Article Text

Abstract
Background and aim: To update our 1996 review on the incidence of subarachnoid haemorrhage (SAH) and assess the relation of incidence with region, age, gender and time period.
Methods: We searched for studies on the incidence of SAH published until October 2005. The overall incidences with corresponding 95% confidence intervals were calculated. We determined the relationship between the incidence of SAH and determinants by means of univariate Poisson regression.
Results: We included 51 studies (33 new), describing 58 study populations in 21 countries, observing 45 821 896 person-years. Incidences per 100 000 person-years were 22.7 (95% CI 21.9 to 23.5) in Japan, 19.7 (18.1 to 21.3) in Finland, 4.2 (3.1 to 5.7) in South and Central America, and 9.1 (8.8 to 9.5) in the other regions. With age category 45–55 years as the reference, incidence ratios increased from 0.10 (0.08 to 0.14) for age groups younger than 25 years to 1.61 (1.24 to 2.07) for age groups older than 85 years. The incidence in women was 1.24 (1.09 to 1.42) times higher than in men; this gender difference started at age 55 years and increased thereafter. Between 1950 and 2005, the incidence decreased by 0.6% (1.3% decrease to 0.1% increase) per year.
Conclusions: The overall incidence of SAH is approximately 9 per 100 000 person-years. Rates are higher in Japan and Finland and increase with age. The preponderance of women starts only in the sixth decade. The decline in incidence of SAH over the past 45 years is relatively moderate compared with that for stroke in general.
Statistics from Altmetric.com
Subarachnoid haemorrhage (SAH) from a ruptured aneurysm accounts for approximately 5% of all strokes. Because it occurs at a young age and has a high case fatality, the loss of productive life years in the general population from SAH is as large as that from cerebral infarction, the most common type of stroke.1 2 Important risk factors are a familial preponderance, hypertension, smoking and alcohol abuse.3 In 1996, we performed a systematic review on the incidence of SAH between 1960 and 1994.4 In that review, the incidence of SAH had remained stable at around 8 per 100 000 person-years over 35 years. An interesting finding was the high incidence in Finland in comparison with other European and American populations. In a small subset of studies, gender specific incidences were given, which indicated a higher incidence in women.
Since the publication of that review, many new incidence studies have been reported, including regions that were not represented in the first review. The incidence for stroke in general has declined over the past decade, and this has been attributed to a declining proportion of people who smoke and to better detection and treatment of hypertension.1 As smoking and hypertension are also risk factors for SAH, a similar decline in the incidence of SAH could be expected. We updated the previous review with new information and assessed regional differences in SAH incidence, as well as differences in incidence according to age, gender and time period.
METHODS
Methods of literature search, inclusion criteria for studies and diagnostic criteria for SAH were essentially the same as in the previous overview.4 To update the review, we searched for population based studies on the incidence of SAH by performing a MEDLINE search from 1993 until October 2005. (Keywords: “stroke” or “subarachnoid haemorrhage” together with “epidemiology”, “population” or “incidence”.) In addition, we searched the reference lists of all relevant publications, searched for related articles given on MEDLINE and checked the citation list of all references found, including those from the previous version of the review. This method of cross checking was continued until no further new studies were found. The list of references thus found was compared with the personal database of references from another author (GJER) to check if references had been missed by the (retrospective) PubMed search (which was not the case). This personal database has been prospectively built by daily search of PubMed over the past 10–15 years by means of the following terms “subarachnoid hemorrhage [All Fields] OR aneurysm [All Fields] OR arteriovenous malformation [All Fields] OR perimesencephalic [All Fields] OR subarachnoid haemorrhage [All Fields] OR aneurysm*”.
