
Abstract
Summary: The persistent otic artery is a rare remnant of early fetal development that, to our knowledge, has been convincingly documented only once before with angiography. Other persistent vessels such as the trigeminal, hypoglossal, and proatlantal intersegmental arteries have been found to be associated with a variety of vascular anomalies. We believe we present the second case of a persistent otic artery documented by means of angiography and the first such case associated with multiple intracranial aneurysms.
The primitive otic artery is one of four transient carotid-basilar anastomoses and usually the first to disappear during embryogenesis. The early disappearance of the artery is theorized to account for its extreme rarity, as compared with the frequency of other persistent anastomoses (1). Our review of the literature revealed only one angiographic demonstration that would seem to confirm its rarity (2). To our knowledge, the following case represents the second example of a persistent otic artery.
Case Report
A 70-year-old female patient with a history of hypertension and an elevated cholesterol level presented with intermittent episodes of lightheadedness and blurry vision over the past year. Neurologically, she was intact with no clinical evidence of a visual deficit. A subsequent workup revealed a large 1.5-cm-diameter unruptured anterior communicating artery (ACoA) aneurysm that was depicted on MR images. Because of her age and comorbidities, the aneurysm was initially managed conservatively. Three months later, sonography of the abdomen revealed a 6-cm abdominal aortic aneurysm (AAA) requiring surgical intervention. Before the repair of the AAA, it was determined that the ACoA aneurysm should be treated to avoid the possibility of rupture during aortic cross-clamping.
An angiogram demonstrated a 2-cm ACoA aneurysm, which was substantially larger than it was 9 months earlier, as well as an incidental 5-mm left posterior communicating artery (PCoA) aneurysm (Fig 1). In addition, a carotid-basilar anastomosis was also seen during angiography. The anastomotic vessel arose from the carotid artery, within the petrous segment, and joined the basilar artery just at its midsection (Figs 1–3). This radiographic anatomy fulfilled the criteria for a persistent otic artery (3). The patient was also found to have a fetal PCA on the left (Fig 1). Proximal to its anastomosis with the otic artery, the basilar artery was smaller in caliber than it was distal to the anastomosis (Fig 2).

Left carotid artery angiograms demonstrate the persistent otic artery (a), the basilar artery (b), the fetal posterior cerebral artery (PCA) (c), the ACoA aneurysm (d), and the PCoA aneurysm (e).
A, Lateral image.
B, Oblique image.

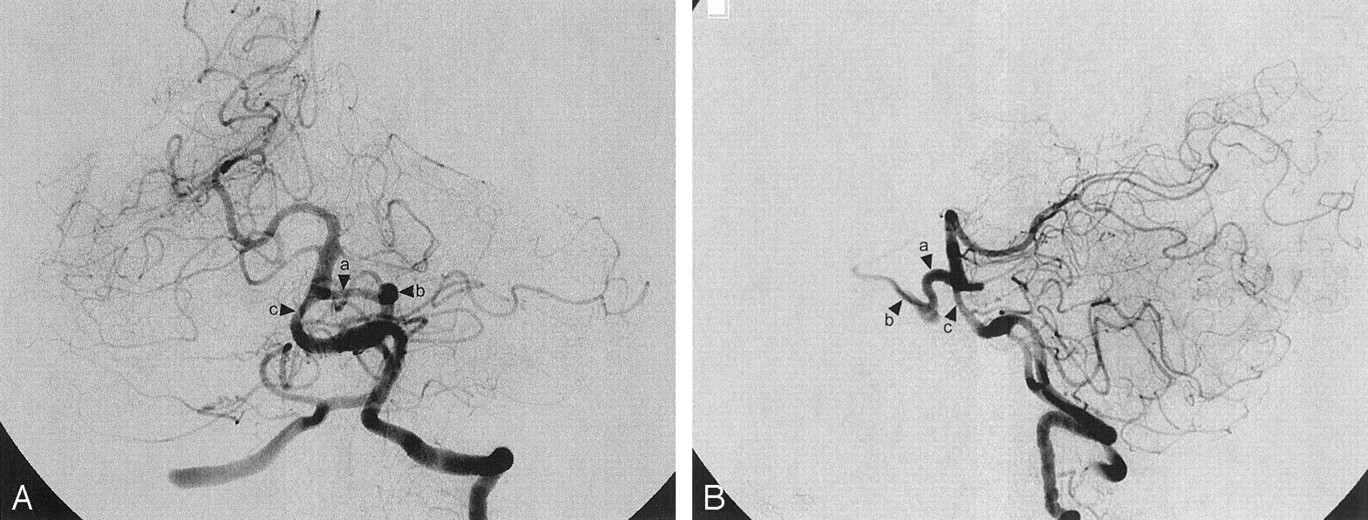
Left vertebral artery angiograms demonstrate the persistent otic artery (a) and the left internal carotid artery (b). In addition, note the smaller size of the basilar artery proximal to the otic artery (c).
