status) can extend the time window.12–15
Many studies have shown that collateral status on CT angiography (CTA) is strongly and independently associated with functional outcome.13–20 In addition, several recent studies have suggested that ORT for the likelihood of good outcome can be adjusted based on collateral status.21–23
We hypothesised that ORT for the likelihood of good outcome after successful recanalisation with EVT differs according to pretreatment collateral status. Therefore, we evaluated the likelihood of good outcome by ORT in a large cohort of patients with good and poor collaterals who underwent EVT for AC-LVO.
Patients and methods
Patient enrolment
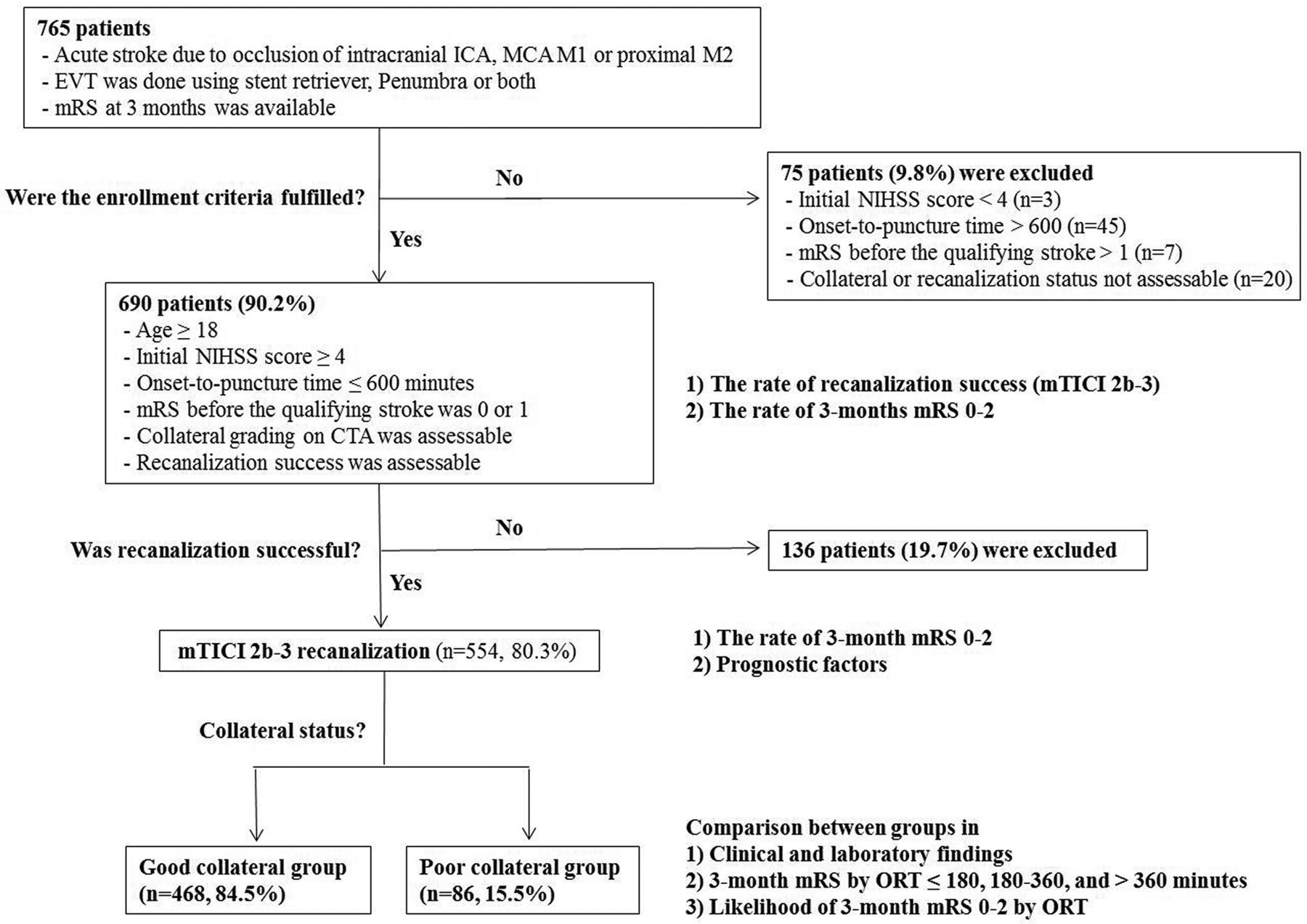
This was a retrospective analysis of cohorts that were prospectively registered between September 2010 and December 2015. The current study was initiated by the Korea Health Technology R&D Project, and a total of 16 comprehensive stroke centres participated. We identified all consecutive patients who underwent EVT using a stent retriever (Solitaire AB/FR, ev3 Irvine, CA, USA; Trevo Proview, Stryker, CA, USA), Penumbra system (Penumbra, Alameda, California) or both for acute ischaemic stroke due to AC-LVO and who had functional outcomes (by modified Rankin Scale (mRS) profile) at 3 months. AC-LVO was defined as intracranial internal carotid artery (ICA) or middle cerebral artery (MCA) M1, or proximal M2 occlusion. Tandem atherosclerotic or dissecting cervical ICA occlusion accompanied by intracranial LVO was included. LVO due to intracranial artery dissection was excluded. Bilateral AC-LVO was excluded. Study enrolment criteria were as follows: (1) age ≥18 years; (2) initial National Institutes of Health Stroke Scale (NIHSS) score ≥4; (3) onset-to-puncture time equal to or less than 600 min; (4) mRS of 0 or 1 before qualifying stroke; (5) collateral grading assessable on CTA; and (6) recanalisation success assessable on catheter angiogram during procedure (figure 1). The Institutional Review Boards of all participating hospitals approved this study and waived the requirement for written informed consent for study inclusion based on the retrospective study design.

Study protocol. CTA, CT angiography; EVT, endovascular thrombectomy; ICA, internal carotid artery; MCA, middle cerebral artery; mRS, modified Rankin Scale; mTICI, modified thrombolysis in cerebral ischaemia; NIHSS, National Institutes of Health Stroke Scale; ORT, onset-to-reperfusion time.
Data collection and assessment
