
Abstract
Summary: When squamous cell carcinoma (SCC) involves the palatine tonsils, they are generally enlarged and demonstrate intermediate to high signal intensity on T2-weighted MR images and enhance after gadolinium administration. We have identified two patients with SCC of the tonsil where the affected tonsil has low signal intensity on T2-weighted MR images and is smaller than the contralateral normal tonsil. We present the “small, dark tonsil” as an alternative imaging presentation of SCC and a new sign to look for when evaluating the patient with metastatic lymphadenopathy from an unknown primary tumor.
Squamous cell carcinoma (SCC) of the palatine tonsil is frequently clinically evident, with a visible oropharyngeal mass, often associated with unilateral or bilateral pathologic cervical lymph nodes. In such circumstances, imaging is important to define the extent of and accurately stage the primary tumor and nodal disease (1, 2). In some cases, however, the presentation of SCC of the palatine tonsil may be very subtle. Carcinoma of the tonsil may account for as many as 20–30% of primary sites of disease in patients who present with lymph node metastases from an unknown primary site (3–5). These patients typically have unremarkable physical examinations of the oral cavity and oropharynx. Imaging studies, along with endoscopic examination with directed biopsies and unilateral or bilateral tonsillectomy, are generally performed to look for a primary site of disease, because the identification of a primary site has a significant impact on disease management. The imaging assessment of these patients is usually focused on detecting diffuse or focal enlargement of the tonsil or areas of abnormally high signal intensity on the T2-weighted and postgadolinium images (6).
We report the cases of two patients who presented with SCC metastatic to level II cervical lymph nodes with no evidence of primary tumor on office or endoscopic physical examination. MR imaging in both showed diminished size and decreased T2 signal intensity of the tonsil ipsilateral to the malignant lymphadenopathy. Both patients underwent subsequent tonsillectomy, which confirmed the primary site of disease to be the small, dark tonsil.
Case Reports
Case 1
A 37-year-old woman who was 22 weeks pregnant presented with a firm, painless mass on the left side of her neck. She had first noted it approximately 4 months before presentation. Fine needle aspiration of the mass yielded moderately differentiated keratinizing SCC on a background of benign lymphoid tissue. Her clinical examination was normal. MR imaging of the neck showed the known level II malignant lymph node but no mass or abnormal T2 prolongation to suggest a primary site of malignancy. The left palatine tonsil was asymmetrically small and dark when compared with the right (Fig 1), but no significance was attached to this finding at the time of the study. No gadolinium was given, because the patient was pregnant. Whole-body FDG-PET was negative for disease other than the known neck abnormality. Direct laryngoscopy, bronchoscopy, and esophagoscopy showed no primary malignancy.

Case 1, a 37-year-old female patient with a left neck mass.
A, Axial fast spin-echo T2-weighted MR image with fat saturation (4000/102/2 [TR/TE/NEX]) demonstrates an enlarged, hyperintense level II lymph node on the left (N). Fine needle aspiration of the node showed moderately differentiated SCC.
B, Coronal fat-saturated fast spin-echo T2-weighted MR image (4000/102/2) of the palatine tonsils does not demonstrate an obvious primary lesion. In fact, the left tonsil (arrows) has slightly decreased signal intensity and is smaller than the right tonsil (arrowheads).
C, Coronal noncontrast T1-weighted MR image (600/14/2) of the palatine tonsils again shows the relative small size of the left tonsil when compared with the right. Tonsillectomy yielded moderately differentiated invasive SCC in the small and relatively T2-dark left tonsil.
The patient underwent bilateral tonsillectomy. Gross examination revealed homogeneous, soft tissue with no focal lesions or masses, but histologic examination of the left tonsil revealed moderately differentiated invasive keratinizing SCC. Little to no fibrosis was seen. Because of the pregnancy, treatment recommendations were different from our standard protocol. A neck dissection was done initially, with radiation therapy and chemotherapy given after the birth of her child at 36-week gestation. The patient is disease-free at 24 months after treatment.
Case 2
A 59-year-old man with a history of tobacco and alcohol use presented with a 1.5-cm painless right neck mass at the angle of the mandible. Fine needle aspiration was nondiagnostic. Eight months later, the mass measured 6.5 cm and became tender, and the patient was referred to our institution for treatment. Fine needle aspiration revealed poorly differentiated, nonkeratinizing SCC.
