Article Text

Statistics from Altmetric.com
Pituitary apoplexy is an uncommon, but well recognised clinical syndrome, which usually results from ischaemic or haemorrhagic necrosis of a pituitary adenoma.1 It is characterised by the abrupt onset of severe headache, visual impairment, ophthamolplegia and often, a deteriorating level of consciousness.2 Signs of meningeal irritation are frequent accompaniments, which may confuse the clinical picture with that of aneurysmal subarachnoid haemorrhage (SAH). We report a case of massive SAH caused by pituitary apoplexy and present the CT and MRI findings.
A 72 year old woman, with nothing in her history to suggest pituitary dysfunction, presented with the abrupt onset of severe headache, vomiting, and gradually deteriorating level of consciousness. A CT examination of the brain without contrast enhancement showed an extensive basal subarachnoid haemorrhage that had diffused into both sylvian fissures and into the sulci over the convexity of the cerebral hemispheres. In addition there was a rounded heterogeneous density mass in the suprasellar cistern (fig 1 A). After the administration of contrast material the lesion displayed heterogeneous central enhancement (fig 1 B.) A ruptured anterior communicating aneurysm was suspected but was excluded by normal cerebral angiography.
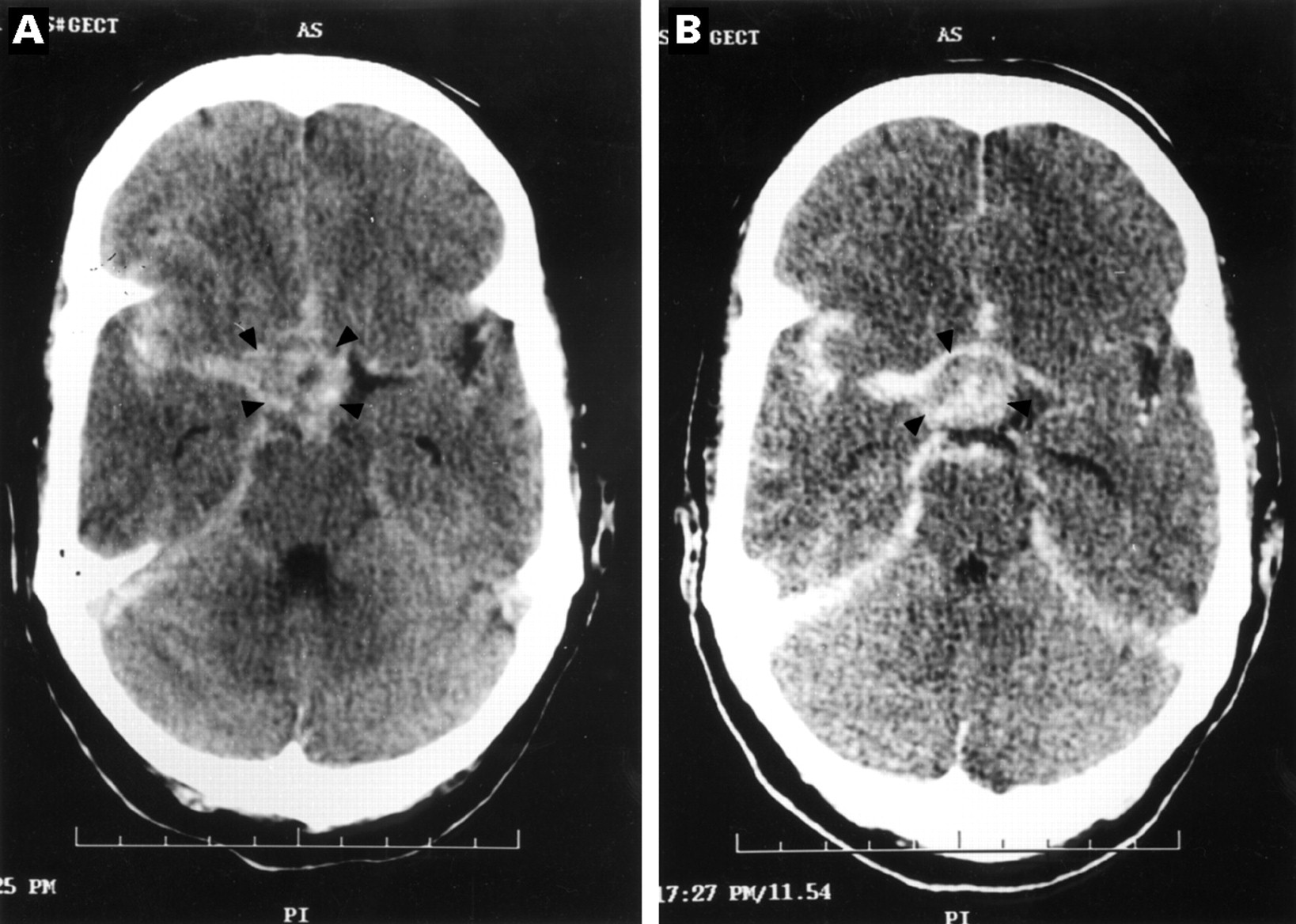
(A)Cranial CT without contrast, showing a heterogeneous but mostly high density mass in the suprasellar cistern (arrowheads). There is also extensive subarachnoid haemorrhage. (B) Cranial CT with contrast, showing central enhancement within a heterogenous high density mass (arrowheads).
Brain MRI confirmed haemorrhage within a pituitary tumour (fig 2 A). It could also be seen that the haemorrhage had ruptured through a defect in the tumour capsule into the subarachnoid space (fig 2 B). Despite the administration of 100 mg hydrocortisone intravenously every 6 hours and cardiopulmonary support her condition progressively worsened and she died 3 days after admission.

{kind=link}
{kind=link}
(A) Coronal T1 weighted MRI, showing suprasellar extension of a sellar mass. The area of high intensity signal (arrow) represents methaemoglobin within clotted blood. Note also the hyperintense tumour rim. (B) Contrast enhanced sagittal MRI T1 weighted image, showing that the bulk of the mass is isointense with brain. There is a defect posteriorly in the superior aspect of the capsule representing the site of rupture (arrow).
The clinical syndrome of pituitary apoplexy evolves within hours to days.2 The symptoms vary from mild to severe and can progress rapidly to coma and death. Because many patients are unaware that they harbour a pituitary tumour,pituitary apoplexy is often unrecognised at presentation. In pituitary apoplexy, blood and necrotic tumour tissue are enclosed and compressed within the confined space of the sella turcica, a region that is in close anatomical proximity to the basal cisterns. When the pressure gradient within the sella exceeds the resistance of the surrounding structures, blood is expelled into the subarachnoid space producing a clinical picture that may be indistinguishable from aneurysmal SAH.3 Thus pituitary apoplexy must be included in the differential diagnosis of “angiographically negative” SAH.4 Brain CT is the modality of choice in the initial investigation of SAH. It will show the spread and severity of the haemorrhage within the subarachnoid space, as well as any extension into the brain.1 When pituitary apoplexy is the cause, CT will usually show the pituitary tumour as well as any recent haemorrhage. Brain MRI is superior to CT in identifying the tumour as well as the associated haemorrhage or infarction. In the case presented here, the enhanced MRI also displayed the defect in the tumour capsule which represented the site of rupture. The management of pituitary apoplexy includes the immediate administration of high dose corticosteroids to combat adrenal insufficiency. When there is rapid deterioration of vision or a progressively worsening level of consciousness, urgent surgery in the form of trans-sphenoidal decompression should be carried out.