Cauda equina syndrome
BMJ 2009; 338 doi: https://doi.org/10.1136/bmj.b936 (Published 31 March 2009) Cite this as: BMJ 2009;338:b936
- Chris Lavy, honorary professor and consultant orthopaedic surgeon,
- Andrew James, specialist registrar,
- James Wilson-MacDonald, consultant spine surgeon,
- Jeremy Fairbank, professor of spine surgery
- Correspondence to: C Lavy christopher.lavy{at}ndos.ox.ac.uk
Summary points
Cauda equina syndrome is rare, but devastating if symptoms persist
Clinical diagnosis is not easy and even in experienced hands is associated with a 43% false positive rate
The investigation of choice is magnetic resonance imaging
Once urinary retention has occurred the prognosis is worse
Good retrospective evidence supports urgent surgery especially in early cases
Litigation is common when the patient has residual symptoms
An understanding of cauda equina syndrome is important not only to orthopaedic surgeons and neurosurgeons but also to general practitioners, emergency department staff, and other specialists to whom these patients present. Recognition of the syndrome by all groups of clinicians is often delayed as it presents with bladder, bowel, and sexual problems, which are common complaints and have a variety of causes. Patients may not mention such symptoms because of embarrassment or because the onset is slow and insidious.
Cauda equina syndrome is a clinical area that attracts a high risk of litigation. Although symptoms have poor predictive value on their own for the syndrome, it is important to document the nature and timing of bladder, bowel, and sexual symptoms (along with any associated clinical findings), particularly if they are new, especially in those with a history of back pain and associated leg pain, and to make a timely referral for appropriate investigation and expert treatment.
This review aims to highlight cauda equina syndrome as a possible clinical diagnosis, review the evidence for an emergency surgical approach, and maintain an awareness of the medicolegal issues that surround the condition.
What is cauda equina syndrome and how common is it?
Cauda equina syndrome results from the dysfunction of multiple sacral and lumbar nerve roots in the lumbar vertebral canal. Such root dysfunction can cause a combination of clinical features, but the term cauda equina syndrome is used only when these include impairment of bladder, bowel, or sexual function, and perianal or “saddle” numbness.1 2 (box)
Clinical diagnosis of cauda equina syndrome
Dysfunction of bladder, bowel, or sexual function
Sensory changes in saddle or perianal area
Other possible symptoms
Back pain (with or without sciatic-type pains)
Sensory changes or numbness in the lower limbs
Lower limb weakness
Reduction or loss of reflexes in the lower limbs
Unilateral or bilateral symptoms
A retrospective review in Slovenia found an annual incidence of cauda equina syndrome resulting from intervertebral disc herniation of 1.8 per million population.3 Using US data on annual incidence of symptomatic disc herniation (1500 per million population), the author estimates that each year 0.12% of herniated discs are likely to cause cauda equina syndrome. We suspect this is an underestimate and are conducting our own review in the United Kingdom, but if these figures are even approximately correct then most UK general practitioners are unlikely to see even one true case caused by intervertebral disc herniation in their career.
How does cauda equina syndrome present and what symptoms suggest it?
A history of perianal sensory loss and sphincter disturbance, with or without urinary retention, suggests the presence of cauda equina syndrome (figure 1⇓ illustrates the anatomy of the lower lumbar and sacral spine showing the cauda equina). Three classic patterns of presentation have been described.4 It can present acutely as the first symptom of lumbar disc herniation (type 1); as the endpoint of a long history of chronic back pain with or without sciatica (type 2); or insidiously in a more chronic way with slow progression to numbness and urinary symptoms (type 3). Most clinicians now divide cauda equina syndrome into two clinical categories4: cauda equina syndrome with retention, in which there is established urinary retention; and incomplete cauda equina syndrome, in which there is reduced urinary sensation, loss of desire to void, or a poor stream, but no established retention or overflow.5 Often the slower the presentation, the better tolerated the symptoms are and the less likely the patient is to be alarmed. Patients with pre-existing bladder and incontinence problems resulting from other disease may also present late.