All data, including clinical and laboratory findings, were obtained from the registries for acute stroke at each participating hospital, and then listed in the predefined case report form (CRF). Procedural details, including complications during EVT, were obtained from the neurointerventional database of each participating centre, and were also added in the CRF. CRFs were anonymised and then sent to a central core laboratory (Severance Hospital). All imaging data including pretreatment non-enhanced CT (NECT) and CTA, catheter angiograms during EVT, and follow-up CT or MRI were anonymised and sent to the central core laboratory as digital imaging and communication in medicine (DICOM) files. Two neuroradiologists independently assessed the images for Alberta Stroke Program Early CT Score (ASPECTS) and collateral status on CTA using a commercialised DICOM viewer (OsiriX, Pixmeo, Geneva, Switzerland). ASPECTS was evaluated on images of 5 mm thickness NECT, and CTA collateral grade was assessed on 20 mm thickness maximum intensity projection images of single-phase CTA. In patients who underwent multiphase CTA, we only used first-phase images to evaluate collateral status. CTA collateral grade was dichotomised into either good or poor collateral. Poor collateral was defined as few or no vessel markings in more than half of MCA territory on the affected side,16 the same as in the Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Time (ESCAPE) trial.24 To reduce misclassification of good to poor collateral groups, patients in whom vessel markings were not well visualised in the contralateral hemisphere were excluded. Two interventional neuroradiologists independently assessed whether recanalisation success was achieved on catheter angiograms during EVT using the same software. Those reviewers were blind to ASPECTS, collateral status and clinical outcome. Recanalisation success was defined as modified thrombolysis in cerebral ischaemia (mTICI) grade 2b or 3 on final control angiogram. Kappa values for inter-rater agreement of ASPECTS (≤7 vs 8–10), CTA collateral grade (good vs poor) and recanalisation success (mTICI 0-2a vs 2b-3) were 0.657, 0.875 and 0.813, respectively. Discrepant cases were resolved by consensus between raters who remained blind to both the patient’s clinical outcome and findings on follow-up CT or MRI. If CTA collateral grade or recanalisation success was difficult to analyse due to poor image quality, or when vessel markings in the contralateral hemisphere were not well visualised on CTA, the case was considered undetermined and was excluded from analysis.