Two authors (NKR and JAP) reviewed all eligible studies independently and completed a data extraction form. These forms included items regarding design of the study, study population, case finding and diagnostic criteria of SAH. The inclusion criteria were: (1) prospective design; (2) study population is representative of the population in general; (3) upper age limit for the study not below 75 years and lower age limit not above 25 years; (4) for studies about stroke in general, SAH should be considered as a separate entity; (5) results include or at least allow calculation of the overall crude incidence of SAH; (6) the majority of cases were reviewed by the study investigator; (7) case finding methods include at least involvement of all hospitals in the region, and either involvement of general practitioners or reviewing death certificates during the study period; and (8) diagnostic criteria include at least lumbar puncture or autopsy in the pre-CT era, or in case the proportion of patients investigated with CT was lower than 90%. In the event of disagreement in the data extraction forms, the article was re-read by another author (GJER or FHHL) and discussed until agreement was achieved. Excellent case finding was defined as involvement of all hospitals in the region as well as involvement of general practitioners and reviewing death certificates during the study period. Excellent diagnostics was defined as more than 90% of SAH patients had undergone CT.
We used incidence rates relating to the entire population, without adjustment for age or sex. Authors were contacted for missing data on crude incidence of SAH if necessary. To assess geographical differences, we compared studies by region. In addition, we extracted gender and age specific incidence rates for those studies that provided sufficient data.
Data analysis
For each of the selected studies, the overall incidence was computed if necessary. Ninety-five per cent confidence intervals were calculated with Poisson methods. We determined the relationship of the incidence of SAH with region, age, gender and time period by means of univariate Poisson regression. Incidences by region were calculated with the subset of studies from the specific area. Relationship of incidence of SAH with age and gender was analysed using demographics of the study populations, and age and gender specific incidences of SAH were calculated with the subset of studies that provided sufficient data. Time trend was analysed using midyear of the study, taking into account regional differences. Multivariate Poisson regression was used to asses the independent contribution of age, gender and time trend to SAH incidence. To examine the influence of design of the study, we selected a subset of studies with excellent case finding and excellent diagnostic criteria for sensitivity analysis.
RESULTS
Literature search
The literature search resulted in 42 new studies (fig 1).5–46 Thirty-three were relevant for overall analysis. The remaining nine studies were not included in the overall analyses because only incidences of limited age categories were provided.6 14–16 19 28 32 34 38 These nine studies were included only for analysis on age specific incidences. Eleven authors were contacted for missing information; in four cases the information was retrieved.14 15 39 45 Together with the 18 investigations from the previous review,47–64 51 studies were used in the total analysis. As four studies provided incidences for 2, 3 or 4 periods or areas,17 27 39 55 the number of study periods and study regions that we analysed was 58, of which 39 were new. The studies covered populations in 21 countries with 45 821 896 person-years of observation.

Calculated incidences, case finding methods and diagnostic criteria from all of the included study periods and regions are summarised in table 1. Table 2 represents the nine studies describing study populations with limited age categories.
Region
There was wide variation in SAH incidence, ranging from 2 to 25 per 100 000 person-years, with most regional incidences between 7 and 13 per 100 000 person-years. We defined all countries other than Japan, Finland and South or Central America as the reference group. Overall incidences were 9.1 (95% CI 8.8 to 9.5) per 100 000 person-years in the reference group (42 studies); 22.7 (95% CI 21.9 to 23.5) in Japan (seven studies); 19.7 (95% CI 18.1 to 21.3) in Finland (six studies); and 4.2 (95% CI 3.1 to 5.7) in South and Central America (three studies) (fig 2). The incidence in Japan was 2.5 (95% CI 2.4 to 2.6) times higher than that of the reference region and in Finland 2.2 (95% CI 2.0 to 2.4) times higher, whereas the incidence in South and Central America was 2.2 (95% CI 1.6 to 2.9) times lower.

Age
The mean age of the study population was mentioned in 37 studies, and univariate Poisson regression analysis was performed for this subset of studies. In populations with a mean age of 35 years, calculated incidence was 8.6 (95% CI 8.0 to 9.2), and for every year of increase in mean age, the incidence was 1.06 times higher (95% CI 1.05 to 1.07).
