
Abstract
Summary: We compared the diagnostic accuracy of lumbar facet blocks guided by either conventional fluoroscopy or CT fluoroscopy (CTF). Seventy-one blocks were performed with conventional fluoroscopy, and 58 were performed using CTF. Pain scores were measured before and after the procedure. The CTF group had a greater percentage decrease in pain (79.5% ± 31.1%) than did the conventional fluoroscopy group (55.5% ± 38.0%; P < .0005). We conclude lumbar facet blocks by using CTF guidance results in greater diagnostic accuracy than do conventional fluoroscopy.
Lumbar facet joint degeneration is a common contributor to lower back pain that can be difficult to diagnose, because there are no specific markers of facet joint related pain. In addition, imaging studies have not shown a correlation between clinical and radiopathologic findings (1). Diagnosis and treatment of facet joint syndrome is done by facet joint anesthetic block. This is generally done by fluoroscopy or CT guidance and involves median branch nerve injections or intraarticular injections of anesthetic and steroids. CT fluoroscopy (CTF) has the potential to improve the efficacy of lumbar facet block injections. CT is an imaging technique commonly used during interventional procedures because it offers exceptional contrast and spatial resolution. Unlike sonography and conventional radiographic fluoroscopy, however, conventional CT is unable to provide real-time guidance capability, which results in longer procedure times because multiple CT scans are needed to confirm appropriate needle or catheter position. Recent advances in CT technology have lead to the development of new applications for CTF. These imaging modalities were first reported by Katada et al (2–4) and Kato et al (5, 6) in the mid-1990s and have since developed into powerful imaging tools with widespread application (6–10). The benefits of CT fluoroscopy as compared with conventional fluoroscopy for facet block injections have not been demonstrated, to the best of our knowledge. We used CT fluoroscopy to guide lumbar facet block injections and evaluated whether using this method would improve diagnostic accuracy and pain relief as compared with conventional fluoroscopy.
Description of Technique
We have used CT fluoroscopy on a daily basis for the past 2 years. We used three evolutions of Acquilion Multi Detector Computational Tomography scanners (MDCT): a 4 detector, 8 detector, and 16 detector with a 0.5-second rotation. All provide the same CTF technique. Our CT scanner can be run by the operator from the tableside during a procedure, similar to an angiography suite. The equipment is operated from in-room controls as a needle is passed down to the facet and steroids or local anesthesia are injected. Three sections are acquired, and each is displayed simultaneously at 13 frames/s (a total of 39 frames/s). This allows the needle to be tracked during the procedure. Two operational settings or modes can be used during CT fluoroscopy: a continuous mode and an intermittent mode. The continuous mode offers for real-time imaging capabilities, allowing visualization of the needle tip or catheter throughout the procedure, while the intermittent mode provides spot images that allow the operator to periodically locate needle tip or catheter position in a manner similar to conventional CT. The two operational modes can be used alone or in any combination during interventional procedures, and both have been well documented (7, 8). Although the continuous mode offers the optimal visualization during a procedure, it results in greater radiation dosages to both operator and patient (9, 10). As a result, this operational mode is usually reserved for interventional procedures in which a high value is placed on being able to localize the needle or catheter position at all times, such as the biopsy of small pulmonary nodules, transbronchial biopsies, or biopsies or drainages where the lesion is in the vicinity of vital structures. For most routine biopsies, drainages, and spinal procedures such as facet blocks, nerve root blocks, and epidural injections, the intermittent mode is used because it provides sufficient spatial resolution and results in less radiation to operator and patient (9, 10).
We conducted a retrospective study of 129 lumbar facet blocks performed on 98 patients over a 2-year period. Fifty-eight procedures were performed with CT fluoroscopy (19 females, 18 males; average age, 59.0 ± 15.6 years; age range, 27–88 years), and 71 procedures with conventional fluoroscopy (38 females, 22 males; average age, 56.0 ± 17.4 years; age range, 16–100 years). One hundred nineteen procedures were bilateral. The average number of levels done on each patient was 2.1 ± 0.8.
