
Abstract
Summary: For broad-based intracranial aneurysms, both surgical and endovascular treatments are demanding. Flexible metallic stents provide an alternative treatment option for these patients, because they enable coil placement through the stent mesh. Evidence from extracranial arteries indicates that aneurysms may also spontaneously thrombose after stent placement. This case report documents three patients with saccular intracranial aneurysms in whom aneurysm thrombosis occurred after stent placement only, without additional packing of the aneurysms with coils.
The present case report documents aneurysm thrombosis induced by deployment of metallic stents in three cases of broad-based intracranial aneurysms. The risk of rebleeding and problems associated with the treatment of potential or symptomatic vasospasm while the aneurysmal lumen remains partially patent during the first weeks after stent deployment are discussed, together with the optimal postprocedural antithrombotic medication.
Case Report
For the last 3 years at our hospital, stent delivery has been a treatment option for patients with intracranial aneurysms. During that period, 399 (female-male ratio, 51.4%:48.6%) patients with 719 intracranial aneurysms underwent 617 different treatments for their aneurysms at our hospital. One hundred seventy (27.6%) of the treatments were performed by endovascular means. Twelve patients underwent intracranial stent placement after informed consent had been obtained. This case report concentrates on three of these patients in whom aneurysm thrombosis occurred after stent placement only, without additional packing of the aneurysms with coils.
Patient 1
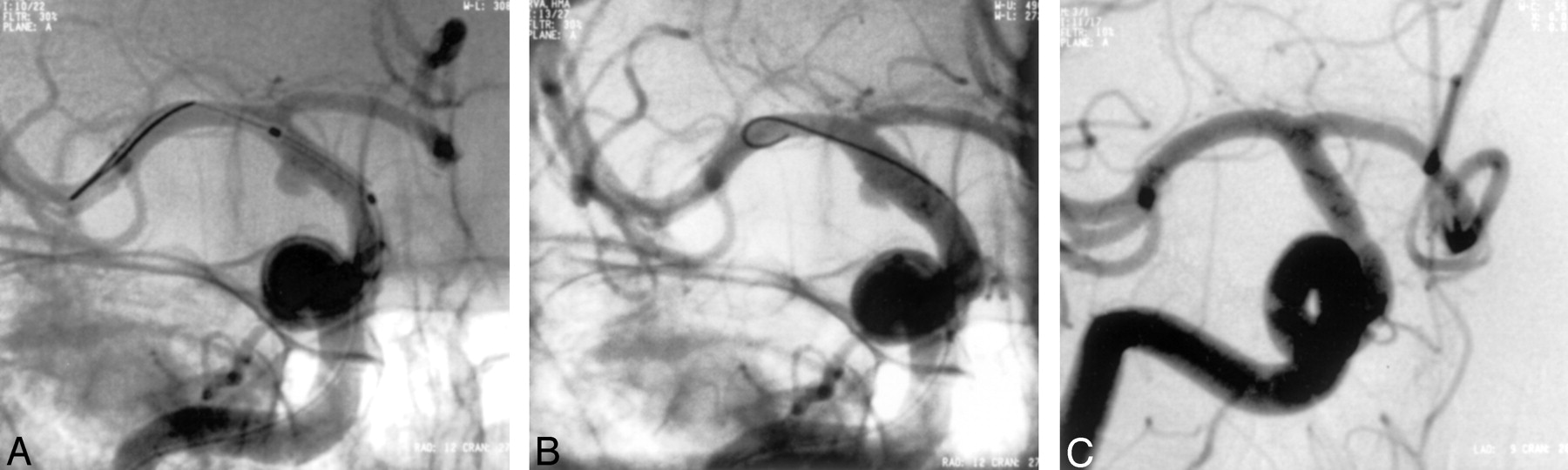
A previously healthy 57-year-old woman suddenly had severe headache and loss of consciousness. Subarachnoid hemorrhage and mild hydrocephalus were detected by use of CT examination. The patient also had pulmonary edema at admittance. Angiography revealed a wide-necked saccular aneurysm at the lateral wall of the basilar artery trunk (Fig 1A). Gradually, the patient’s clinical condition improved, except for visual disturbances caused by vitreous hemorrhage. After her informed consent had been obtained, a self-expanding coronary stent (5/24-mm Magic Wallstent; Schneider, GmbH, Bülach, Switzerland) was successfully delivered into the basilar artery 2 months after the bleeding. After deployment, the stent was fully open and completely covered the base of the aneurysm. In the immediate postprocedural control study, the aneurysmal sac was found to have diminished in size and intraaneurysmal flow had decreased. Antiplatelet medication (ticlopidine, 250 mg daily) was initiated and continued for 1 month, and acetylsalicylic acid and dipyridamole were administered thereafter. Follow-up angiography performed 1 month (Fig 1B), 6 months (Fig 1C), and 2 years later showed total obliteration of the aneurysm and full patency of the artery. The patient recovered uneventfully and returned to work. Two years after the occurrence of the subarachnoid hemorrhage, she had only mild visual impairment.