MR imaging showed a complex right upper neck mass involving levels II and III, consistent with a partially necrotic conglomerate nodal mass with extracapsular spread. The right tonsil was smaller than the left tonsil and had lower T2 signal intensity (Fig 2). MR imaging did not clearly show a primary site of disease, although at the time it was questioned whether the larger and more hyperintense left tonsil was actually a contralateral primary site of disease. Whole-body FDG-PET demonstrated uptake in the right nodal conglomerate but no clear primary site of disease. Only mild uptake was seen in the left and right tonsils, with standardized uptake values (SUV) of 2.1 and 1.7, respectively (<3 SUV is considered normal).
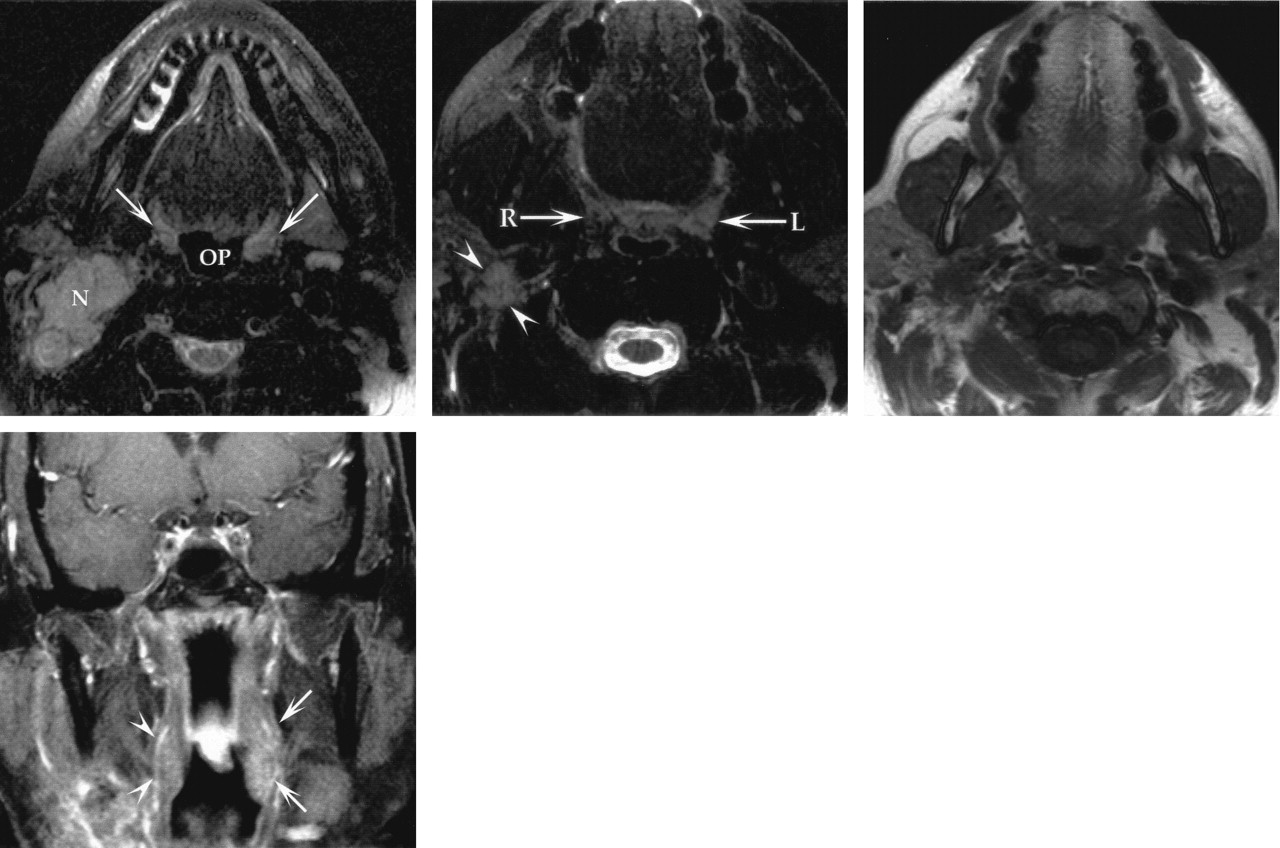
Case 2, a 59-year-old male patient with enlarging mass at the angle of the right mandible.
A, Axial fast spin-echo T2-weighted MR image with fat saturation (4000/102/2) at the level of the oropharynx (OP). There is a conglomerate level II nodal mass on the right (N). The right palatine tonsil is asymmetrically small and slightly hypointense when compared with the left (arrows). No discrete tonsillar mass is identified.