Twenty studies, including the nine studies with only age specified subsets of the population, reported separately on incidences per age group.5 6 8–10 16 18–20 22 27 36 45 49 50 52 54 57 60 64 The overall incidence of these 20 studies was 13.9 (95% CI 13.3 to 14.5) per 100 000 person-years. In this subset, incidence increased with age: taking age 45–55 years as the reference category, incidence ratios increased from 0.10 (95% CI 0.08 to 0.14) for age <25 years, to 1.61 (95% CI 1.24 to 2.07) for ⩾85 years (table 3).
For Japan, incidences per age decade were given in two studies. Based on these two studies, increase in age specific incidence seemed to be steeper in Japan than in other regions, ranging from 0.56 (95% CI 0.18 to 1.75) per 100 000 person years for age <25 years to 7.96 (95% CI 5.33 to 11.88) for ⩾85 years. For Finland, no age specific incidence per age decade was available for analysis, and for South and Central America, numbers were too small to provide reliable estimates.
Age adjusted incidences per 100 000 person-years in Japan varied from 21 (95% CI 18 to 24) to 23 (95% CI 19 to 28),23–27 and in Finland from 14 (95% CI 10 to 19) to 30 (95% CI 22 to 40).17 58 From studies in South and Central America, age adjusted incidence was given in only one study (4; 95% CI 2 to 6 per 100 000 person-years), which was also adjusted for sex.9
Gender
Gender distribution was provided in 37 studies. Univariate Poisson regression analysis showed that for each additional per cent of women, the incidence became 1.07 times higher (95% CI 1.04 to 1.10).
Eighteen studies reported incidences for men and women separately.5 9 10 17 18 20 22 27 29 35 44 45 47 49 50 52 54 57 The overall incidence in this subset of studies was 10.5 (95% CI 9.9 to 11.2) per 100 000 person-years; the incidence for men was 9.2 (95% CI 8.4 to 10.2) and for women 11.5 (95% CI 10.6 to 12.6). Thus the incidence in women was 1.24 (95% CI 1.09 to 1.42) times higher than in men. Separate women–men ratios per region were 1.26 (95% CI 1.03 to 1.52) for the reference region, 1.16 (95% CI 0.95 to 1.42) for Japan, 1.58 (95% CI 1.08 to 2.30) for Finland and 0.89 (95% CI 0.32 to 2.47) for South and Central America.
Age and gender
In the 37 studies that reported mean age of the study population and gender distribution, mean age and proportion of women were analysed by multivariate analysis. After adjustment for age, incidence increased by a factor of 1.03 (95% CI 0.99 to 1.06) for each additional percentage point of women in the study population. After adjustment for gender, incidence increased by a factor of 1.06 (95% CI 1.05 to 1.07) for each additional year.