A numerical rating scale was used to quantify pain (11). Patients were asked to rate their pain before and immediately after the procedure on a scale of 0 to 10, with 0 indicating no pain at all and 10 indicating the worst pain imaginable.
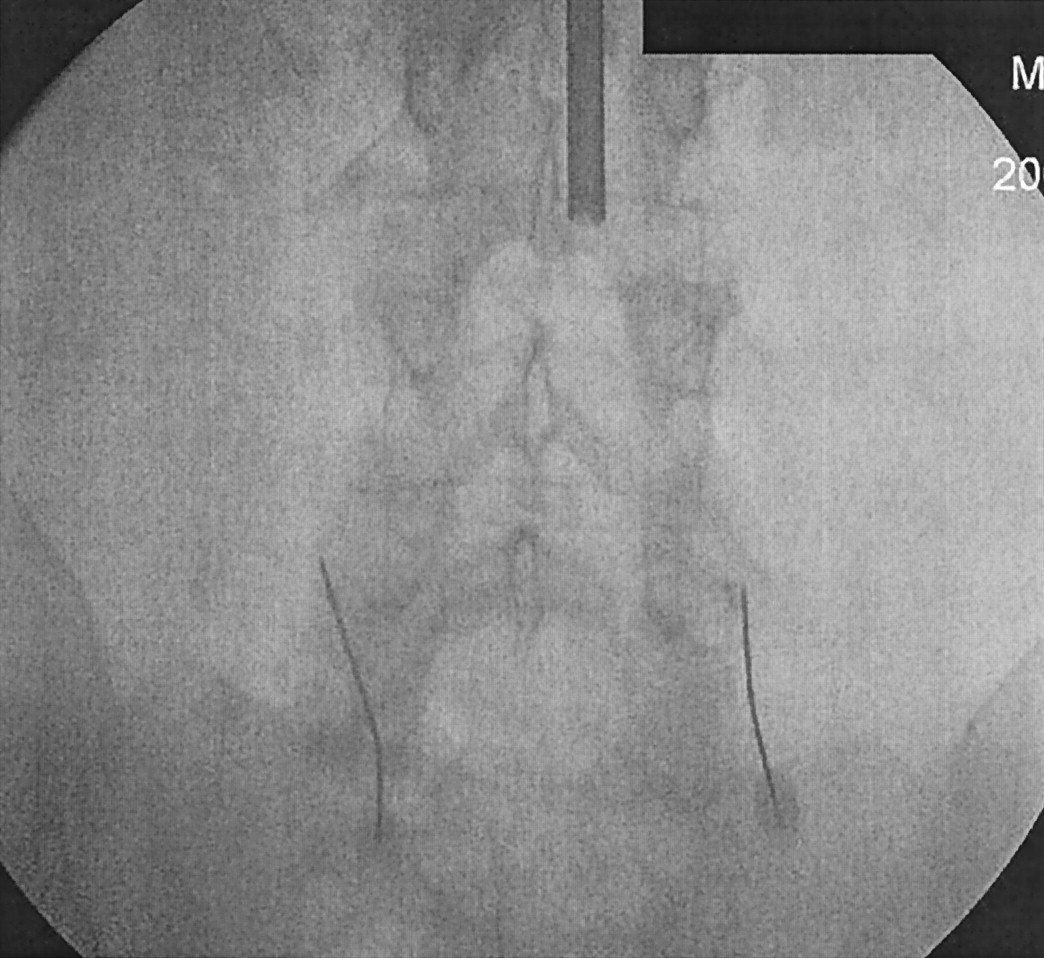
All procedures were performed by the primary author, who is well experienced in both methods. All radiologists and nurses wore protective lead aprons. A spiral CT of the region of interest was done. CT fluoroscopic parameters were chosen (120 kVp, 50 mA). Patients were placed in prone position, and the overlying skin was sterilized. The facet joint was localized using either conventional or CT fluoroscopy. Once localized, a 22-gauge, 3.5-inch needle was directed into the desired facet joint. One needle was used per joint. During CTF, diagnostic accuracy was achieved by ensuring that the position of the tip of the needle was within 5 mm from the superior aspect of the facet of the lumbar spine (Fig 1). For conventional fluoroscopy, the needle tip was placed at the junction between the facet joint and transverse process of the corresponding level (Fig 2). Contrast injections were not used to localize the needles. Once the needles were in place, 1 mL of bupivicane (0.5%) was injected into the joint.
