
Abstract
Summary: Primary cartilaginous lesions of the larynx are relatively uncommon. We present a case of bilaterally pseudocystic lesion of the thyroid cartilage that demonstrated progressive calcification. Pathologic analysis showed features suggesting a dystrophic lesion with no evidence of malignancy. We hypothesize that repetitive microtrauma related to muscular overuse probably led to inflammatory changes at tendinous insertions on the laryngeal cartilage and resulted in dystrophic ossification of the laryngeal cartilage.
Primary lesions of the laryngeal cartilages are rare, with the most common being chondromas and chondrosarcomas. Their endolaryngeal growth produces dyspnea and hoarseness. These tumors arise from the cartilages of the larynx, most commonly cricoid and thyroid. Inflammatory lesions of the larynx are not well characterized in the imaging literature. Distinguishing between infectious and inflammatory lesions from neoplasms may be very difficult.
Case Report
A 42-year-old nonsmoking female who had a 6-month history of dysphonia was examined. No dyspnea or dysphagia was noted. She had recently been experiencing increased signs of voice fatigue, especially at the end of the day, associated with overuse of her speaking voice. This symptom reduced her quality of life, particularly in her work as an executive manager. She had no history of inflammatory changes involving muscles, tendons, or joints.
Laryngoscopy demonstrated bilateral reddish swelling of the anterolateral larynx wall bilaterally at the level of the false vocal cords, with smooth overlying mucosa. An outside unenhanced CT examination revealed a bilateral circumscribed homogenous hypoattenuated lesion located at the level of the thyroid cartilage. A mass effect on the false vocal cords was seen. The airway lumen was asymmetric (Fig 1). This appearance raised the question of bilateral fluid-filled laryngoceles. Laryngeal MR imaging was performed to exclude an occult laryngeal ventricule tumor. MR imaging showed a homogenous hypointensity on T1-weighted images (Fig 2A) with a marked signal intensity increase on T2-weighted sequences (Fig 2B). The lesion was centered in the thyroid cartilage rather than within the laryngeal lumen. There were no intra- or extralaryngeal tumor growth, and no lymph node enlargement was noted. The location of the lesion suggested a thyroid cartilage origin. Conventional radiographs of hands, feet, and the cervical spinal were systematically taken, which showed no evidence of inflammatory bone or joint disease. In addition, a 99-Technetium radionuclide study revealed no abnormal bone activity. Therefore, an annual imaging follow-up of the thyroid cartilage lesion was planned.

Postcontrast CT scan at the level of the false vocal cords showing bilateral circumscribed, homogeneous, low-signal-intensity lesions of the thyroid cartilage (arrows).

A, Precontrast axial spin-echo T1-weighted image showing a homogenous soft tissue mass (arrows), isointense to muscle, and located in the wall of the larynx lateral to the pre-epiglottic fat, medially to laryngeal muscle strap.
B, Axial fast spin-echo T2-weighted image at the level of the false vocal cords, showing a pronounced high signal intensity of the bilateral well-circumscribed lesion of the thyroid cartilage (arrowheads).