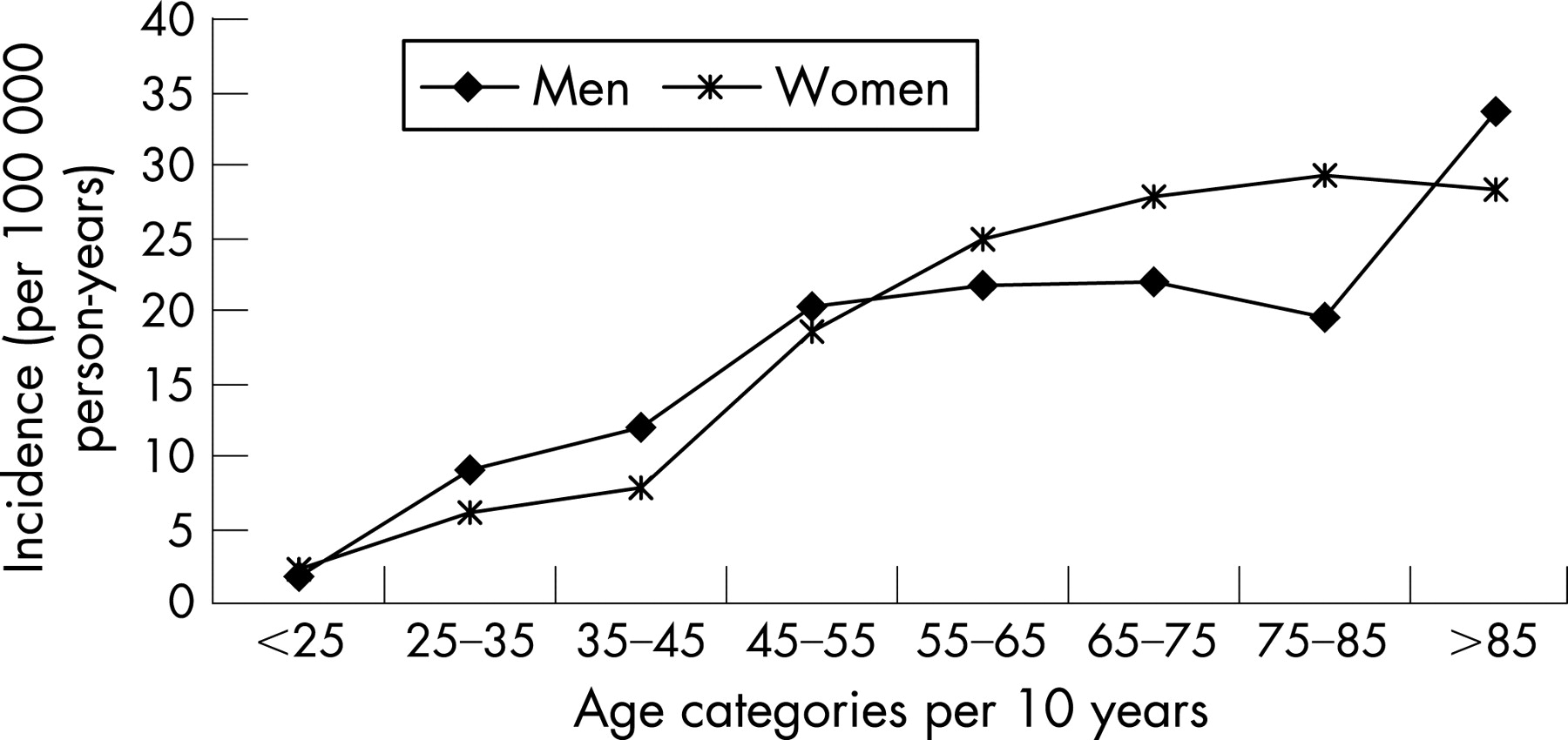
Incidences were reported separately for women and men by age category in 16 studies.5 6 9 10 16 18–20 22 27 45 49 50 52 54 57 In this subset of studies, the women–men ratio ranged from 0.65 (95% CI 0.51 to 0.82) to 1.50 (95% CI 1.07 to 2.10). In the age group 25–45 years, incidence was significantly higher in men than in women, but in the age group 55–85 years, incidence was significantly higher in women than in men (table 3, fig 3).

{kind=link}
{kind=link}
{kind=link}
Time trend
Midyear of the study was analysed by univariate and multivariate analysis for evaluation of a time trend. Because studies in Japan and Finland were confined to more years, analyses on time trend were performed for the reference region only. During the observation period, incidence decreased by a factor of 0.994 (95% CI 0.987 to 1.001) per year in the reference region after adjustment for gender and age. When all 42 studies were analysed from the reference region without adjustment for age and gender, the rate ratio was 1.001 (0.997 to 1.004) for year-to-year annual change, thus showing no decrease in incidence. In the subset of studies that reported on study periods after 1990 and that provided exact proportions of patients investigated by CT, the rate ratio for use of CT on reported incidence was 0.997 (95% CI 0.993 to 1.002) in the reference region (n = 14), 0.963 (95% CI 0.908 to 1.022) in Japan (n = 4) and 0.963 (0.821 to 1.13) in South and Central America (n = 3). Thus after 1990 there was no obvious relation between the use of CT and reported incidence of SAH. To exclude the influence of percentage of CT use, separate analyses were performed including only studies after 1990. For this subset of 24 studies after 1990 from the reference region, results were essentially the same after adjustment for age and gender (table 4).