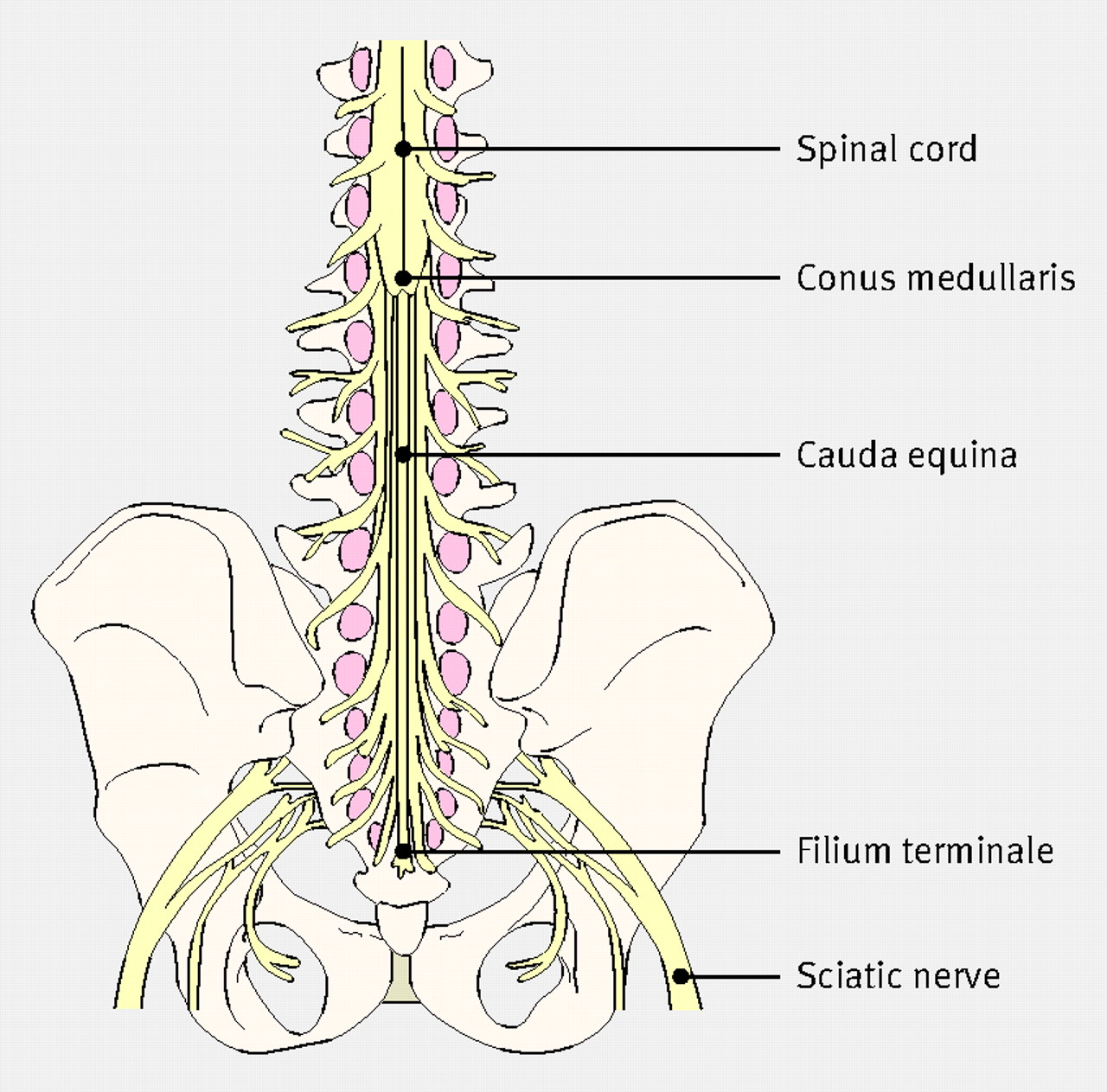
Fig 1 Anatomy of the lower lumbar and sacral spine showing the cauda equina
{kind=link}
What causes cauda equina syndrome?
The commonest cause of cauda equina syndrome in our practice and the focal causative condition in the literature6 is compression arising from large central lumbar disc herniation at the L4/5 and L5/S1 level. Parke and colleagues suggest that there is an area of relative hypovascularity at the proximal portion of the cauda equina.7 Blood supply alterations resulting from nerve root pressure may therefore be of greater importance in this region of the cauda equina than elsewhere, with rapid changes allowing less adaptation than those of a slower onset.
Patients may be predisposed to cauda equina syndrome if they have a congenitally narrow spinal canal or have acquired spinal stenosis arising from a combination of degenerative changes of the disc and the segmental posterior joints with consequent thickening of the ligamentum flavum and narrowing of the available canal cross section.
Numerous other less common causes of cauda equina syndrome have been reported—for example, spinal injury with fractures or subluxation. Spinal neoplasms of metastatic or primary origin can cause compression, usually accompanied by marked pain and often as part of a chronic condition. Infective causes with abscess formation or bony involvement, either within the spinal canal or impinging on it, may also cause cauda equina syndrome.8 The spine is the most commonly affected skeletal site for tuberculosis, and Pott’s paralysis is well documented.9 A wide range of iatrogenic causes are reported, including manipulation,10 spinal anaesthesia,11 postoperative complications such as haematoma12 or gelfoam implanted to protect the dura. Other space-occupying lesions, such as nerve derived tumours, schwannomas, ependymomas, facet joint cysts,13 perineural Tarlov cysts, haemangiomas,14 vena varix,15 and hydatid cysts 16 are also recognised.