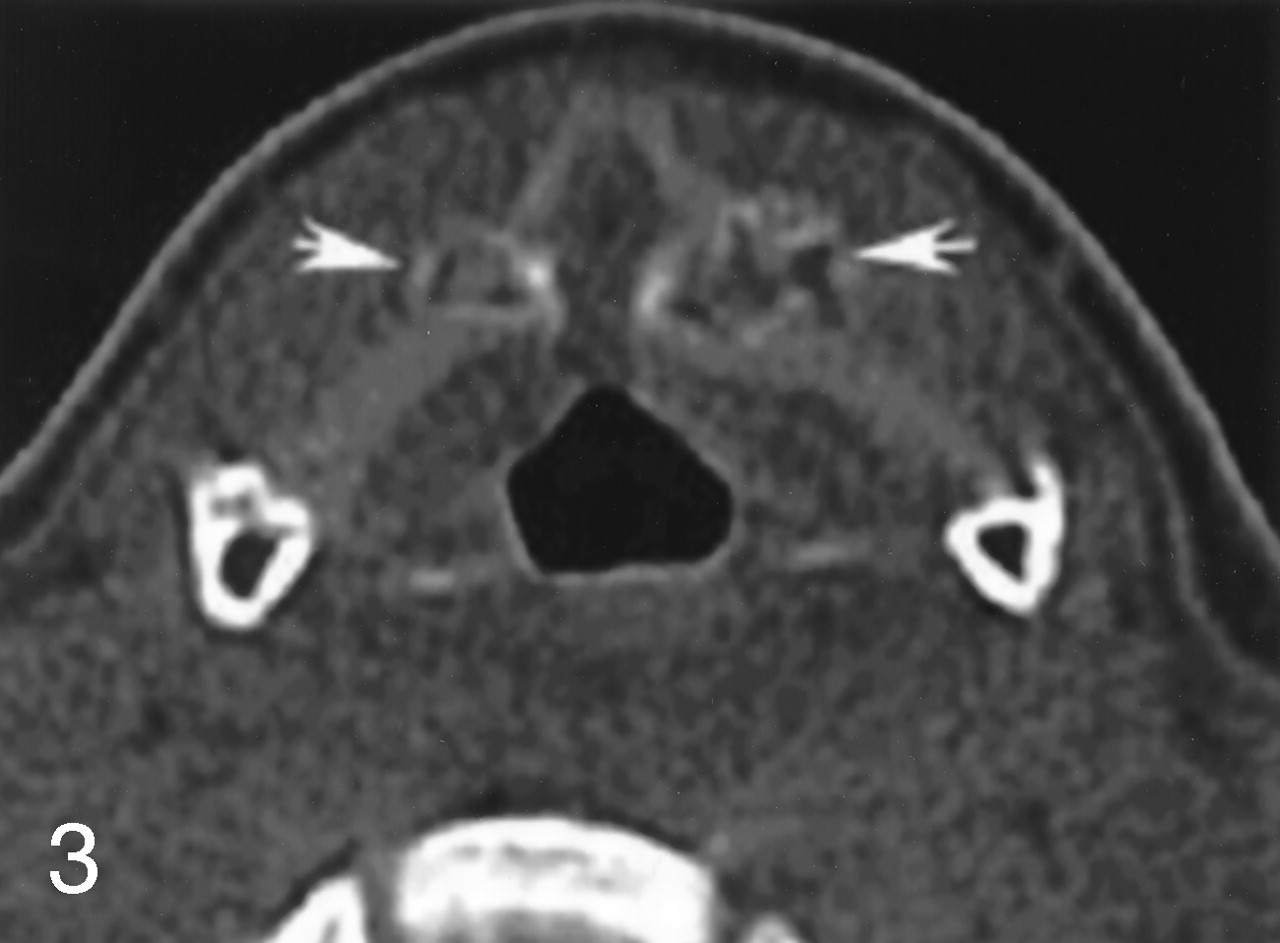
On a 2-year follow-up CT scan, the lesion demonstrated progressive calcification (Fig 3). Lesion enhancement was demonstrated on postgadolinium T1-weighted images with fat saturation (Fig 4).

CT scan image taken 2 years after the initial examination, showing the progressive calcification of the lesion, with a cartilaginous matrix aspect (arrows). Note the relationship of the lesion to the noncalcified thyroid plate.
