
Abstract
SUMMARY: Subarachnoid hemorrhage (SAH) is a recognized presentation of Moyamoya disease in adults. Because there are extensive collateral networks and potential complications that develop, a thorough investigation of the intracranial and extracranial circulation is necessary to exclude a treatable cause when these patients present with SAH. We present a case of SAH due to a ruptured pseudoaneurysm of the anterior spinal artery arising from the supreme intercostal artery, which was the sole source of blood supply to the intracranial circulation.
Moyamoya disease is a cerebrovascular condition characterized by narrowing or occlusion of the supraclinoid internal carotid arteries and proximal middle and anterior cerebral arteries. Subsequent development of extensive collateral vessels defines the disease. Subarachnoid hemorrhage (SAH) is a common presentation in adults with Moyamoya disease, and atypical aneurysms arising from varied locations can be the source of such hemorrhage.
Case Report
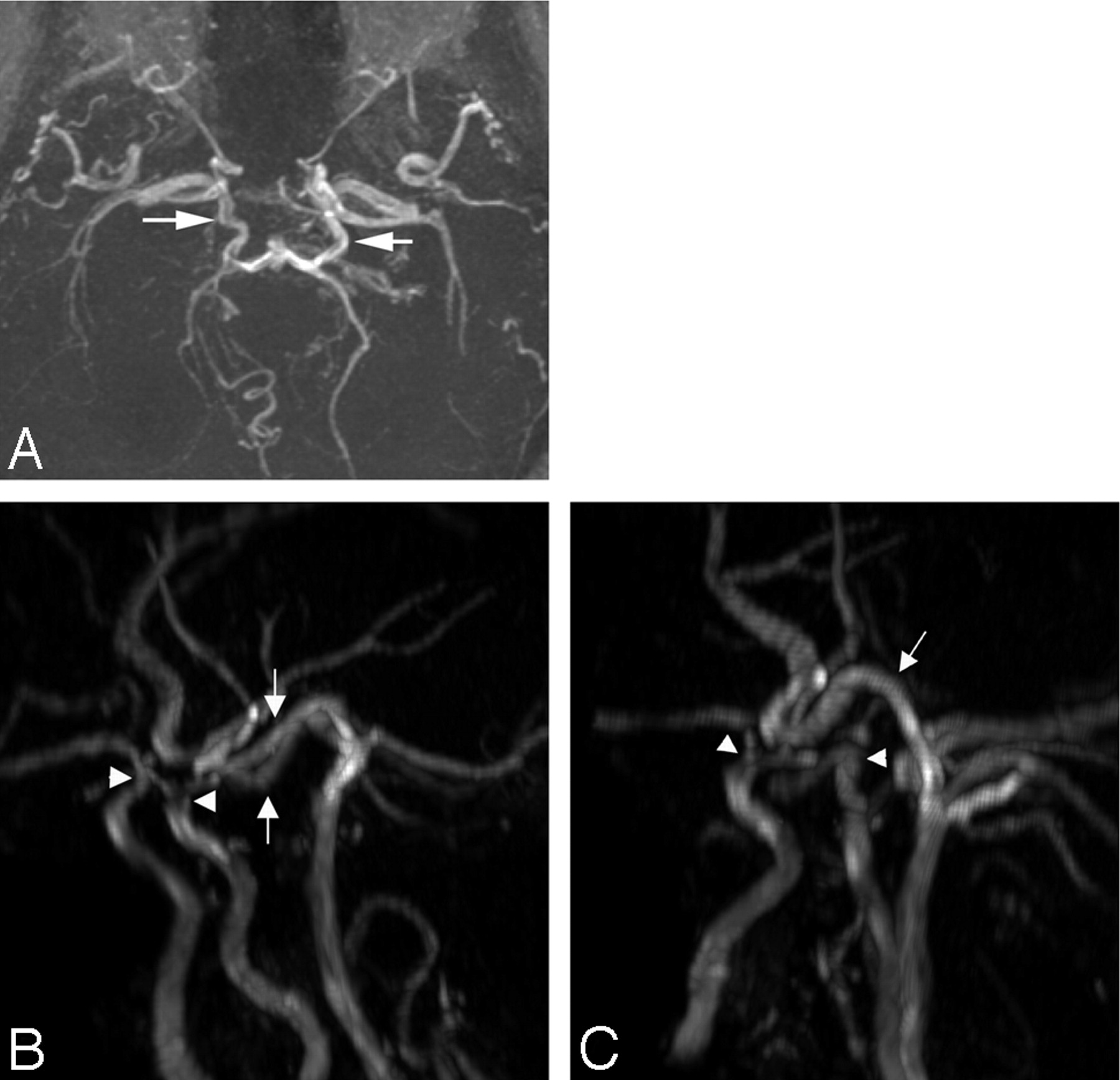
A 58-year-old man of Middle Eastern descent presented to the emergency department of a neighboring institution with headache and was found on noncontrast CT to have diffuse SAH. A catheter angiogram was then performed, which revealed Moyamoya-type vascularity but no intracranial aneurysm (Fig 1). The posterior circulation could not be evaluated, because of an inability to catheterize the vertebral arteries bilaterally. Therefore, following the angiogram, MR imaging and MR angiography (MRA) were performed revealing supraclinoid carotid occlusive disease with a patent basilar artery. Prominent posterior communicating arteries were present bilaterally, which enabled the basilar artery to be the sole feeding vessel to both the anterior and posterior circulations (Fig 2).

