Article Text

Statistics from Altmetric.com
Neuropathological changes of carbon monoxide (CO) poisoning include the pallidoreticular pattern of brain damage1consisting of bilateral necrosis of the globus pallidus and substantia nigra. We here report brain MRI of a CO poisoning victim that showed bilateral lesions of the globus pallidus and substantia nigra. This is the first neuroimaging demonstration of the pallidoreticular pattern of brain damage in a patient with CO poisoning.
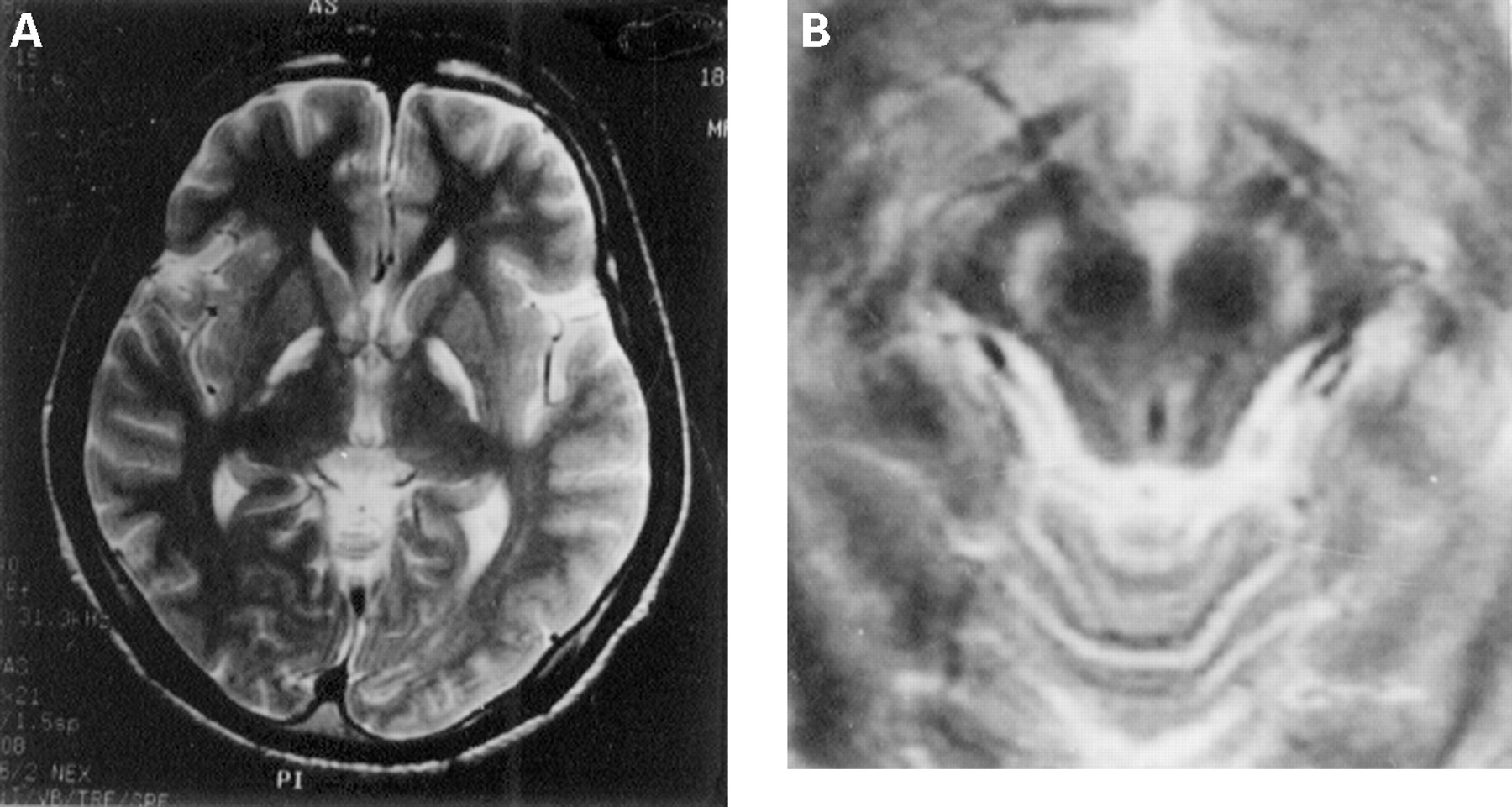
A 17 year old previously healthy man was found unconscious in a bathroom. He was transferred to an emergency room and diagnosed as having CO poisoning due to faulty ventilation. Hyperbaric oxygen therapy improved his consiousness from coma to being fully alert. However, he had parkinsonism. Severe akinesia was noted although there was no tremor or rigidity of the limbs. Additional hyperbaric oxygen therapy for six months did not improve his neurological deficit. Brain MRI, a year after CO exposure, disclosed bilateral pallidal lesions: the globus pallidus appeared streaked with a decreased signal intensity on T1 weighted images and an increased signal intensity on T2 weighted images (figure A). Also noted was an increased signal intensity of the substantia nigra on T2 weighted images (figure B). There was otherwise no alteration on brain MRI. A CSF examination showed a decrease in homovanillic acid concentration to 5.9 ng/ml (normal range 28.83–54.28 ng/ml) with normal values of CSF protein and sugar concentrations and normal cell counts.
{kind=link}
(A) Axial T2 weighted MRI at the level of the basal ganglia. The globus pallidus shows an increased signal intensity. (B) Axial T2 weighted MRI of the midbrain. The substantia nigra shows an abonrmally high signal intensity.
Auer and Benveniste1 described the pallidoreticular pattern of brain damage in necropsied cases of CO poisoning. They speculated that the iron rich regions could be affected by binding of CO to iron molecules. In our patient, bilateral pallidal lesions on MRI were consistent with necrosis because of MR signal features. A decreased concentration of homovanillic acid in the CSF2and an increased signal intensity of the substantia nigra on T2 weighted images seem to be due to neuronal loss and gliosis in the substantia nigra.
The pallidoreticular pattern of brain damage1 to our knowledge has not been reported on MRI in patients with CO poisoning. We emphasise the possible involvement of the substantia nigra in some victims of CO poisoning. In those patients, parkinsonism would be explained partly by neuronal loss in the substantia nigra in addition to the bilateral pallidal necrosis.3