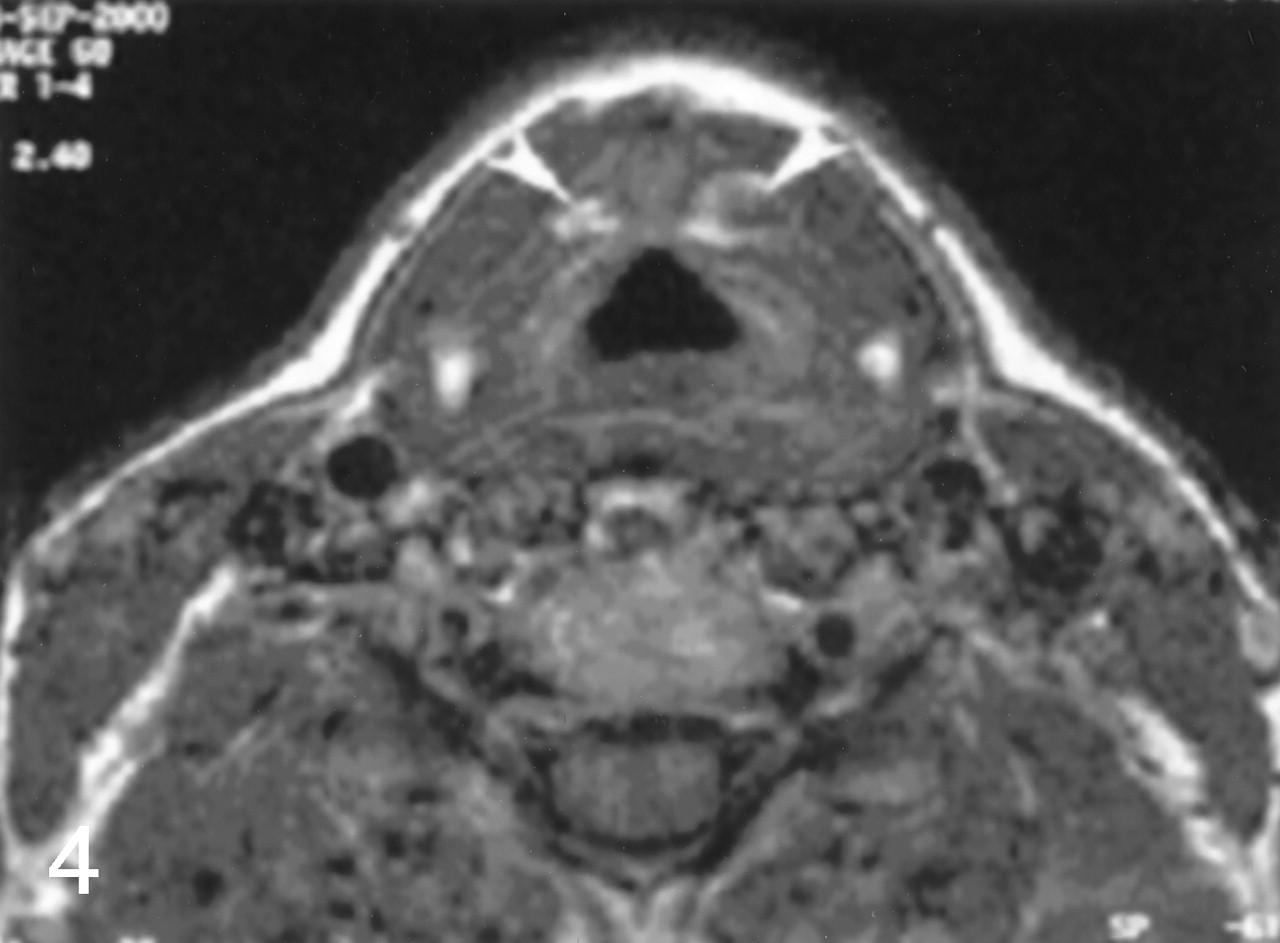
Fat saturation postcontrast axial spin-echo T1-weighted image showing a bilateral pronounced enhancement of the thyroid cartilage (arrowheads).
Over a 4-year period, the lesion persisted unchanged, with no evidence of aggressive behavior or malignant degeneration. A partial laryngectomy was performed 5 years after the initial examination, because of the persistence of the lesion and the patient’s preference. A 2-year clinical and imaging follow-up revealed rehabilitation of vocal function and no tumor recurrence.
Histologic examination showed bilateral circumscribed areas of cartilaginous and bone dystrophia, with no evidence of malignancy. The dystrophic bony tissue was filled with a cartilaginous matrix, with a normally ossified bone trabeculum. The trabeculae were in a disorganized pattern.
Discussion
When a submucosal mass is identified in the larynx, a cartilage lesion must be considered. T2-weighted images can be misleading with regard to differential diagnosis, because the cartilaginous lesions can be hyperintense, thus suggesting a fluid-filled cyst such as a laryngocele.