Lateral views from digital subtraction angiography with selective injection of the left (A) and right (B) internal carotid arteries reveals bilateral supraclinoid occlusion of the internal carotid arteries with prominent collaterals via the ophthalmic artery, the meningohypophyseal trunk, and hypertrophied lenticulostriates.

MRA 3D time-of-flight technique (A) demonstrates hypertrophied posterior communicating arteries (white arrows) feeding the anterior circulation. Lateral oblique views (B and C) by use of a Vitrea workstation once again demonstrate prominence of the posterior communicating arteries (white arrows) as well as evidence of occlusive disease involving the internal carotid arteries bilaterally (white arrowheads).
The patient’s hospitalization was complicated by recurrent episodes of SAH with the eventual development of hydrocephalus followed by hemiplegia and then quadriplegia. MR imaging of the cervical spine was then performed, which revealed an intradural mass compressing and resulting in edema of the cord at the C3–C4 level (Fig 3).

Sagittal and axial (A and B) T1-weighted images of the cervical spine reveal a mixed signal intensity intradural mass at approximately the level of C4. This mass appears to contain blood products of varying age. Postgadolinium sagittal and axial (C and D) sequences reveal vague peripheral enhancement around the intradural mass.
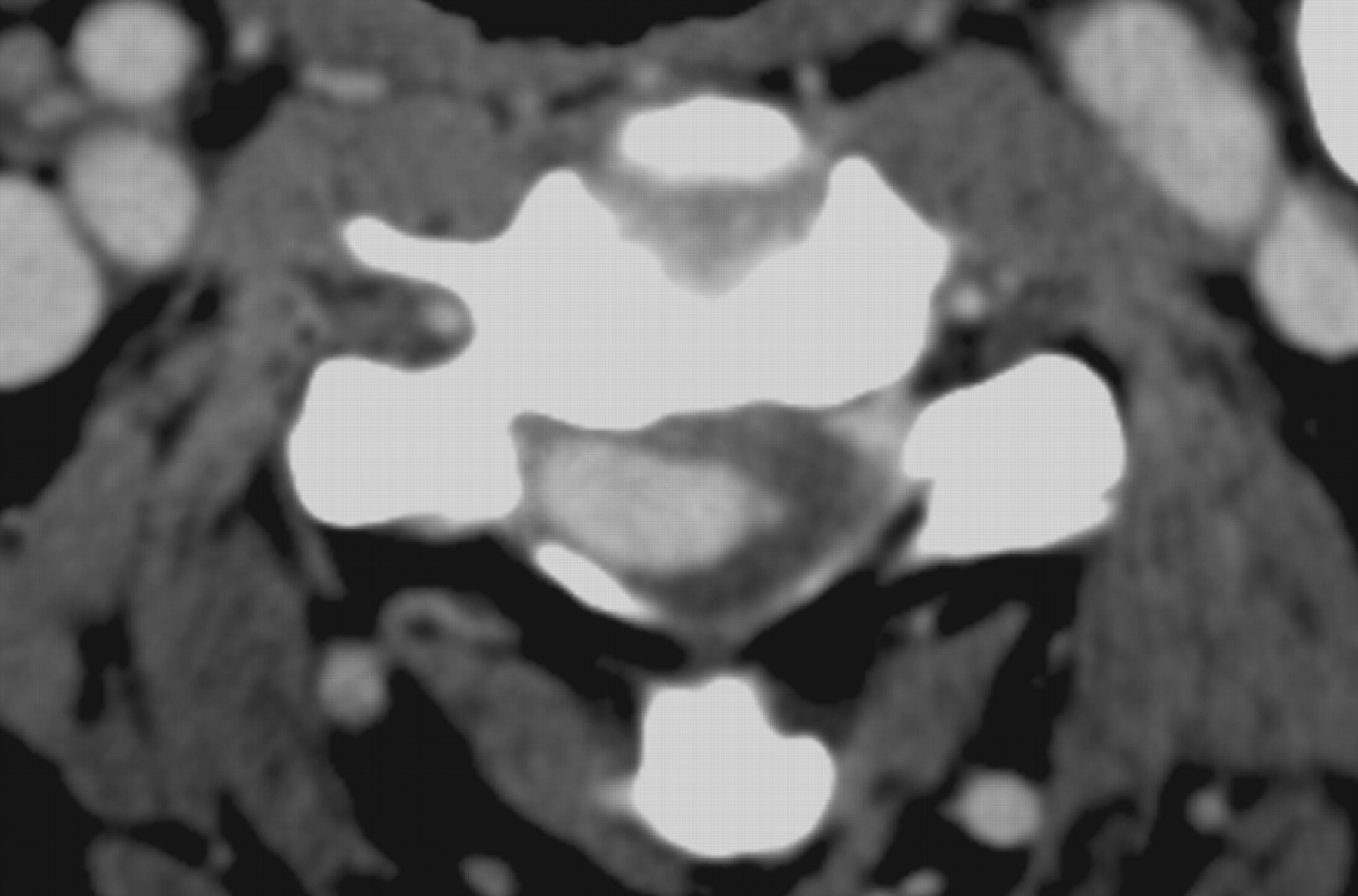
