
Abstract
Summary: We herein describe two cases of moyamoya vasculopathy occurring in two men who used alkaloidal cocaine for years. One patient presented with aneurysmal subarachnoid hemorrhage and one with infarction in both lobes. Particularly impressive was a significant degree of collateral development with lenticulostriate networks.
Cocaine use has been associated with both acute hemorrhagic and ischemic stroke (1, 2). Although the precise pathophysiological course associated with cocaine-induced stroke is poorly understood, a number of mechanisms have been proposed. These include acute rise in blood pressure (3), cerebral vasoconstriction (4), vasculitis (5), and acute thrombosis (4). The limited number of studies that have examined histopathologic specimens of arteries in patients with cocaine-associated stroke have proven to be conflicting; some show nonspecific inflammatory cells or normal findings, and others show changes consistent with vasculitis (6). These studies have focused solely on the relation of cocaine to acute cerebrovascular complications. More rarely, ongoing cerebrovascular damage caused by cocaine dependency has been explored.
We herein describe an unusual presentation of moyamoya vasculopathy occurring in two men who used alkaloidal cocaine for many years. These cases provided evidence that chronic use may occlude major intracranial arteries. This radiologic finding should suggest to physicians cocaine abuse in appropriate circumstances.
Case Reports
A 34-year-old man (patient 1) with a 2-year history of hypertension presented to a North Dakota hospital for evaluation of new-onset change in personality and episodes of inappropriate behavior. He complained of a 1-month history of “complete lack of emotions.” The onset of these changes was insidious, without any preceding trauma, headache, change of vision, dysarthria, weakness, or paresthesias. The patient was transferred to our facility for further evaluation.
The patient showed his inappropriate behavior by urinating on the floor of the emergency department. His medical history was significant for hypertension treated medically for 2 years, toxic goiter treated with radioablation, and perforated diverticulum. Medications included atenolol and Synthroid. His social history was remarkable for having quit smoking 2 years earlier, consuming 6 beers per week, and a 10-year history of regular alkaloid cocaine use, with increased use within the previous month. Family history did not reveal stroke, early-onset atherosclerosis, or coagulopathy. A neurologic examination revealed an alert, oriented, cooperative man with a markedly flat affect, prominent perseveration, significant decrease in attention and recall, and a complete lack of abstraction. Comprehension and language were intact. Frontal release signs were absent. The remaining results of his neurologic and physical examinations were unremarkable. The results of the initial laboratory investigations, including a hematologic survey and measurement of electrolytes and sedimentation rate, were all normal. ECG showed normal sinus rhythm. Laboratory investigation for evidence of systemic vasculitis, coagulopathy, or infectious processes (including HIV and hepatitis) were negative. A transesophageal ECG revealed no thrombus, cardiomyopathy, or wall motion abnormality.
CT revealed patchy low attenuation with some mass effect in the left frontal lobe and a smaller low-attenuation zone in the right frontal lobe, both consistent with ischemic infarcts. Cerebral angiography showed prominent high-grade stenosis of both the internal carotid artery and middle cerebral arteries. Particularly impressive was the degree of collateral development, with significant lenticulostriate networks and collateral filling from the anterior circulation (Fig 1).
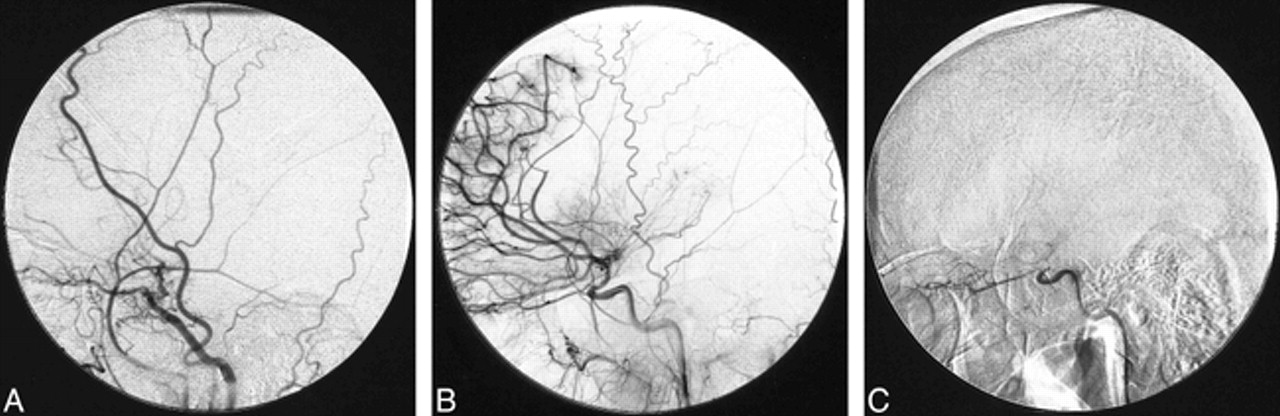
Patient 1. A, Lateral projection angiogram shows complete occlusion of the left middle cerebral artery with small residual left anterior cerebral artery filling.