Patient 1.
A, Severe subarachnoid hemorrhage and mild hydrocephalus were detected by means of CT examination. The patient also had pulmonary edema at admittance. Four-vessel angiography revealed a saccular aneurysm in the lateral wall of the basilar artery trunk, located between the anterior inferior cerebellar arteries and superior cerebellar arteries. The left posterior cerebral artery filled from the carotid artery contrast medium injection (not shown).
B, Self-expanding 5/24-mm coronary Wallstent (straight arrow) was deployed in the basilar artery over a Choice-PT extra-support guidewire (curved arrow). After deployment, the stent was fully patent and completely covered the base of the aneurysm.
C, Aneurysm was totally thrombosed and stent remained patent on control angiogram obtained 6 months later.
Patient 2
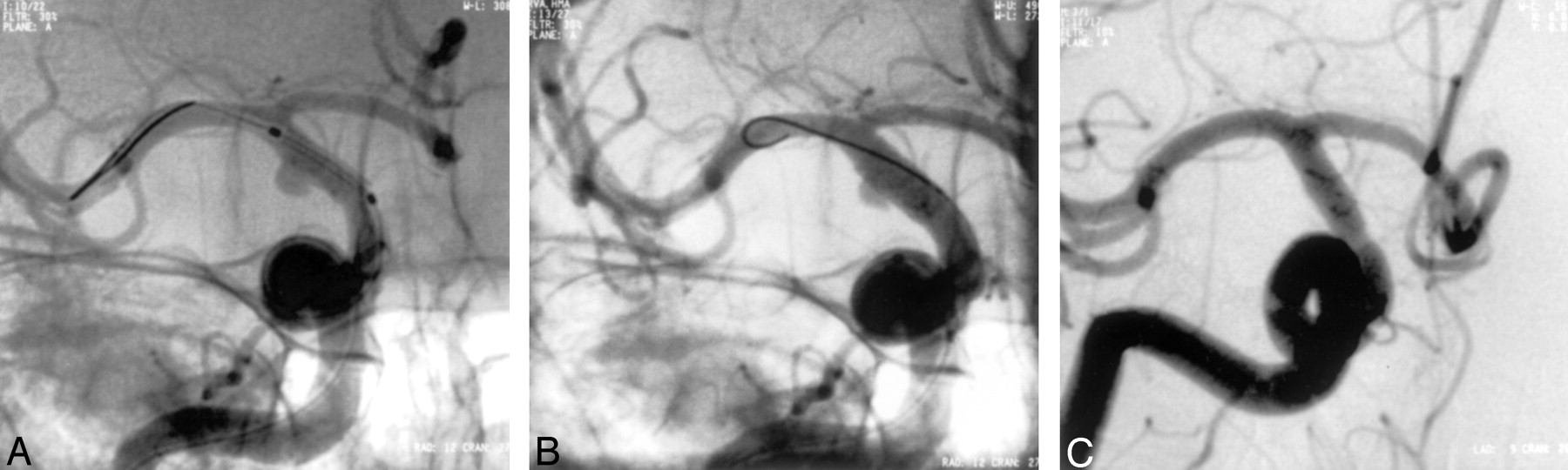
A previously healthy 44-year-old man had severe headache and nausea while driving a car. Subsequent CT revealed subarachnoid hemorrhage, and angiography showed a small broad-based blisterlike aneurysm on the lateral wall of the distal internal carotid artery (ICA) on the right (Fig 2A). Surgical treatment of the aneurysm was considered risky. A balloon-expanded stent (4/9-mm S7; Medtronic AVE, Santa Rosa, CA) was delivered, covering the orifice of the aneurysm. Control angiography performed immediately after the intervention (Fig 2B) showed full patency of the ICA and persistent but slower flow into the aneurysmal lumen. The stent also covered the orifice of the anterior choroidal artery, located close to the level of the aneurysm, but the filling of this artery remained normal. Acetylsalicylic acid (100 mg) and clopidogrel (75 mg daily for 1 month, with a loading dose of 300 mg) were initiated. Control angiography performed 1 week after the procedure revealed total thrombosis of the aneurysmal lumen. The patient was discharged from the hospital in good clinical condition. Control angiography performed 3 months later showed that the aneurysm remained fully thrombosed (Fig 2C).