What features on examination suggest cauda equina syndrome?
When cauda equina syndrome is suspected a neurological examination of the legs should be performed, including perianal sensation and an assessment of anal tone (table⇓). This is easily done in the lateral position: perineal sensation can be tested from the outside in towards the sphincter using a gentle gloved finger stroke and, if there is any uncertainty, a folded tissue and an unfolded paper clip. After this, a rectal examination can be performed. Loss or diminution of the bulbocavernosus reflex (whereby stimulation of the glans, penis, or clitoris causes reflex contraction of the anal sphincter) is suggestive of cauda equina syndrome as the reflex is mediated through the sacral roots.
Motor sensory and reflex components of lumbar and sacral roots
How should suspected cauda equina syndrome be investigated?
Recently published guidelines for the management of patients with back pain and neurological signs recommend urgent surgical referral for suspected cauda equina syndrome.17 Clinical diagnosis of cauda equina syndrome even by resident neurosurgeons has a 43% false positive rate,18 so accurate confirmatory imaging is important. In the United Kingdom magnetic resonance imaging (MRI) is the imaging modality of choice. It does not define bone as clearly as computed tomography (CT) but is better at showing soft tissues such as intervertebral disc, ligamentum flavum, dural sac, and nerve roots. In resource poor settings where neither MRI nor CT is available myelography can be useful in showing the presence and site of compression of the cauda equina.19 Figures 2⇓ and 3⇓ show examples of cauda equina on MRI scans.

Fig 2 Left: MRI scan showing compression of the cauda equina (arrow) due to a large posterior disc herniation at L4/5. Right: MRI scan showing a large disc herniation at L5/S1 (arrow) bulging posteriorly and compressing the cauda equina syndrome
{kind=link}

Fig 3 Top: Axial cross sectional MRI view at the level of L5/S1 of a patient with cauda equina syndrome showing a large irregular disc herniation (arrow) occupying most of the vertebral canal. Bottom: By contrast, a cross sectional MRI view at L5/S1 in a patient without cauda equina syndrome showing an unobstructed vertebral canal (arrows from top down: body of S1 vertebra; vertebral canal containing cauda equina with no compression; spine of S1)
{kind=link}
How is cauda equina syndrome treated?
When a patient has clinical features of cauda equina syndrome and an MRI scan shows a potentially reversible cause of pressure on the cauda equina then current consensus recommends surgical decompression.6 This article will not review management of all the conditions leading to cauda equina syndrome, and some causes such as tumour clearly require detailed assessment of the nature and extent of the pathology. However, most cases of cauda equina syndrome are caused by herniation of the lumbar disc, for which the surgery indicated is decompression at the level of the herniation, usually involving discectomy. The operation can be very demanding technically, and great care is needed to avoid causing further damage to nerve roots or tearing tightly compressed dura.
Is surgery for cauda equina syndrome urgent?
The urgency of surgery remains controversial. When there is pressure on the cauda equina causing loss of sphincter control it would be understandable to think that the ideal treatment would be to remove the pressure as soon as possible with surgery. Ethical considerations will not allow this hypothesis to be tested by a randomised study, and it is very difficult to prove by literature review of retrospective and cohort studies (level 3 evidence) for two reasons. Firstly, the time of onset of symptoms is difficult to specify. Thus it is difficult to define the delay between symptoms and surgery. Secondly, any discussion is muddied by many published (mainly retrospective) series containing a mix of patients with both incomplete cauda equina syndrome and cauda equina syndrome with retention.
The authors of two recent reviews20 21 argue that only incomplete cauda equina syndrome requires emergency surgery to try to stem the deterioration in bladder function. They conclude that in patients with cauda equina syndrome with retention the clinical outcome is poor anyway and bears no relation to timing of surgery. Thus these patients can wait until an elective surgical list the next morning rather than having a potentially difficult operation in the middle of the night, when circumstances are less than optimal.
Two other recently published UK series22 23 have found that outcome is independent of the timing of surgery. Incontinence at presentation is a poor prognostic feature in the largest prospective series.23
A review that is widely quoted suggests that intervention less than 48 hours after the onset of symptoms will produce a better outcome than intervention delayed for longer than this.6 These data have been selectively reanalysed24 and suggest that the outcome for both types of cauda equina syndrome (with retention, or incomplete) is better with interventions within rather than after 24 hours. In a further analysis of the selected retrospective series, the authors noted that of 47 patients having surgery within 24 hours, 41 (87%) recovered normal bladder function, whereas of 46 patients having surgery later than 24 hours, only 20 (43%) recovered normal bladder function.25
A recent meta-analysis supports the view that early surgery is related to better results with incomplete cauda equina syndrome, but the case for cauda equina syndrome with retention is less certain.4 We urge the establishment of a multicentre outcome study with clear clinical entry points and clear separation of incomplete cases and those with retention.