B, Angiogram shows complete occlusion of the distal right middle cerebral artery with filling of medial and lateral lenticulostriate arteries. Note the extensive pial collateral circulation from the anterior cerebral arteries.
C, Lateral-view angiogram of the right carotid artery shows occlusion above the ophthalmic artery origin.
Similar angiographic findings were found in a 49-year-old man (patient 2) who was transferred for management of subarachnoid and intracerebral hemorrhages. He had been found unresponsive at his home and was brought to a local hospital, where his urine drug screen tested positive for cocaine. CT revealed subarachnoid hemorrhage and thalamic hematoma with intraventricular extension and hydrocephalus. Cerebral angiography showed a posterior cerebral artery aneurysm.
The patient was drowsy but able to answer simple questions. A neurologic examination showed absent upward gaze, downbeat nystagmus, and left hemiparesis. The patient recalled an acute onset of headache, with subsequent loss of consciousness, and freely admitted to having used alkaloid cocaine earlier that day. He admitted to a 30 pack-year history of smoking, 20-year cessation of alcohol, and 10-year history of daily alkaloid cocaine use. Family history included drug abuse in siblings and late-onset cardiovascular disease, but none had a stroke, vasculitis, or coagulopathy. CT revealed thalamic, subarachnoid, and intraventricular hemorrhages. Laboratory investigations were negative for systemic vasculitis and coagulopathy. HIV and hepatitis serologic analysis was negative. Transesophageal ECG was normal.
Cerebral angiography confirmed a posterior cerebral artery aneurysm but, in addition, showed bilateral, internal carotid artery occlusions with extensive collateral development in a moyamoya-like pattern (Fig 2). During subsequent clipping of the aneurysm, surgeons noted the significant “web” of collateral vessels that had to be dissected from the surface of the aneurysm. Histologic examination of a cortical biopsy specimen of the temporal lobe did not reveal vasculitis. With the exception of a right third nerve palsy acquired during surgery, the patient showed no focal neurologic deficits.

Patient 2. A, Angiogram shows high-grade stenosis of supraclinoid left internal carotid and anterior cerebral artery and complete occlusion of the left middle cerebral artery.
B, Angiogram shows extensive pial collateral circulation from posterior cerebral arteries and branches and prominent thalamostriate arteries.
Discussion
Cardiovascular complications caused by cocaine use, including myocardial infarction, arrhythmias, and cardiomyopathy, have dominated the literature. Within the last 2 decades, however, cerebrovascular complications have gained particular attention. Brust and Richter (7) reported the earliest descriptions of neurologic complications associated with cocaine use in 1977. Later case reports have appeared sporadically, showing the wide array of neurologic complications potentially associated with cocaine use (8). Intracerebral or subarachnoid hemorrhages have been reported most frequently, and have been tentatively attributed to the hypertension caused by intranasal cocaine use (9). After alkaloidal (or “crack”) cocaine made its appearance in 1983, the clinical spectrum changed with an emergence of ischemic cerebrovascular complications. Mechanistic theories point to cocaine and its sympathomimetic effects causing vasoconstriction with resultant cerebral ischemia. This hypothesis is supported by in vitro data showing that cocaine metabolites do potentiate vasoconstriction of cerebral arteries (10). Cerebral autoregulation may further indicate vasoconstriction in response to cocaine-associated acute surge in blood pressure. A recent provocative study with serial MR imaging and cocaine administration confirmed a dose-related vasoconstriction (11). Alternate mechanisms for cerebral ischemia have been proposed (12). There has been concern that cocaine metabolites increase platelet aggregation, specifically because of increased thromboxane and decreased prostacyclin (12). It has been postulated that cerebral vasospasm may cause endothelial injury, exposing damaged vessels to the enhanced platelet activity with subsequent acute thrombosis.
A much more controversial pathophysiological mechanism proposed for cocaine-associated stroke concerns whether a form of cerebral vasculitis exists. Although cocaine is pharmacologically similar to methamphetamines (a drug more commonly associated with vasculitis), there is a paucity of confirmatory data and considerable contradictory biopsy evidence. Brain biopsy in one of our patients also failed to show cerebral vasculitis.
Our patients share common distinctive angiographic features of severe cerebrovascular occlusive disease. These angiographic findings are conspicuously absent in studies specifically addressing ischemic stroke associated with cocaine abuse (1). The network of collateral vessels beyond bilateral carotid occlusions (the so-called acquired moyamoya vasculopathy) implies an insidious, progressive process rather than an acute event.
A number of potentially confounding factors might limit our ability to link cocaine to this vascular pattern definitively, but we think that the association is sound. For instance, nicotine typically does not result in this degree of cerebrovascular disease. In addition, one might question the reliability of both patients and the potential for abuse of other illicit substances that may cause an occlusive vasculopathy. However, both our patients freely admitted to regular long-term cocaine abuse.
Footnotes
↵1 Address reprint requests to Eelco F.M. Wijdicks, MD, Mayo Clinic, W8B, 200 First Street SW, Rochester, MN 55905.
References
- Received July 30, 1999.
- Accepted after revision January 12, 2000.
- Copyright © American Society of Neuroradiology








{kind=link}
{kind=link}