Abstract
Summary: Nasal leiomyoma, a benign tumor composed of smooth muscle cells, is rare in the head and neck region. Cellular leiomyomas of the uterus exhibit high intensity on T2-weighted images. Here we present a case of nasal leiomyoma in which the pathologic findings are similar to those of cellular leiomyoma. The present case exhibited slightly elevated intensity on T2-weighted images and marked enhancement on postcontrast images. CT findings showed a soft tissue lesion without bone erosion. These findings appear to be characteristic of intranasal leiomyoma.
Leiomyomas are benign smooth muscle tumors most commonly found in the uterus, skin, and gastrointestinal tracts (1, 2). Leiomyomas of the nasal cavity are very rare.
Previous studies have shown that leiomyomas of the uterus usually have low-intensity signals on T2-weighted images. Cellular leiomyomas of the uterus, however, have high-intensity signals on T2-weighted images (3). The pathologic findings of nasal leiomyomas are similar to those of cellular leiomyomas of the uterus (4, 5). In the present report, we describe a case of nasal leiomyoma with CT and MR imaging findings that differ from those of other nasal tumors. The present findings indicate that cellular leiomyoma and nasal leiomyoma have some characteristics in common.
Case Report
A 76-year-old woman complaining of nasal obstruction that had persisted for 1 year was admitted to our hospital. Her medical history included cataracts, diabetes mellitus, hypertension, and hyperlipidemia.
A CT scan showed a soft tissue lesion involving the right nasal cavity without apparent erosion of the bone and extending nasopharynx (Fig 1). MR imaging revealed a homogeneous mass, a low-intensity signal intensity on T1-weighted images, a slightly high-intensity signal intensity on T2-weighted images, and marked enhancement on postcontrast images (Fig 2).
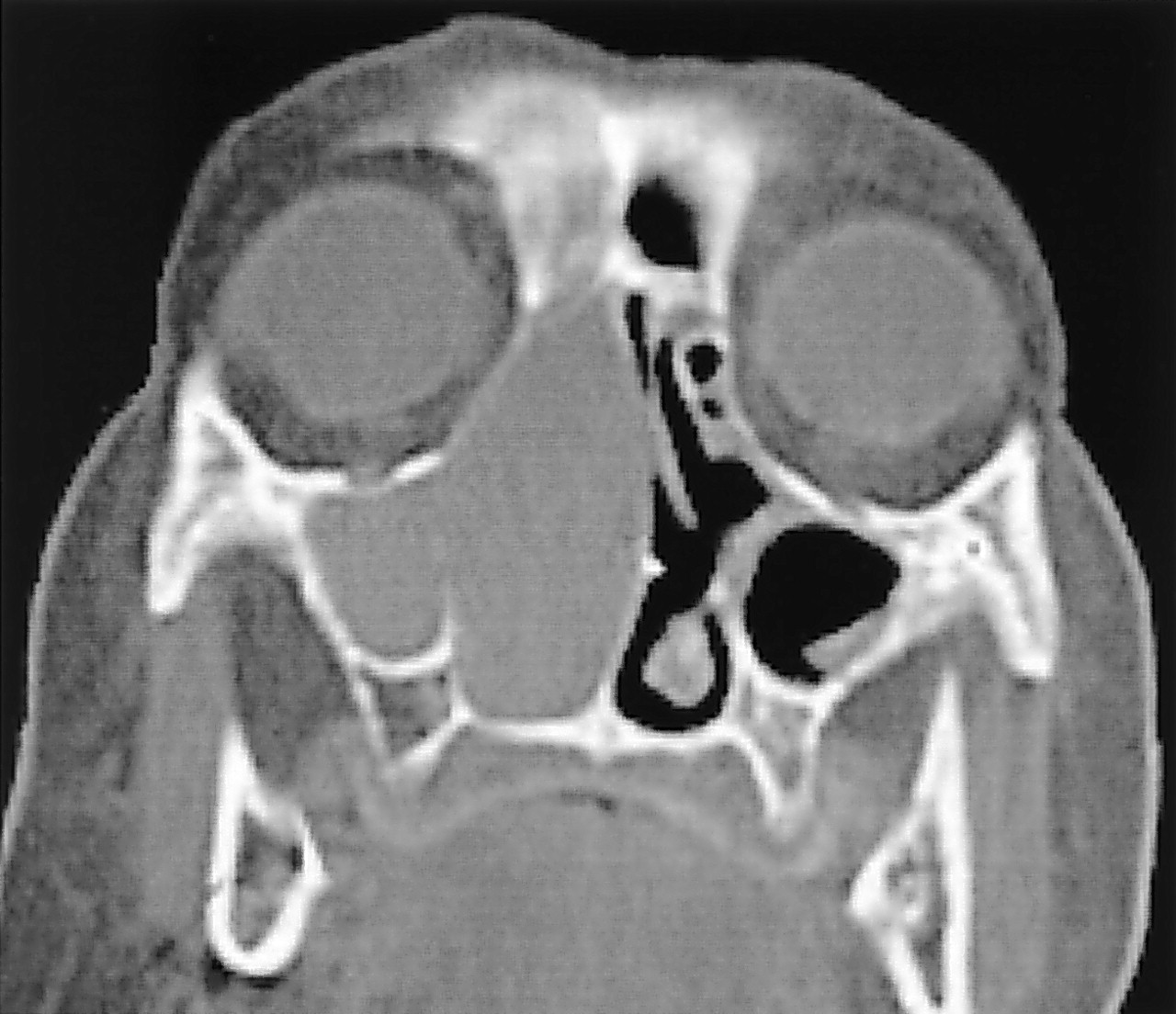
Noncontrast coronal CT scan shows a low-attenuated mass in the right nasal cavity without apparent erosion of the bone.