Cartilaginous tumors of the larynx account for <1% of laryngeal neoplasms. In 70% of cases, the site of origin is the cricoid cartilage, followed by the thyroid cartilage, which occurs in 20% of cases (1). Chondroid lesions arising from other laryngeal sites are uncommon. Most patients with laryngeal cartilaginous tumors are male (3:1 male-to-female ratio) between their 6th and 7th decades of life (2). Their etiology is unknown. One hypothesis suggests abnormalities in the development of ossification of laryngeal cartilage, a process that begins at the age of 4 years. Usually, cartilaginous tumors of the larynx grow slowly and have only local aggressiveness. Their main clinical symptoms are alteration of the voice, dyspnea, and dysphagia (3). Histologic examination reveals either chondromas or chondrosarcomas of various grades; however, the histologic difference between a benign chondroma and a low-grade chondrocarcinoma is often impossible to establish (4).
In the reported case, the symmetrical development did not point to a cartilaginous tumor. Furthermore, the progressive calcification of the lesion raised the possibility of a mechanical or inflammatory process occurring at a tendinous insertion.
The laryngeal cartilages are hyaline cartilage, except for the fibroelastic cartilage of the epiglottis. Hyaline cartilages undergo change over time, with progressive enchondral ossification (5, 6). There is wide variation between the age of an individual and the stages of calcification of the laryngeal cartilage. Nevertheless, calcifications progressively progress with age. Moreover, the order of ossification of laryngeal cartilages correlates with the distribution of the mechanical forces applied to the larynx cartilages (6). Therefore, we hypothesized a mechanism that would involve repeated microtrauma or overuse of the extralaryngeal muscles, leading to a progressive ossification at the tendinous insertions of the muscles. The gadolinium uptake indeed suggests the possibility of a component of inflammation and chondritis but is nonspecific.
The tendinous insertions present on the surface of the thyroid plate include, in the outside part the sternothyroid muscle, the thyrohyoid muscle, and the thyropharyngeal part of the inferior constrictor muscle of the pharynx, and in the inner part the cricothyroid muscle (7). At the mid-third of the thyroid plate, there is an oblique insertion line with a tubercle at each end. A tendinous arch extends between the two tubercula. Both the thyrohyoid muscle anteriorly and the thyropharyngeal part of the inferior constrictor muscle of the pharynx posteriorly have insertions on this oblique line, the tubercle and the tendinous arch. The sternothyroid muscle attached on the tendinous arch, and the tubercles has no insertion into the oblique line (8). The inconstant external part of the cricothyroid muscle is attached to the lowest edge of the thyroid plate.