Sensitivity analysis
The criterion for excellent case finding was met by 33 studies (20 new, 13 from the previous review) and the criterion for excellent diagnostics by seven studies (five new, two from the previous review). If we combine both “excellent” case finding methods and “excellent” diagnostic criteria, none of the studies fulfilled these criteria. Therefore, we were unable to perform a sensitivity analysis with excellent studies.
DISCUSSION
We found that wide variation exists in the incidence of SAH. The overall incidence of SAH was approximately 9 per 100 000 person-years but varied significantly by region, with doubled rates in Japan and Finland and far lower rates in South and Central America. The incidence was higher in women and increased with age. The gender distribution varied with age. At young ages, incidence was higher in men, while after the age of 55 years, the incidence was higher in women. The incidence of SAH has probably decreased slightly over the past 45 years.
Several factors may contribute to the higher incidence in Finland and Japan, but the extent of their contributions remains speculative. In Japan and Finland, a higher risk of rupture of intracranial aneurysms is described.65 Genetic factors may also play an important role in both Japan and Finland.
The relatively older age in Japan may be another explanation. Global statistics report the Japanese as being the oldest population in the world, with a median age of 43 years in 2005.66 However, this older age cannot entirely explain the high incidence, because age specific incidences were also higher in Japan than in the reference population. Another explanation may be better case finding, but case finding in the studies from Japan was not more exhaustive than in other regions. Five of the seven studies did not describe regular contacts with general practitioners, and none mentioned contacting rehabilitation facilities or nursing homes as a case finding method. However, the majority of studies from Japan examined instances of sudden death more extensively than studies from other regions. Most studies from Japan used in addition to autopsy, neuroimaging of patients who had died suddenly or during transportation to the hospital. Probably more patients dying early after SAH were detected by scrutinising all of these events, which increased the incidence of SAH compared with studies in which such instances of sudden death were not examined in this way. However, sudden death accounts for only 12% of all SAH patients67; more extensive examination of patients dying early may contribute to, but cannot entirely explain, the higher incidence in Japan. The proportion of patients in whom the diagnosis of SAH was confirmed by CT scanning was almost 100% in Japan. However, a large proportion of patients investigated by means of CT does not lead to a higher incidence. In our previous review, we found a higher percentage of CT use to be associated with a lower incidence of SAH and in recent studies we found no relation between the proportion of patients investigated by means of CT and the reported incidence. The greater use of neuroimaging in Japan is therefore unlikely to be an explanation for the high incidence rates reported in Japan.
Age adjusted incidences were also higher in Finland than in the reference region. In Finnish studies, the proportions of patients in whom the diagnosis of SAH was confirmed by CT were low (varying between 0% and 60%). If we apply the rate ratio for proportion investigated by CT on incidence found in the previous version of the review, and if we assume a hypothetical 100% proportion of patients investigated by CT, the incidence of SAH would be 10.6 (95% CI 8.9 to 12.5) in Finland, which is still higher than the incidence in the reference region. Thus the low proportions of CT in Finnish studies do not entirely explain the higher incidences found. Case finding methods in Finnish studies were not more exhaustive compared with other studies, thereby not increasing the incidence found. Other explanations for the high incidence in Finland include high prevalence of smoking and hypertension,68 and heavy episodic alcohol abuse.69
The low incidences in South and Central America can perhaps be explained in part by the relatively young mean age of people in these regions. Reported mean ages in the study populations varied between 25 and 35 years, whereas for the reference population this mean age was 37 years. However, the age adjusted incidence given in one study was also lower than in the reference region.9 Thus other factors are likely to be involved in the lower incidence in this region. No differences in case finding methods were noted, but access to hospitals in these regions may be less than in other regions. Another explanation might be racial differences, although in some studies the incidence of SAH in black populations was higher in comparison with white populations.70
In summary, none of these explanations can completely explain the regional differences, and other factors are likely to be involved.