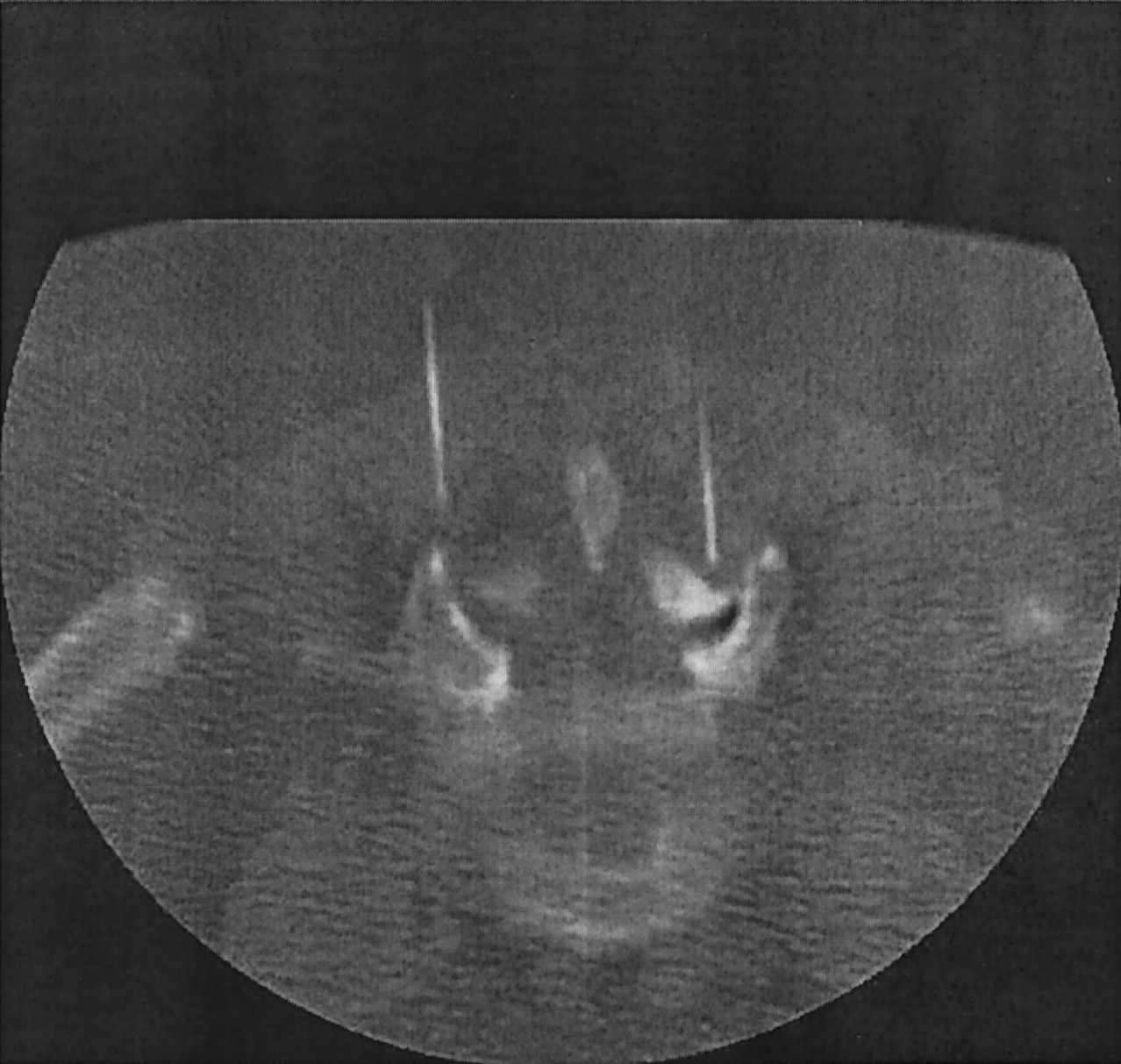
Lumbar facet block at L4–L5 by using CTF.

