
Abstract
Summary: A 27-year-old man with congenital external carotid–jugular arteriovenous fistula presented with a diminished level of consciousness and an ataxic gait. Axial fluid-attenuated inversion-recovery (FLAIR) MR imaging revealed venous congestion, a dilated right jugular vein, and an area of high signal intensity in the brain stem and cerebellum. Angiography showed a dilated right external carotid artery and jugular vein and the presence of a fistula. After coil embolization of the fistula, axial MR FLAIR images showed only a few areas of high signal intensity in the brain stem and cerebellum. The causal factor was venous congestion in the inferior petrosal sinus and basilar plexus due to high blood pressure in the jugular vein. This case is presented for its unusual clinical and radiologic findings.
Arteriovenous malformations (AVMs) arising between the external carotid artery and the jugular vein are rare: a review of the literature revealed only nine cases that presented with symptoms other than a pulsatile mass (1–8). Only three of these patients, including two with vertigo, had neurologic findings attributable to the brain stem or cerebellum. We describe our findings in a patient with symptoms of congenital external carotid–jugular arteriovenous fistula.
Case Report
A 27-year-old man presented with various clinical symptoms, including ataxia, in April 1999. He had suffered from an attention deficit disorder since childhood, and his school records had been consistently poor. The patient had no history of trauma. A pulsatile swelling beneath his right ear caused it to move with each pulse, a finding that had been clearly visible since birth. He had experienced a gait disturbance for the 2 years prior to admission and often fell down. In addition, he had suffered from headache since April 1998 and pollakiuria since February 1999, at which time he had consulted a neurosurgeon, who diagnosed congenital external carotid–jugular arteriovenous fistula; however, the cause of the ataxia could not be explained.
Upon admission, the patient's blood pressure was 106/76 mm Hg and clinical findings included headache, nausea, and loss of appetite. No edema or cardiac failure was observed. Bruit was detectable above the pulsatile swelling beneath his right ear. His consciousness level was found to be impaired and he was absent-minded with poor recent memory. Bilateral choked disk, horizontal nystagmus, and truncal ataxia were present. Serum histochemical levels were all found to be within normal limits.