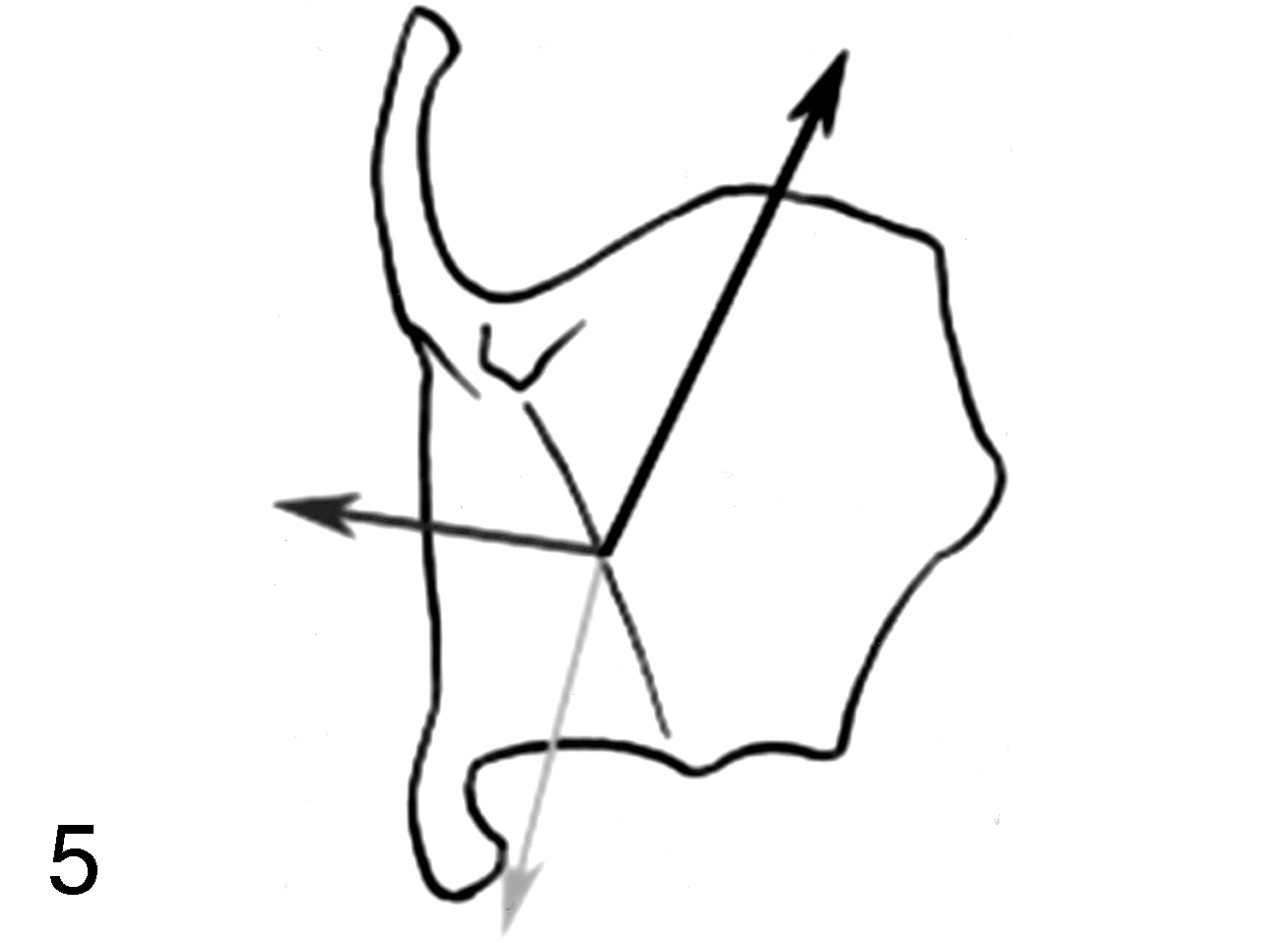
These muscles have antagonist functions: the thyrohyoid muscle raises the larynx, whereas the sternothyroid muscle depresses it. The thyropharyngeal part of the inferior constrictor muscle of the pharynx constricts the lower part of the pharynx (9). They all act during swallowing. Therefore, the oblique line, the tuberculum, and the tendinous arch make up areas of multiple muscular insertions acting with opposite mechanical forces (Fig 5).

Schematic representation of the mechanical forces in the area of muscular insertion of the thyroid plate (external side). The black arrow illustrates the thyrohyoid muscle force, the dark gray arrow the thyropharyngeal part of the inferior constrictor muscle of the pharynx, and the light gray arrow the sternothyroid muscle.
Because the location of the dystrophic lesion corresponded to the thyroid area of muscular insertion of the oblique line, we believe that these muscular mechanical forces are implicated in the origin of the pseudotumor described above. Moreover, the inflammatory process located at the muscular insertion could lead to a rapid and abnormal ossification of the thyroid plate. Osteosclerosis of the arytenoid cartilage has been reported, following chronic inflammation of the perichondrium at the base of a vocal granuloma (10).
Thus, we can postulate that bilateral masses circumscribed within the thyroid cartilage—without a midline connection, but showing a cartilaginous pattern on MR imaging examination and demonstrating progressive calcification—should not be surgically removed unless they significantly interfere with voice or breathing.
Conclusion
The exact anatomic location is the key point in diagnostic assessment when evaluating a cartilaginous laryngeal mass. Distinguishing a chondroid lesion from a dystrophic one cannot be based on postcontrast enhancement alone. In fact, bilaterality, midline symmetry, and absence of size increase at periodic evaluations should suggest the diagnosis of a dystrophic cartilage lesion.
Acknowledgments
We thank Hugh D. Curtin, PhD, for his helful suggestions, which allowed us to complete this article, and Mrs. Linda Northrup, for her help in preparing the English-language text.
References
- Received August 12, 2003.
- Accepted after revision September 6, 2004.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.