Patient 2.
A, Angiogram shows a small broad-based blisterlike aneurysm on the lateral wall of the distal ICA on the right. A balloon-expanded stent has been advanced to the level of the aneurysm orifice but has not been dilated. The tip of the guidewire is in the middle cerebral artery.
B, Angiogram obtained immediately after stent placement shows persistent but slower flow into the aneurysmal lumen.
C, Control angiogram obtained 3 months after intervention shows that the ICA is fully patent and the aneurysm totally thrombosed.
Patient 3
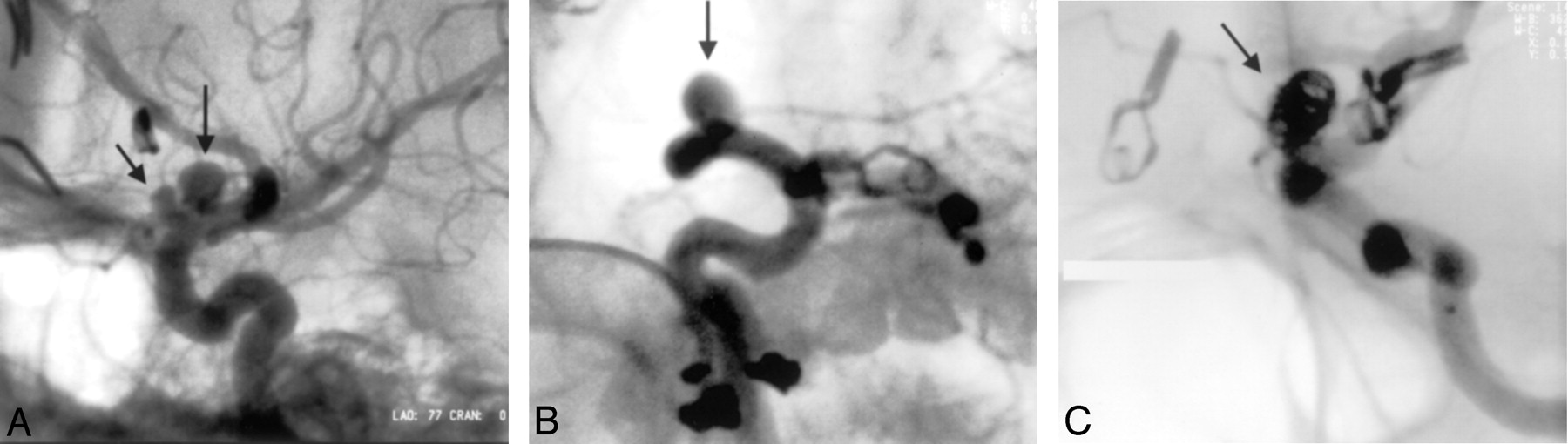
A previously healthy woman had a subarachnoid hemorrhage at the age of 39 years. Four-vessel angiography revealed multiple aneurysms: bilateral middle cerebral artery aneurysms, pericallosal artery and anterior communicating artery aneurysms on the right, and two broad-based aneurysms in the anterior wall of the left ICA located in the segment between the ophthalmic and posterior communicating arteries (Fig 3A). On the basis of the location of the hematoma as revealed by CT, the pericallosal artery aneurysm was considered ruptured and was clipped. Five months after the occurrence of the subarachnoid hemorrhage, the unruptured anterior communicating artery and middle cerebral artery aneurysms on the right were operated on uneventfully. During the third craniotomy, which was performed 10 months after the occurrence of the subarachnoid hemorrhage, the small unruptured middle cerebral artery aneurysm on the left was clipped and clipping of the two ICA aneurysms was attempted with the help of perioperative angiography and proximal temporary balloon occlusion of the parent artery. However, clipping was considered too hazardous and the two aneurysms were left in place. Because the neck of both of these aneurysms was wide and thus unfavorable for coiling, a balloon-expanded metallic stent (Inx, Medtronic) was first delivered to cover the neck of both of the aneurysms. After deployment of the stent, a dissection of the distal ICA and proximal middle cerebral artery was noticed. However, the angiographic flow limiting stenosis caused by the dissection disappeared within a few minutes. After the procedure, the patient recovered uneventfully. The administration of clopidogrel and acetylsalicylic acid was continued, and filling of the aneurysm lumen with electrolytically detachable coils was scheduled for 3 months after stent delivery. Control angiography performed 3 months after stent delivery showed the more proximal aneurysm to be totally occluded (Fig 3B). The partly thrombosed more distal aneurysm was selectively catheterized with a microcatheter and filled with GDCs (Fig 3C). After 6 months, the patient remained free of symptoms and had returned to work as a school teacher.