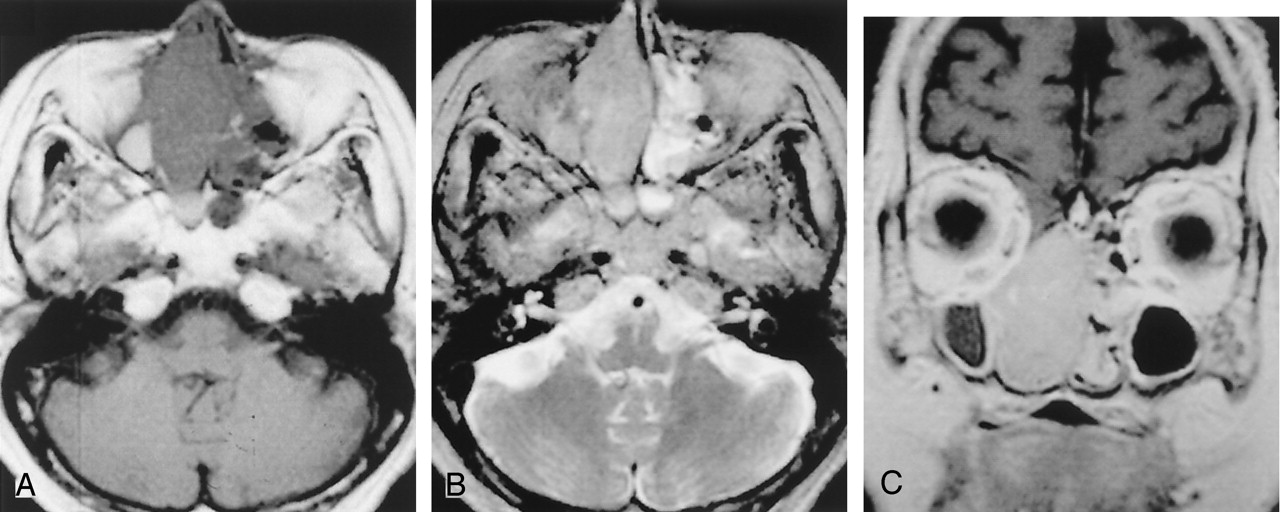
MR images show a homogeneous mass in the right nasal cavity adjacent to paranasal collection.
A, Axial T1-weighted image.
B, Axial T2-weighted image.
C, Coronal contrast-enhanced T1-weighted image.
A biopsy was performed, and the pathology report was consistent with hemangioma. Macroscopic examination at the time of surgery revealed a smooth mass arising from the nasal septum. The lesion was removed at our hospital, and the specimen was an 8 × 3 × 1.5 cm mass, with a white-grayish cut surface. The mass contained a hemorrhagic area. Necrosis and cystic formation, however, were not observed.