A, Anteroposterior image.
B, Lateral image.
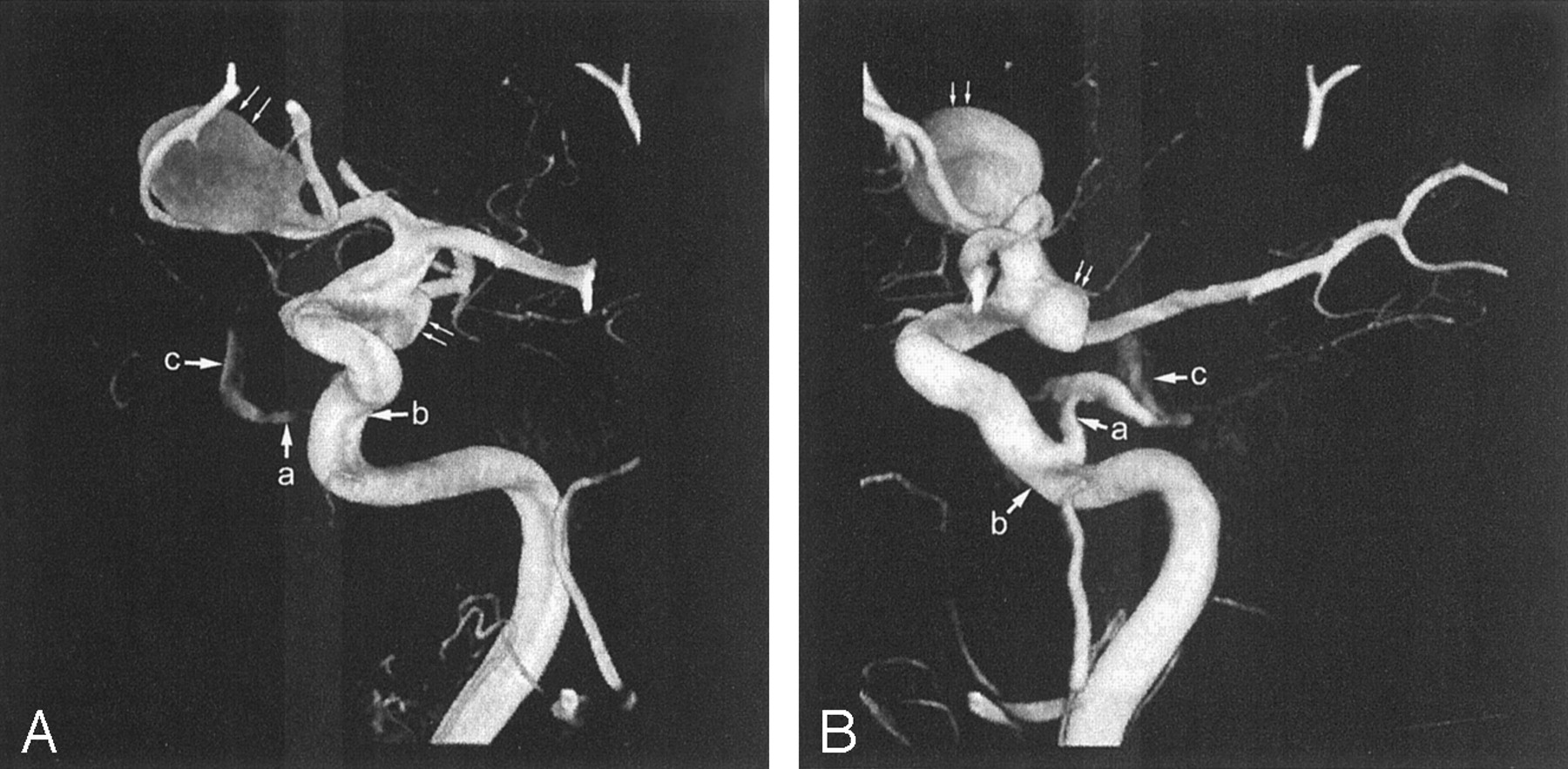
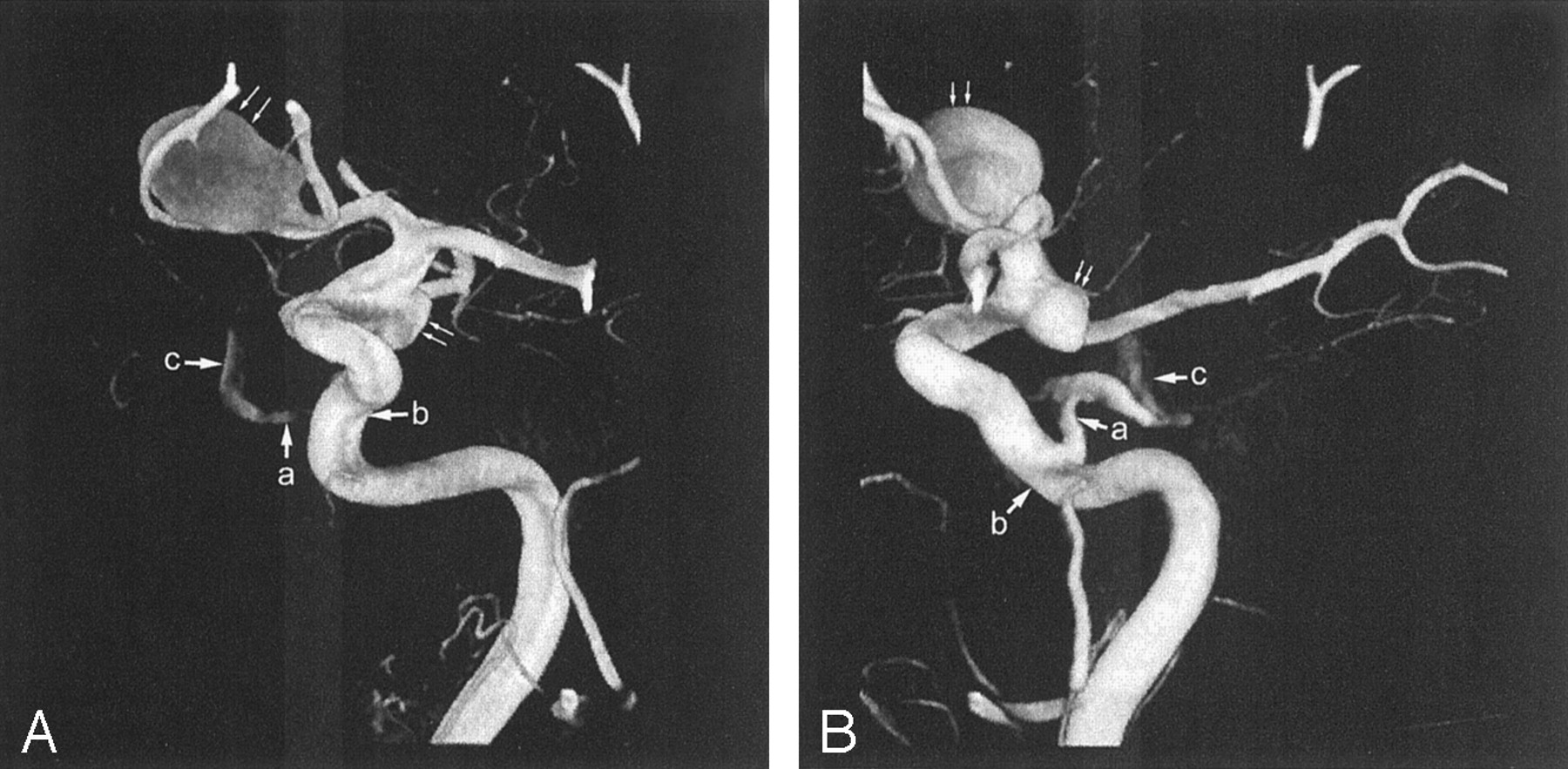
Three-dimensional rotational angiographic reconstructions of the left carotid artery demonstrate the persistent otic artery (a), the left petrous internal carotid artery (b), and the basilar artery (c). In addition, note the ACoA and PCoA aneurysms (arrows).