B, A more superior axial fast spin-echo T2-weighted MR image with fat saturation (4000/102/2) shows the upper aspect of the level II nodal mass (arrowheads) and the relatively small and dark appearance of the right palatine tonsil when compared with the left (arrows).
C, Axial T1-weighted image (600/14/1.5) shows that the right palatine tonsil is smaller than the left but has similar T1 signal intensity characteristics.
D, Coronal postgadolinium T1-weighted image with fat saturation (600/14/1.5) demonstrates the slightly reduced enhancement of the smaller right tonsil (arrowheads) compared with the left (arrows). Right tonsillectomy yielded SCC, whereas the left palatine tonsil was normal.
Direct laryngoscopy, bronchoscopy, and esophagoscopy showed no evidence for a primary site of disease. The patient underwent bilateral tonsillectomy, which showed a 0.9-cm moderately differentiated invasive SCC in the right tonsil, along with moderate fibrosis. The left tonsil and biopsy findings of the tongue base were normal. The patient was treated with radiation therapy and chemotherapy with a complete response and has remained free of disease for 30 months.
Discussion
Metastatic SCC of the head and neck from a clinically occult primary site of disease is unusual, accounting for less than 5% of all cases of head and neck SCC. In this situation, approximately 30% of identifiable primary tumors are found in tonsillectomy specimens (3–5). The recommended workup in these patients without an obvious primary tumor includes cross-sectional imaging (CT scanning or MR imaging) and panendoscopy (laryngoscopy, bronchoscopy, and esophagoscopy) with directed biopsies. Because small primary tumors can exist deep in the palatine tonsillar crypts, tonsillectomy may be performed rather than “random” tonsillar biopsies to exclude the tonsil as a primary site of disease (3). Because contralateral spread of metastatic cancer from occult tonsil lesions has been reported (4), bilateral tonsillectomy is advocated by some as part of a complete workup for metastatic cervical lymphadenopathy from an unknown primary tumor.
We report the cases of two patients who presented with metastatic SCC in upper cervical lymph nodes who had MR imaging studies showing ipsilateral palatine tonsils that were decreased in size and T2 signal intensity as compared with the contralateral side. Both patients underwent tonsillectomy proving that the primary lesion was in the smaller, hypointense tonsil. These cases stand in contrast to the “typical” MR imaging appearance of palatine tonsil SCC (1).
MR imaging, with its multiplanar imaging capability and excellent soft tissue contrast, is generally considered the method of choice for evaluating the patient with SCC of the oropharynx (1), although many use CT scanning for this purpose. Typically the tonsil with cancer will be enlarged (6). Carcinoma is mildly hypointense or isointense relative to normal lymphoid tissue on T1-weighted images, which can make differentiation from surrounding muscle difficult (7). On T2-weighted images, however, the tumor is usually hyperintense, allowing differentiation from adjacent normal lymphoid tissue and muscle (8). Furthermore, carcinomas tend to enhance after gadolinium administration (9).
The reason for the somewhat unusual imaging characteristics in our two patients is unknown. It would seem that the histologic findings of the primary tumor, such as high cellularity or fibrous elements, should explain the diminished size, low T2 signal intensity, and relative lack of enhancement. However, review of the pathologic specimens in the two cases with tonsillectomy was unrevealing, with moderate fibrosis in one case but no significant fibrosis in the other. It is also possible that the degree of cellular differentiation may influence the T2 signal intensity in the same way that tumors with a high nuclear-cytoplasmic ratio tend to have low to intermediate T2 signal intensity. The identification of additional cases may shed more light on this issue as more pathologic specimens are acquired.
Conclusion
The identification of a primary mucosal lesion in the patient who presents with a cervical nodal metastasis has a number of clinical benefits (3, 4). It allows the patient to weigh therapeutic options (surgery versus radiation therapy or chemotherapy or both) and influences the way in which radiation therapy will be targeted. If the nasopharynx and contralateral parotid gland can be spared, radiation-related complications such as xerostomia can be reduced. The identification of a primary site also improves post-treatment surveillance for recurrent disease, because it focuses clinical and imaging attention on the known primary site. MR imaging is an important adjunct to clinical staging for SCC of the palatine tonsil, and it is important to recognize the “small, dark tonsil” as a potential indicator of a primary site in the patient who has SCC metastatic to the neck with a clinically unknown primary lesion.
References
- Received April 21, 2004.
- Accepted after revision May 19, 2004.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.