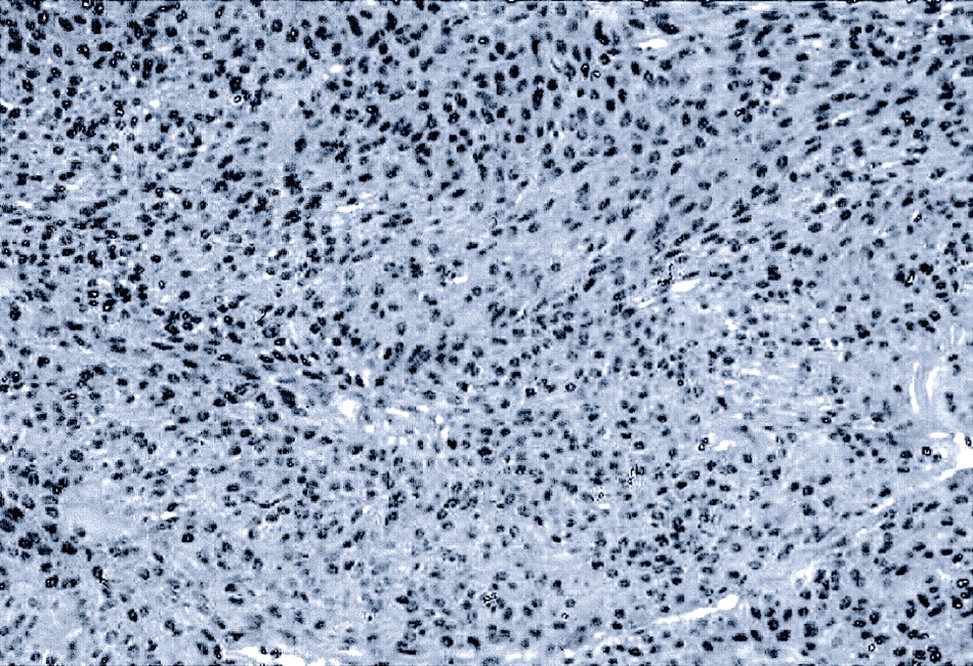
Histopathologic examination showed spindle-shaped cells organized in fascicles. A rich vascular compartment of a different caliber was observed, with apparent concentric arrangement of the spindle cells around the vessels (Fig 3). In immunohistochemical staining, the specimen was positive for vimentin and alpha-smooth muscle actin. A final diagnosis of leiomyoma was made. The patient is currently doing well postoperatively, without evidence of recurrent disease.
{kind=link}
{kind=link}
{kind=link}
Hematoxylin eosin–stained sections show spindle-shaped cells organized in fascicles or loosely arranged in a myxoid stroma.
Discussion
Leiomyomas most commonly (95% of cases) arise from the smooth muscle of the female genital tract (1, 2). Other common origins include the skin, subcutaneous tissue, and gastrointestinal tract. Less than 1% of all leiomyomas occur in the head and neck area, and only 3% of leiomyomas in the head and neck area occur in the nasal cavity (4).
Intranasal leiomyoma is extremely rare. Only 30 cases have been documented in the English-language literature (6). An additional 49 cases have been reported in the Japanese-language literature (7).
Intranasal leiomyomas are most commonly found in patients between the ages of 40 and 60 years. The female-to-male ratio among cases is 2:1. Most cases develop from the middle or inferior turbinate or nasal vestibule. Nicolai et al (8) reported that the nasal septum was the site of origin in 2/25 cases (8%) they examined.
MR imaging is particularly useful for differentiating neoplastic tissue from inflammatory changes such as sinusitis and mucocele. To the best of our knowledge, MR imaging has been used in four previously reported cases of intranasal leiomyoma (7–9). Two of the three cases in which T2-weighted images were used had slightly high intensity signal intensities on T2-weighted images (7–9). In all four cases, CT findings did not show bone erosion (7–9). These findings are similar to those of the present case.
Leimyomas are usually classified as vascular or nonvascular. Three hypotheses have been proposed for the origin of smooth muscle tumors in the nasal cavity: aberrant undifferentiated mesenchyma; smooth muscle elements in blood vessel walls; or both (1). Most findings are consistent with the hypothesis that these tumors originate in vascular smooth muscle (10, 11). Horie et al (12) reported that the cellularity of intranasal leimyoma was higher than that of leiomyomas at other sites. The pathologic findings in the present case are similar to those previously reported for cellular leiomyoma.
Yamashita et al (3) reported that cellular leiomyoma of the uterus consists of spindle-shaped cells. A rich vascular component is also present. Cellular leiomyomas, which are composed of compact smooth muscle cells with little or no collagen, can have relatively high-intensity signal intensity on T2-weighted images and exhibit enhancement on contrast-enhanced images (3). Uterine leiomyomas, however, usually have low-intensity signals on T2-weighted images.
The differential diagnosis for the present findings includes angiofibroma, hemangioma, neurinoma, inverted pappiloma, and malignant lymphoma (8, 9). Angiofibroma typically occurs in juveniles, whereas leiomyoma typically occurs in middle-aged patients. Angiofibroma and hemangioma have markedly high-intensity signals on T2-weighted images. Neurinoma exhibits heterogenous enhancement. Inverted pappiloma and malignant lymphoma are slightly enhanced in postcontrast images.
The present case exhibits a slightly high-intensity signal intensity on T2-weighted images and markedly homogenous enhancement on postcontrast images. Bone erosion was not observed on the CT images. These findings appear to be characteristic of intranasal leiomyoma.
References
- Received August 31, 2004.
- Accepted after revision September 12, 2004.
- Copyright © American Society of Neuroradiology