A, Anteroposterior image.
B, Lateral image.
The ACoA aneurysm was found to involve both A2 segments, which made clipping the preferred treatment. The patient underwent a left frontotemporal craniotomy with a left orbital osteotomy and clipping of both the large ACoA and left PCoA aneurysms.
Discussion
Primitive basilar-carotid anastomoses form early during fetal embryogenesis, at approximately 24 days (1). By 24–28 days into the development of craniocerebral circulation, the internal carotid arteries are supplied by the ventral aorta and the third aortic arches. Posteriorly, the hindbrain circulation begins to develop from two vascular beds that eventually fuse in the midline to become the basilar artery. This plexus is initially supplied from below by cervical intersegmental arteries and by four transient anastomoses between the posterior vascular plexus and the anterior carotid artery. From cephalic to caudal, these anastomoses are the trigeminal, otic, hypoglossal, and proatlantal intersegmental arteries, and, with the exception of the last, they parallel their respective cranial nerves. Ordinarily, the otic artery disappears at the 4th week of embryogenesis, followed soon after by the disappearance of hypoglossal and trigeminal arteries. The proatlantal intersegmental maintains the posterior circulation until the vertebral arteries are fully developed between 7 and 8 weeks (3). When these anastomoses fail to become obliterated, they become congenital persistent anastomoses. Their individual incidence rates have been found to be inversely related to their order of disappearance. The persistent trigeminal artery has a reported incidence of 0.1–0.2% (4), whereas the primitive otic has been convincingly documented only once before, with angiography, as mentioned above (2).
The primitive otic artery arises from the carotid artery within the carotid canal, it emerges from the internal acoustic meatus, and it joins the basilar artery at a caudal point (3). One of the earliest documentations is a sketch of an autopsy specimen in 1969. In this report, Kempe and Smith (5) demonstrate an artery emerging from the internal auditory meatus and joining the basilar artery and an associated ipsilateral hypoplastic vertebral artery. A few presumptive case reports describe a persistent otic artery, but two were based only on lateral skull images (6, 7) and a third failed to demonstrate the relationship of the vessel to the bony landmarks described previously (8). As mentioned earlier, the only convincing documentation of a persistent otic artery was in a 72-year-old woman with a right frontal cystic lesion, as described by Reynolds et al (2). This patient was also found to have a rudimentary right vertebral artery and no left vertebral artery.
Persistent anastomoses have also been associated with a variety of anomalies in the normal cerebral vasculature. Hypoplastic vasculature has been documented in association with all four persistent anastomosis (2, 9, 10, 11). The presence of arteriovenous malformations has also been associated with a persistent trigeminal artery and a hypoglossal artery (12, 13). These primitive anastomoses have also been associated with cerebral aneurysms. The persistent trigeminal and hypoglossal arteries have been associated with aneurysms of their respective branch points from the internal carotid artery (14, 15). The trigeminal, hypoglossal, and proatlantal intersegmental arteries have also been associated with aneurysms distant from the persistent vessel (10, 16, 17). Because of the rarity of a congenital otic artery, we believe no cases of an associated aneurysm have been documented until this case. Our patient had both a large ACoA and a left PCoA aneurysm. Additionally, the angiograms demonstrated a fetal PCA and a narrowed basilar artery proximal to the otic artery. These anatomic variations are important to recognize during angiography for endovascular and surgical planning.
Conclusion
To our knowledge, this report describes the second angiographically documented case of a persistent otic artery, as based on the criteria set forth by Lie (3). We also believe that this is the first documented case of a persistent otic artery associated with intracranial aneurysms.
References
- Received June 10, 2002.
- Accepted after revision July 15, 2002.
- Accepted after revision July 15, 2002.
- Copyright © American Society of Neuroradiology









{kind=link}
{kind=link}
{kind=link}