Outcome measurement
Rates of recanalisation success and good outcome were evaluated in all patients who fulfilled the enrolment criteria. Good outcome was defined as mRS 0–2 at 3 months. Rate of good outcome and prognostic factors were evaluated in patients with recanalisation success. Then, patients were dichotomised into good and poor collateral groups based on CTA. The two groups were compared in mRS profiles after being subgrouped into ≤180 min, 180–360 min and >360 min by ORT. Finally, we tested whether the likelihood of good outcome by ORT differed between the two groups (figure 1).
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics V.23 (IBM). The graph was composed using R statistical software (V.3.2.2, http://www.r-project.org). All categorical variables are presented as number and frequency (%), while continuous variables are presented as mean±SD or median±IQR. In univariate analysis, χ2 test, Fisher’s exact test, Student’s t-test and Mann-Whitney U test were appropriately used to find factors for good outcome in patients with recanalisation success. To find independent factors for good outcome, multivariate binary logistic regression analysis was performed. Variables with potential associations (p<0.20) in univariate analysis were included in the binary logistic regression analysis. Study model’s goodness of fit was assessed by the Hosmer-Lemeshow test.
We have described the effect of ORT on the likelihood of good outcome with OR and 95% CI for increased delays with 30 min intervals. We also tested whether the likelihood of good outcome by ORT differed between good and poor collateral groups using the log-rank test. Adjusted OR of the two groups for every 30 min delay and p values were derived from the binary logistic regression analysis.
Sensitivity analysis was performed to examine the validity of detected associations. Since various EVT methods were applied in this study, we analysed the association between ORT and likelihood of good outcome in patients who received EVT using stent retriever alone.
A p value less than 0.05 was considered significant with a 95% CI.
Results
A total of 805 patients underwent EVT for acute stroke caused by Anterior Circulation Large Artery Occlusion (AC-LAO) using stent retriever, Penumbra or both; among them, 765 patients (95.0%) had mRS available at 3 months. Of the 765 patients, 690 (90.2%) fulfilled the enrolment criteria (figure 1). Of these 690 patients, 554 (80.3%) showed recanalisation success and 343 (49.7%) had good outcome at 3 months. The mean±SD of ORT was 298.4 min±113.8 min (range, 81–665 min), and 130 patients (23.5%) had ORT>360 min.
Rate of good outcome was significantly higher in patients with recanalisation success (308 of 554 patients, 55.6%) than in those with recanalisation failure (35 of 136 patients, 25.7%). In the 554 patients with recanalisation success, age (OR 0.944; 95% CI 0.919 to 0.970; p<0.001), diabetes mellitus (OR 0.358; 95% CI 0.192 to 0.669; p=0.001), previous ischaemic stroke (OR 0.376; 95% CI 0.191 to 0.738; p=0.004), initial NIHSS (OR 0.914; 95% CI 0.865 to 0.96; p=0.002), good collateral on CTA (OR 40.766; 95% CI 10.668 to 155.78; p<0.001) and ORT (OR 0.926 every 30 min delay; 95% CI 0.862 to 0.995; p=0.037) were independent factors for good outcome (table 1).
Predictors for good outcome in patients with recanalisation success (n=554)
Of the 554 patients with recanalisation success, 468 (84.5%) were classified into good collateral group and the remaining 86 patients (15.5%) were classified into poor collateral group. The mean±SD of onset-to-door, door-to-image, image-to-puncture and puncture-to-recanalisation times were 112 min±105 min, 24 min±28 min, 96min±50 min and 66min±44 min, respectively. After dichotomisation, significant differences were found between good and poor collateral groups in ORT, as well as incidences of hypertension, smoking history, previous ischaemic stroke, tandem cervical and intracranial artery occlusion, distal ICA involvement, haemorrhagic infarction type 2, parenchymal haematoma type 2, good outcome at 3 months and mortality (table 2). ORT remained an independent prognostic factor in both good (p=0.007) and poor collateral groups (p=0.019) (table 3). In patients with good collaterals, the clinical features of age, diabetes mellitus, stroke history, initial NIHSS score and ORT determined the functional outcome after successful recanalisation with EVT. In contrast, only ORT independently determined the functional outcome after successful recanalisation in patients with poor collaterals.