The higher incidence of SAH in women was found in the previous version of our review but the age dependent gender difference is a new finding. While previous literature describes a peak incidence in the sixth decade,71 some recent studies found a continuous increase with age, or an age dependent gender difference.6 The current review confirms these observations from some individual studies. The reasons for the overall higher incidence in women are not clear, but hormonal factors (including use of hormone replacement therapy) are a possible explanation.72 73 Our finding that the preponderance of women starts only after the sixth decade further supports this suggestion.
Although several studies have reported a statistically significant decline in stroke of approximately 2% per year over the past two decades,12 74 75 it is still uncertain if the reduction in cardiovascular risk factors has also translated into a reduction in the incidence of SAH. Our study found a decrease in incidence of 0.6% per year, which is modest compared with the decline in stroke in general. In our analysis, the influences of region, age, gender and improved diagnostic criteria by CT were taken into account. In our previous review, we found that the apparent decline in the incidence of SAH until 1990 was entirely explained by the increasing proportion of patients investigated by CT.4 In this update, we found that in studies performed after 1990, the proportion of patients investigated by means of CT was no longer significantly related to incidence in any region. The most likely explanation is that after 1990, almost all hospitalised patients were investigated using CT. Thus the contrast between studies with small proportions investigated by CT (with over reporting of SAH)76 and studies with large proportions investigated by CT has disappeared. The time trend found in our study is therefore not explained by percentages of CT use for confirmation of diagnosis of SAH. The small magnitude of the decline in incidence of SAH may in part be explained by the stronger influence of genetic factors in SAH than in stroke in general.77 However, genetic factors explain only 10% of SAH, and most cases are attributed to smoking, hypertension and excessive use of alcohol.77 Perhaps the reduction in risk factors is more effective in older people (where most stokes in general occur) than in younger people (who are most at risk of SAH), but we have no data to support this hypothesis.
It seems contradictory that the incidence of SAH decreased over time, although the overall incidence in our update was higher than the incidence found in our previous review. However, by updating the review, we included five new studies in the reference region published after 1993 presenting data from before 1990. These five studies had a combined incidence of 10.4 per 100 000 person-years, which is higher than the overall incidence from the studies that had been included in the previous version of the review. The net result is that the incidence of all studies (including the newly found ones) for the observation period from the previous review (1972–1990) has increased compared with that in the previous review. This effect in part explains the paradox of higher incidence in the current review despite declining incidence over time. Furthermore, we found the decrease in incidence only after adjustment for gender and age. Thus the increased incidence in the updated version of the review may be explained in part by inclusion of study populations with higher ages in the more recent years.
The number of population based studies (51) and number of person-years (45 821 896) included in this review was large and therefore overall estimates are precise. Subgroup analyses according to region, age, gender and time trend were based on smaller numbers of studies and person-years. Nevertheless, even for these analyses, CI values were narrow. This current review also included data from additional parts of the world compared with the previous version; only African, South Asian and Chinese populations were not represented.
Our study shows that the incidence of SAH has declined over the past decades, although to a lesser extent than that of stroke in general. Moreover, incidence continues to increase until older age, is higher in women than in men only after the fifth decade and varies considerably per region. Further studies should address the reasons for the relative moderate decline in incidence of SAH, the higher incidence in women only after the fifth decade and the regional differences in SAH incidence. The answers to these questions will probably provide further clues to the aetiology of SAH.
REFERENCES
Footnotes
Competing interests: None.
- Abbreviations:
- SAH
- subarachnoid haemorrhage