Axial fluid-attenuated inversion-recovery (FLAIR) MR imaging on the day of admission revealed venous congestion, a dilated right jugular vein, and an area of high signal intensity in the brain stem and cerebellum. A small infarction was detected in the temporal lobe (Fig 1A). Angiography showed a dilated right external carotid artery and internal jugular vein connected by a fistula (Fig 1B and C).

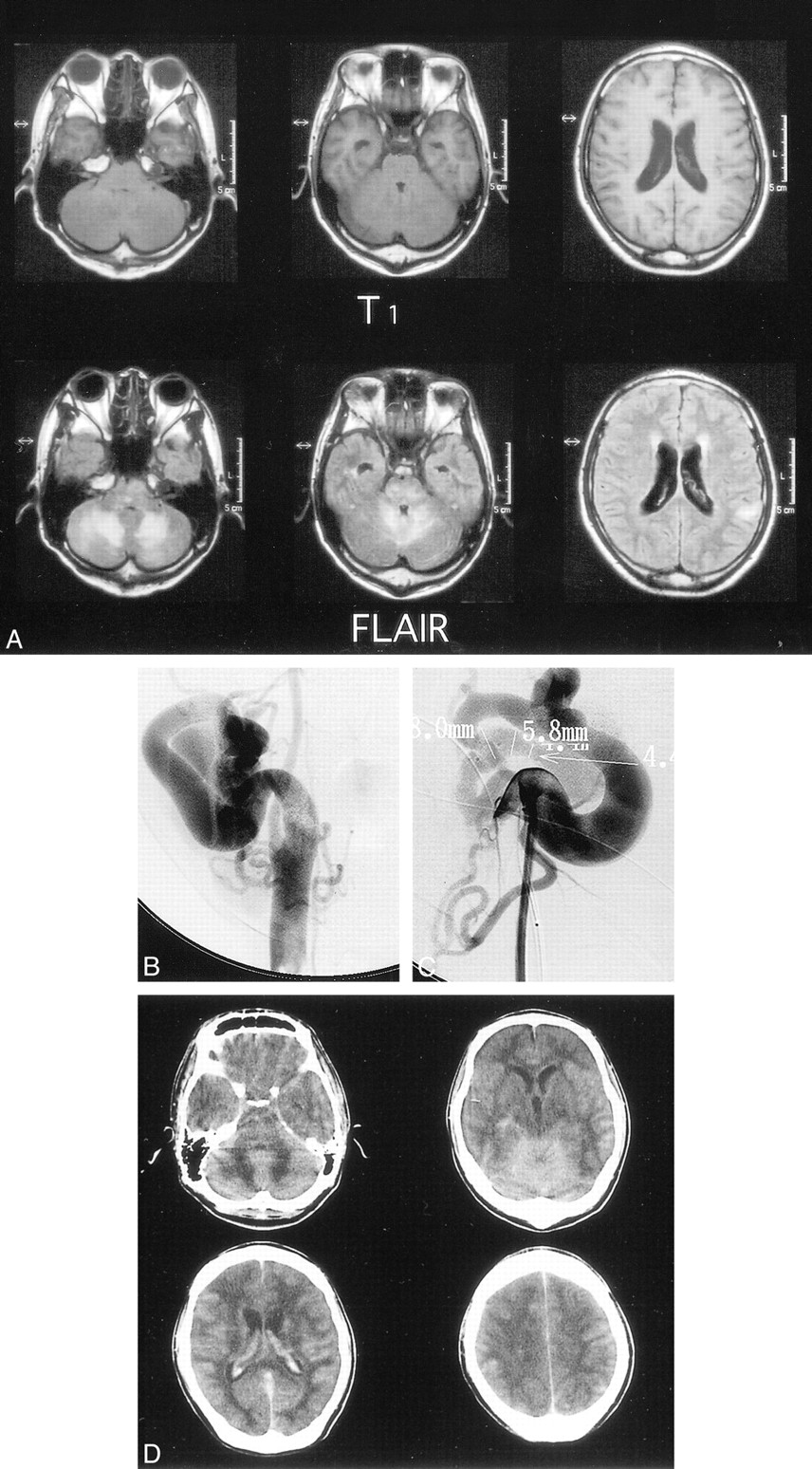
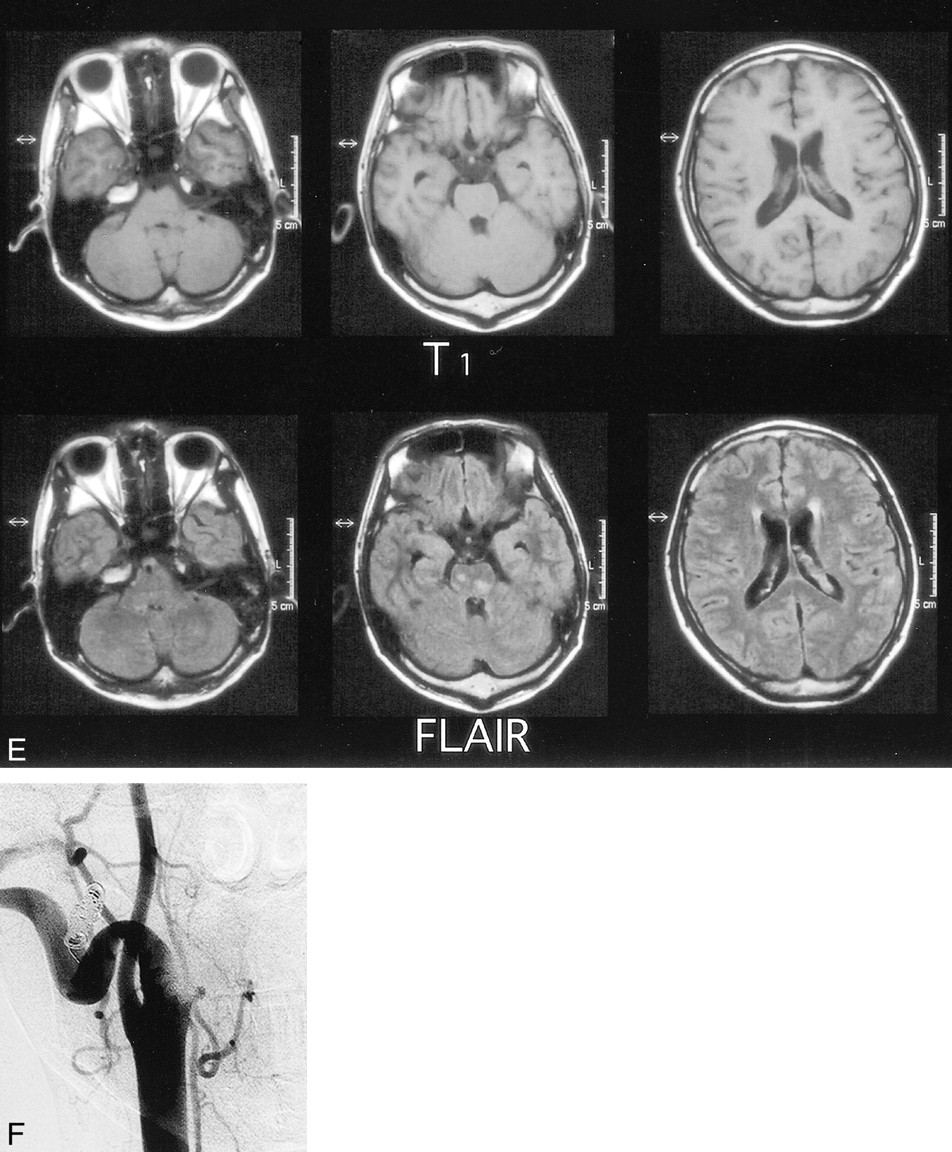
27-year-old man with congenital external carotid–jugular arteriovenous fistula who presented with a diminished level of consciousness and an ataxic gait.
A, Axial FLAIR MR images (6000/120) on the day of hospital admission show venous congestion, a dilated right jugular vein, and an area of high signal intensity in the brain stem and cerebellum. A small infarction is visible in the temporal lobe.
B and C, Angiograms, frontal (B) and lateral (C) views, 1 day after admission show a dilated right external carotid artery and internal jugular vein and the presence of a fistula.
D, Brain CT studies 5 hours after angiography show congestion and edema.
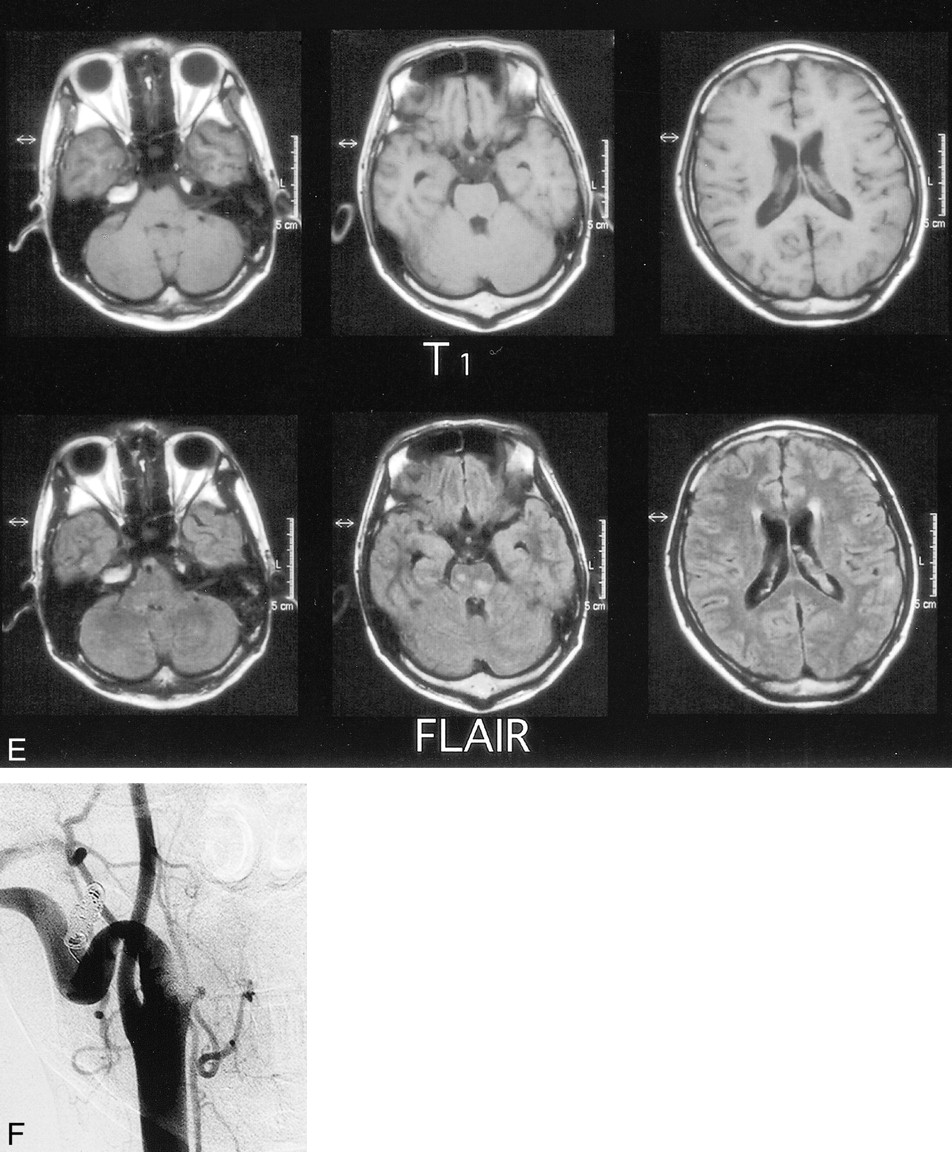
fig. 1 Continued.