Comparisons between poor and good collateral groups
Predictors for good outcome in good and poor collateral groups
Good collateral group showed significantly better 3-month mRS profiles. After subgrouping into ORT≤180 min, 180–360 min and >360 min, better 3-month mRS profiles were observed in good collateral group across every subgroup (p<0.01 for every subgroup) (figure 2). Regression curve for likelihood of good outcome by ORT showed a significantly faster drop in poor collateral group (adjusted OR 0.305 every 30 min delay; 95% CI 0.113 to 0.822) than in good collateral group (adjusted OR 0.926 every 30 min delay; 95% CI 0.875 to 0.980) (p<0.01) (table 3 and figure 3). ORT cut-off for good outcome was 200 min in patients with poor collaterals. In fact, no patient with poor collateral and ORT>174 min had good outcome. In contrast, the likelihood of good outcome decreased slowly with a prolonged ORT. Therefore, no clear cut-off time point of ORT for good outcome rate <50% was observed during the tested ORT window in those with good collaterals.

Distributions of 3-month modified Rankin Scale score between good and poor collateral groups by onset-to-recanalisation time. mRS, modified Rankin Scale.

{kind=link}
{kind=link}
{kind=link}
Regression curves of the likelihood of good outcome by onset-to-recanalisation time, as predicted by unadjusted analysis based on collateral status. ORT, onset to-recanalisation time.
Sensitivity analysis showed consistent findings of differential association between ORT and good outcome after EVT, depending on the collateral status (online supplementary figure).
Supplementary file 1
Discussion
The major findings of this study were that: (1) no clear cut-off time point was observed for EVT during the tested ORT window (within 600 min of onset-to-puncture time after last seen well) in these patients; and (2) in patients with poor collaterals, ORT was the main determinant for likelihood of good outcome after successful recanalisation.
The present study has one of the largest cohorts of real-world data on this topic. Poorer collateral development is linked to faster infarct growth. Thus, collateral status becomes far more important with prolonged time of image-to-recanalisation (image-to-puncture plus puncture-to-recanalisation).9 In this study, image-to-puncture and puncture-to-recanalisation times were 96 min±50 min and 66 min±44 min, respectively. As suggested by post hoc analysis of Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion (REVASCAT),9 prolonged image-to-recanalisation time seemed to make the effect of collateral status on the likelihood of good outcome by ORT accentuated. In poor collaterals, if onset-to-image time was prolonged, patients would show large infarct core on initial imaging and therefore would not be candidates for EVT. On the contrary, if onset-to-image time was very short, patients would show small infarct core on initial imaging and become candidates for EVT. With much shorter time for image-to-recanalisation time compared with that in our study, patients with small infarct core, due to very short onset-to-image time, might have good outcome after successful recanalisation even if they belonged to poor collateral group. Our results are in line with those from a meta-analysis of individual patient data from five randomised trials of EVT and CT Perfusion to predict Response to Recanalization in Ischemic Stroke Project (CRISP), which suggested that ORT is strongly associated with outcome after EVT, but with less impact in certain patients.4 23 Our findings indicate that every effort to shorten ORT is more critical in patients with poor collaterals. On the other hand, in good collaterals, while a significant association of outcome with ORT was shown, cut-off time for good outcome could not be provided during the tested time window. To find the cut-off ORT for good outcome in good collaterals, a wider range of tested time window may be needed. In addition, other variables either took higher weightage or had stronger association with good outcome compared with ORT.