Patient 3.
A, Angiogram shows two broad-based aneurysms in the anterior wall of the left ICA, located in the segment between the ophthalmic and posterior communicating arteries (arrows).
B, Control angiogram obtained 3 months after the delivery of a metallic stent covering the orifice of both aneurysms. The more proximal aneurysm is totally occluded. The more distal aneurysm remains patent (arrow).
C, Aneurysm remaining patent has been catheterized selectively and filled with GDCs (arrow).
Discussion
In patients with subarachnoid hemorrhage, early craniotomy and surgical clipping have been advocated to isolate the ruptured aneurysm from the intracranial circulation, thus preventing rebleeding and enabling aggressive treatment of potential symptomatic vasospasm. Endovascular coil embolization is a technique that offers an alternative treatment option for these patients. Recently, the indications for endovascular treatment have widened. Embolization with mechanical or electrolytically detachable coils may be attempted as the primary treatment option (1–5). However, in broad-based intracranial aneurysms, both surgical treatment and endovascular coil embolization are demanding, and alternative treatment options for these patients are desirable (6, 7).
The development of flexible metallic stents provides an important new alternative for the endovascular treatment of lesions in cervicocranial arteries (8). Balloon-expandable or self-expanding metallic stents facilitate successful GDC packing through the stent mesh and therefore constitute a promising option for the treatment of broad-based, fusiform, or dissecting aneurysms located both in the cervical and proximal intracranial arteries (6, 7, 9). Another possibility for the treatment of large broad-based aneurysms may be a combination of a stent and balloon-assisted occlusion of the aneurysm with a liquid polymer.
There is evidence from animal studies and from extracranial human arteries that aneurysms may also spontaneously thrombose after stent placement (10, 11), without additional packing of the lumen. However, this has not been previously reported in association with saccular intracranial aneurysms in humans.
Packing of the aneurysm with GDCs after stent placement was not attempted in the same session in two of our patients with ruptured aneurysms (patients 1 and 2). This was partly because the filling of these aneurysms with contrast agent was obviously reduced, as shown by the immediate postprocedural angiography, indicating potential progressive thrombosis of the lumen after the periprocedural heparinization is ceased. In addition, in patient 2, the depth of the aneurysmal lumen was measured to be <2 mm (Fig 2B) and thus less than the diameter of the smallest coil available. In very small aneurysms, the risk of perforation is especially high.
In addition, even if it may be feasible to coil the aneurysm through the stent mesh during the same session, the manipulation of the stent with a guidewire and a microcatheter immediately after deployment may lead the stent to slide to an unintended position, as was our experience in one of the earlier cases. It may be speculated that the immediate attachment of a stent to the vessel wall is poorer in young patients with aneurysmal lesions than it is in vasoocclusive atherosclerotic lesions with a thicker intima-media complex. In our third case, the two aneurysms in the ICA were unruptured and it was considered safer to wait for the full endothelialization of the stent to the vessel wall before the complementary coiling.
In patient 2, the size of the aneurysm was very small and the width of the neck was obviously very unfavorable for coiling, even with the remodeling technique and a 3D coil. In patients 1 and 3, the remodeling technique with balloon protection was considered to be an alternative treatment method. However, we chose to attempt to use a stent plus coiling in a second session because it is our experience that complete packing of a wide aneurysm neck with coils is sometimes not possible with the remodeling protection technique. The nature of these aneurysmal remnants is unpredictable (5).
Delayed aneurysm thrombosis after stent placement, similar to that in our experience, has been reported in association with dissecting cervical pseudoaneurysms and in peripheral arteries (10, 11). Benndorf et al (12) used two overlapping stents and suggested that the reduced stent porosity caused by the overlapping stents, which result in significant hemodynamic changes inside the aneurysmal sac, may accelerate intraaneurysmal thrombosis and may be helpful in achieving a more rapid complete occlusion than that achieved by single stent placement.