E, Axial FLAIR MR images (6000/120) after embolization show only a few areas of high signal intensity in the brain stem and cerebellum.
F, Angiogram 1 month after admission shows that the external carotid artery and jugular vein are almost equivalent in size, and no arteriovenous communication is detected.
After the angiography, the patient's consciousness level worsened to a state of somnolence. A brain CT study 5 hours after angiography showed congestion and edema (Fig 1D). The patient was intubated and the fistula was embolized with coils 2 days after admission.
Following embolization, the pollakiuria and nausea disappeared, and the headache and ataxia diminished. Eighteen days postoperatively, axial MR FLAIR images revealed only a few areas of high signal intensity in the brain stem and cerebellum (Fig 1E). The patient had retrograde amnesia of the 2-month period prior to recovery.
Before embolization, angiography depicted venous congestion, and both the artery phase and delayed venous phase were observed. After embolization, however, no congestion was detected and only the artery phase was observed. The external carotid artery and internal jugular vein were almost equivalent in size, and no arteriovenous communication was observed (Fig 1F). The patient's right ear no longer moved with each pulse. Before surgical intervention, oxygen saturation values in the superior vena cava were 93.8%, PCO2 was 24.0 mm Hg, and PO2 was 87.9 mm Hg. After the procedure, the equivalent values were 86.2%, 31.7 mm Hg, and 47.6 mm Hg, respectively.
Discussion
The universality of the response of peripheral vessels to fistula formation warrants recognition of the hemodynamic principle that states that flowing blood, like flowing water, seeks the path of least resistance (9). The most common symptoms among patients with an arteriovenous fistula are a pulsatile mass, swelling, and bruit accompanied by a partial increase in blood flow (10, 11). In our case, low oxygen saturation in the superior vena cava and reversible venous congestion may have resulted from the steal phenomenon (12).
Axial MR FLAIR imaging in our patient showed that a preexisting small infarction with high signal intensity in the temporal lobe either decreased or disappeared after surgical embolization of the fistula. This finding indicated that venous congestion represented a reversible circulatory insufficiency. Willinsky et al (13) proposed the term venous congestive encephalopathy to describe neurologic deficits caused by venous hypertension. These authors reported two patients with ataxia caused by dural AVMs. In both cases, MR imaging revealed edema in the cerebellum while angiography showed dural AVMs at the torcular herophili near the inferior petrosal sinus with reflux into cerebellar veins. The cause of ataxia in the present case was venous congestion in the inferior petrosal sinus and basilar plexus due to high blood pressure in the jugular vein.
In some cases involving direct surgical correction of a fistula, segmental parotidectomy is performed; however, this is associated with a risk of injury to the facial nerve (14, 15). Endovascular treatment does not leave facial scars nor does it carry the risk of bleeding during surgical exposure (14). For these reasons, we elected to perform endovascular treatment in our case.
Footnotes
↵1 Address reprint requests to Masahiro Horiuchi, MD, Department of Internal Medicine, Division of Neurology, St. Marianna University School of Medicine, 2-16-1 Sugao, Miyamae-ku, Kawasaki, 216-8511, Japan.
References
- Received May 12, 2000.
- Copyright © American Society of Neuroradiology
In this issue








{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.