Recent EVT randomised trials were successfully performed by increasing recanalisation rate and reducing ORT. However, although recanalisation was successful within 180 min after symptom onset, approximately 32% of patients still had unfavourable outcomes.5 In contrast, a meta-analysis of five randomised trials (Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke Trials (HERMES)) has suggested that patients can benefit from EVT for up to 7.3 hours of onset-to-puncture time.4 Such contradictory finding is most likely associated with the degree of collateral development of an individual patient. Collateral status has been suggested as a strong independent predictor for functional outcome in many studies, regardless of recanalisation success.12–23 Furthermore, several recent studies have suggested that ORT for the likelihood of good outcome can be adjusted by collateral status.12 21–23 In this study, poor collateral group showed significantly faster drop in the likelihood of good outcome compared with good collateral group. In terms of EVT safety, although ORT was significantly shorter in poor collateral group (272±109 min) than in good collateral group (303±114 min) (p=0.022), the rates of type 2 haemorrhagic transformation, type 2 parenchymal haematoma and mortality were significantly higher in poor collateral group (18.6%, 23.3% and 35.0%) than in good collateral group (8.3%, 5.3% and 4.3%), concordant with previous studies (table 2).25–29
Most current guidelines for acute ischaemic stroke recommend the time window for EVT to be within 360 min after symptom onset.1 2 However, a meta-analysis of five randomised trials has suggested that onset-to-puncture time can be extended to 7.3 hours.4 Among the five randomised trials included in meta-analysis, while mismatch profile by CT perfusion or collateral status on multiphase CTA was considered for patient inclusion criteria in 298 EVT patients (47% of all EVT patients) of three trials, neither collateral status nor mismatch profile was included in the inclusion criteria in 336 EVT patients (53% of all EVT patients) of two trials.3
Therefore, individual patient collateral status was only partly reflected in the suggested time window (7.3 hours) eligible for EVT in the meta-analysis. The results of this study show that, if collateral status is appropriately assessable, time window for EVT may be reset by collateral status. In other words, compared with the recommended current guidelines, time window for EVT may be shortened in those with poor collaterals, whereas it should be extended in good collateral group and may be more than 7.3 hours.
Recently, a randomised clinical trial (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Stroke Undergoing Neurointervention with Trevo, DAWN) proved that EVT time window can be extended beyond 6 hours and up to 24 hours after onset, based on the principle of age-adjusted clinical-core mismatch.30 Another randomised trial (Endovascular Therapy Following Imaging Evaluation for Ischaemic Stroke 3, DEFUSE 3) has succeeded, in which EVT time window can be extended up to 16 hours with selection by perfusion imaging.31 The results of our study are in line with those of DAWN and DEFUSE 3 in suggesting that an exclusive time-based EVT paradigm should be modified based on individual variation in compensatory mechanisms for ischaemia, including collateral flow.30
This study had some strengths and limitations. First, although this was a retrospective study, the study population represented at least a tenth of all real-world patients who received EVT in Korea over the study period, which were inferred from nationwide data of the Health Insurance Review and Assessment Service. In addition, compared with five recent successful randomised clinical trials that measured ASPECTS score, target mismatch profile or collateral status, our study population was evaluated with the same workups of CTA-based collateral status. Second, collateral status was evaluated on single-phase CTA, as this was the method used in most participating centres (93.5% of enrolled patients). As suggested in a previous study, multiphase CTA is likely superior to single-phase CTA in collateral status evaluation.22 Contrast agent filling into cerebral arteries can be insufficient on single-phase CTA due to delayed circulation time relative to CTA scan initiation in an individual patient. To reduce misclassification from good to poor collaterals due to delayed contrast agent filling beyond CTA scan starting time, we only included the cases when vessel markings in the contralateral normal hemisphere were well visualised. Also, to alleviate the difference between single and multiphase CTA, we only used first-phase images for collateral evaluation in patients who underwent multiphase CTA (6.5%); by doing so, excellent inter-rater agreement was obtained. Finally, since we only included patients who fulfilled strict enrolment criteria in our analysis, selection bias might have affected the results. Therefore, the results of this study should be interpreted with caution. A randomised clinical trial is required to confirm the results of this analysis. Nevertheless, the results of this study provide important baseline data for designing a randomised clinical trial to set EVT time window based on CTA collateral status.
Conclusions
Earlier successful recanalisation was strongly associated with good outcome in patients with poor collaterals; however, this association was weak during the tested ORT window in patients with good collaterals. Regression curve of the likelihood of good outcome by ORT showed a significantly faster drop in poor collateral group than in good collateral group. This suggests that collateral status may set the ORT window for good outcome.
References
Footnotes
Contributors BMK had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. BMK, HSN, JHH, JHB and OYB were involved in study concept and design. BMK, OYB and JHB were responsible for drafting a significant portion in the manuscript or figures. All authors were involved in the acquisition and analysis of data.
Funding This research was investigator initiated and supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare of the Republic of Korea (HC15C1056).
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Severance Hospital Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.