What are the medicolegal implications of cauda equina syndrome?
Persisting cauda equina syndrome has a devastating effect on personal and social life, and its mismanagement is one of the commonest causes for litigation in spinal surgery. Most patients are young to middle aged and in work before they develop cauda equina syndrome, so the size of claims is large. The presence of residual symptoms means that many of these patients are unable to work and have genitourinary and bowel symptoms. From 1997 to 2006 the NHS Litigation Authority dealt with 107 cases in England in which care in hospital had been compromised (NHS Litigation Authority, personal communication, 2008). Extrapolating from previous data,3 we would expect about 100 new cases of cauda equina syndrome annually in England, suggesting that at least 10% of cases involve litigation. The NHS Litigation Authority reported that between 1997 and 2006 in 35% of litigation cases the primary complaint was against the emergency department and in 52% it was against the inpatient management team (personal communication as above). In the remaining cases the primary complaints were against other clinical areas, such as outpatients. The responsible clinician in the litigation cases was in orthopaedics in 52% of cases, the emergency department in 27%, and neurosurgery in 8%; in the remaining cases the responsible clinician varied across various specialties.
JF and JW-MacD have prepared 22 medical negligence reports in cases of cauda equina syndrome over the past five years. The average delay to diagnosis was 67 hours and to treatment 6.14 days. These delays were attributed to orthopaedic surgeons in 32% of cases, general practitioners in 18%, and others in 14%, but in 34% of cases there was no clear case to answer. Fourteen per cent of patients had received their treatment within 24 hours and 32% within 48 hours. All patients had moderate or severe bowel and genitourinary symptoms. Most also had persisting back pain that would probably have occurred whatever the timing of surgery. Doctors who manage patients with spinal disorders need to be aware of cauda equina syndrome and its possible complications.
Sources and selection criteria
We searched Medline using the search term “cauda equina syndrome”. In addition, we used our personal reference archives and consulted other experts.
Questions for future research
Multicentre outcome studies are needed to define which subgroups of cauda equina syndrome may benefit from emergency surgery and which do not need such urgent treatment
Such studies may also develop prognostic indicators such as the length and degree of compression of the cauda equina
Qualitative research is needed to determine appropriate questions and appropriate language to inquire about sensation in intimate areas
Tips for non-specialists
Be alert to the development of new symptoms of perianal sensory change or bladder symptoms in patients with an increase in back pain or sciatica
Be aware that cauda equina syndrome can arise insidiously when patients who have had back and leg pain for a long time develop bladder symptoms gradually
Establish the most appropriate channel for referral or further investigation in suspected cases in your specialty
Make sure that clinical documentation is clear and well recorded
Additional educational resources*
Cauda Equina Syndrome Resource Center (www.caudaequina.org)—Support group for people with cauda equina syndrome to share information about the condition
BackPainExpert (www.backpainexpert.co.uk/CaudaEquinaSyndrome.html)—Patient information site with articles written by invited experts
Wikipedia (http://en.wikipedia.org/wiki/Cauda_equina)—Part of the online editable encyclopedia wikipedia; anyone may post comments or make changes
Cauda Equina (http://orthoinfo.aaos.org/topic.cfm?topic=A00362)—Information on the website of the American Academy of Orthopaedic surgeons
*All these websites are free and do not need registration
A patient’s perspective
I wasn’t that concerned at first. I had just sneezed. I hadn’t even lifted anything heavy. The sudden, searing lower back pain was unpleasantly familiar to me and it usually got better by itself. I didn’t notice anything unusual until I started to get pins and needles in both my feet. And then, after painfully struggling to the toilet, I remember wiping myself with the toilet paper and it feeling decidedly odd—not completely numb but distant. It was my refusal to admit to numbness that fooled my general practitioner. He asked if I could feel him touching me, not whether his touch felt normal. He organised an urgent outpatient referral for three days later. Foolishly I just waited, not reporting the progressive loss of sensation, muscle fasciculation, creeping incontinence, and onset of a deep burning pain around my perineum. Unable to arrange ambulance transfer, a friend took me to the hospital lying in the back of his estate car. Within 90 minutes of arrival I had had an MRI scan and was in theatre undergoing an L4/5 discectomy. Two days later, the postoperative anxiety was replaced by euphoria when I managed to stand unaided and pass urine into a bottle.
Notes
Cite this as: BMJ 2009;338:b936
Footnotes
We acknowledge the help of our departmental colleagues in preparing this clinical review, in particular James Teh, Gavin Bowden, Nas Qureshi, Adi Zubovitch, David McKenna, David Mant, Elaine Buchanan, and Louise Hailey.
Contributors: This article was suggested after discussion at a departmental audit meeting. All authors contributed to the research and writing. CL is the guarantor.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent obtained.