Surgical treatment of large aneurysms in the basilar area and in the proximal intracranial segment of the ICA can be difficult and hazardous without proximal control of the parent vessel. Complications with the parent artery easily lead to serious ischemic consequences. In the basilar area and in the proximal ICA segments, the usual technical difficulty lies in properly visualizing the neck of the aneurysm. The methods used for this are either trimming of the skull base or decompressing the aneurysm sack by endovascular methods before clipping the aneurysm. Metallic stents together with coils seem to be one promising option in treating these difficult aneurysms.
Delivery of stents to the small caliber, tortuous intracranial arteries requires low-profile, flexible stents with good tractability and “pushability” properties for the delivery catheter. The use of a heavy-duty guidewire and distally advanced guiding catheter with firm back-up are mandatory, as is the ability to relieve arterial spasm with, for example, intraarterial boluses of nimodipine. Stent designs are continually being improved to overcome problems in delivery and deployment and to achieve prevention of stent thrombosis. A stent for treatment of intracranial aneurysms should preferably be self-expanding with good tractability and flexibility, because the radial force required is less than that required in the treatment of vasoocclusive lesions. We used a self-expanding coronary stent in one of our patients; in our experience, however, the advancement of balloon-expanded coronary stents or dedicated intracranial stents to the intracranial target lesions is currently easier than the advancement of self-expanding stents.
Anticoagulation and antithrombotic medications are generally considered contraindicated immediately after acute subarachnoid hemorrhage, before the aneurysm is secured. On the other hand, antithrombotic medication is generally considered necessary after the deployment of intraarterial metallic stents to prevent stent thrombosis and distal thromboembolic complications. Experience in the use of stents in the coronary and peripheral arteries favors the use of antiaggregatory medication for at least 1 month after the intervention to maintain patency of the parent artery. Treatment with acetylsalicylic acid and ticlopidine is associated with a lower rate of coronary stent thrombosis than is treatment with acetylsalicylic acid alone or a combination of acetylsalicylic acid and warfarin, although there are more hemorrhagic complications than with acetylsalicylic acid alone. There is evidence from randomized clinical trials and coronary registries that clopidogrel, in addition to its better tolerability and fewer side effects, is at least as efficacious as ticlopidine. In our three patients with unsecured aneurysms and antiaggregatory treatment, no rebleedings occurred. In all cases, aneurysm thrombosis occurred gradually after stent deployment, despite the ongoing antiaggregatory medication, while the parent artery remained patent. The stent mesh over the orifice of the aneurysm probably causes alterations in the flow velocity and pattern inside the aneurysmal lumen and may thus induce gradual, slow development of thrombosis. Our three patients did not develop clinical signs of vasospasm, and there was no need for the use of triple H (hypervolemic, hypertensive, and hyperdynamic) therapy. Hypervolemia and hypertension can be considered contraindicated in cases with unsecured aneurysms.
Conclusion
Our findings with these three patients imply that coil packing may not always be necessary during the same session with stent placement in small intracranial lateral-wall aneurysms, because the stent alone may induce spontaneous aneurysmal thrombosis during the ensuing weeks. The magnitude of the added risk imposed by the need to use antiplatelet medication may be significant and remains to be determined.
References
- Received June 3, 2002.
- Accepted after revision July 18, 2002.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Efficient multi-fidelity computation of blood coagulation under flow
- Effect of stenting on progressive occlusion of small unruptured saccular intracranial aneurysms with residual sac immediately after coil embolization: a propensity score analysis
- Multiple overlapping stents as monotherapy in the treatment of 'blister' pseudoaneurysms arising from the supraclinoid internal carotid artery: a single institution series and review of the literature
- Report of two cases of a rare cause of subarachnoid hemorrhage including unusual presentation and an emerging and effective treatment option
- Technical, angiographic and clinical outcomes of Neuroform 1, 2, 2 Treo and 3 devices in stent-assisted coiling of intracranial aneurysms
- A single center comparison of coiling versus stent assisted coiling in 90 consecutive paraophthalmic region aneurysms
- A Novel "Y" Stent Flow Diversion Technique for the Endovascular Treatment of Bifurcation Aneurysms without Endosaccular Coiling
- X-Configured Stent-Assisted Coiling in the Endovascular Treatment of Complex Anterior Communicating Artery Aneurysms: A Novel Reconstructive Technique
- Endovascular treatment of recurrent intracranial aneurysms with re-coiling or covered stents
- Clinical and Angiographic Follow-Up of Stent-Only Therapy for Acute Intracranial Vertebrobasilar Dissecting Aneurysms
- Cerebral Aneurysm Multicenter European Onyx (CAMEO) Trial: Results of a Prospective Observational Study in 20 European Centers