Lumbar facet block at L4–L5 by using conventional fluoroscopy.
Discussion
Analysis of mean preprocedure pain scores between the two groups revealed no significant difference; however, the mean postprocedure pain score of the CTF group was significantly lower than the conventional fluoroscopy group. The CTF group also had a significantly larger mean percentage decrease in pain following the procedure (Table).
Comparison of pain scores between both study groups
Lumbar facet degeneration is a common cause of lower back pain that is not easily diagnosed or treated. Facet-related pain is difficult to diagnose, in view of the lack of specific clinical or radiologic findings (1). Diagnosis and treatment have traditionally been done by facet block injections, using fluoroscopy or CT-guidance as imaging modalities during the procedures. The value of facet injections has been debated in the literature. In studies of the therapeutic benefit of intraarticular injections, results have varied, with pain relief ranging from 13% to 90% (12, 13).
CTF is an imaging technique that has the potential of increasing the diagnostic accuracy and treatment of lumbar facet pain. CT fluoroscopy offers the spatial resolution of conventional CT with the real-time capabilities of sonography and thus provides numerous benefits during interventional procedures. Like sonography, CT fluoroscopy allows for the visualization of the needle tip or catheter tip throughout interventional procedures, but with greater contrast and spatial resolution.
Our results show a significant decrease in pain following lumbar facet injection. This was most likely due to increased specificity of needle placement. With the use of CT fluoroscopy, we were able to place needles directly into the facet joint, resulting in improved diagnostic accuracy and pain relief.
Another benefit of CT fluoroscopy is the reduction in needle placement times during interventional procedures when compared with the same procedures performed by using conventional CT (8). Although procedure times for the facet blocks were not recorded, other procedures at our hospital using CTF have had procedure times reduced by as much as 50%, and reports from other institutions show similar reductions in procedure times (3–9). This is due primarily because the physician performing the procedure is able to monitor the location of the needle or catheter at the patient’s side. During interventional procedures in which conventional CT is used, needle localization requires the physician to leave the room to perform a spot-check scan, resulting in longer procedure times.
One risk associated with CT fluoroscopy is the potential for increased radiation exposure to patients and physicians. Typical radiation exposure factors during CT fluoroscopy were 80–120 kVp and 30–50 mA/s, with radiation dosage rates ranging between 20–60 Gy/min (4–6). Although Nawfel et al (14) reported radiation exposure in excess of conventional CT, several other studies have shown that radiation dose to the patient can actually be reduced. Studies conducted at the Mayo Clinic by Carlson et al (15) reported a 94% decrease in patient absorbed dose when CT fluoroscopy was compared with conventional CT. The use of the intermittent technique and low fluoroscopic parameters used during procedures were the primary reasons for this. To help reduce radiation exposure to physicians, several strategies have emerged. The use of lead aprons and lead shields can lower radiation exposure dramatically. Use of needle holders during the procedure, which avoids placing hands directly into the conventional radiographic beams, has also been shown to reduce radiation dosages significantly (9).
Conclusion
Our results indicate that CTF increases the diagnostic accuracy and therapeutic effect of lumbar facet blocks by allowing for increased specificity of needle placement. It also has the potential for decreasing procedure times and radiation exposure, benefiting both the patient and the practitioner. As this technology improves, its application will most likely increase in the future.
- Received July 9, 2004.
- Accepted after revision November 11, 2004.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- CT-Guided Lumbar Nerve Root Injections: Are We Using the Correct Radiation Dose Settings?
- Role of Facet Joints in Spine Pain and Image-Guided Treatment: A Review
- The Lumbar Multifidus Muscles are Affected by Medial Branch Interventions for Facet Joint Syndrome: Potential Problems and Proposal of a Pericapsular Infiltration Technique
- Intra-articular injection composed of steroid, iohexol and local anaesthetic -- is it stable?