This mass demonstrated mixed signal intensity on T1- and T2-weighted images and was felt to represent blood products of varying age. CT angiography was performed and demonstrated a high attenuation, homogeneously enhancing vascular structure centered within the spinal canal compressing the cord (Fig 4). 3D reconstruction by use of the Vitrea workstation (Vital Images, Minnetonka, Minn) demonstrated this vascular mass arising from what appeared to be a markedly enlarged anterior spinal artery (Fig 5). The origin and distal route of this vessel were not identified on the CT angiogram.

Axial source image from a CT angiogram reveals an attenuated homogeneously enhancing mass at the C4 level. The enhancement pattern matches that of the carotid vessels, which indicates the vascular nature of this lesion.

Reconstructed 3D image by use of a Vitrea workstation demonstrates an irregularly shaped aneurysm arising from an enlarged anterior spinal artery.
A repeat angiogram was performed and once again revealed Moyamoya vascularity and no intracranial source of SAH. Investigation of the vasculature of the neck revealed an enlarged anterior spinal artery arising from the supreme intercostal artery as the sole feeding vessel to the basilar artery. The anterior spinal artery was markedly enlarged and contained a 1.1 × 1.1 cm irregular bilobed pseudoaneurysm in the location of the enhancing mass seen compressing the spinal cord on the CT angiogram and MR imaging (Fig 6).
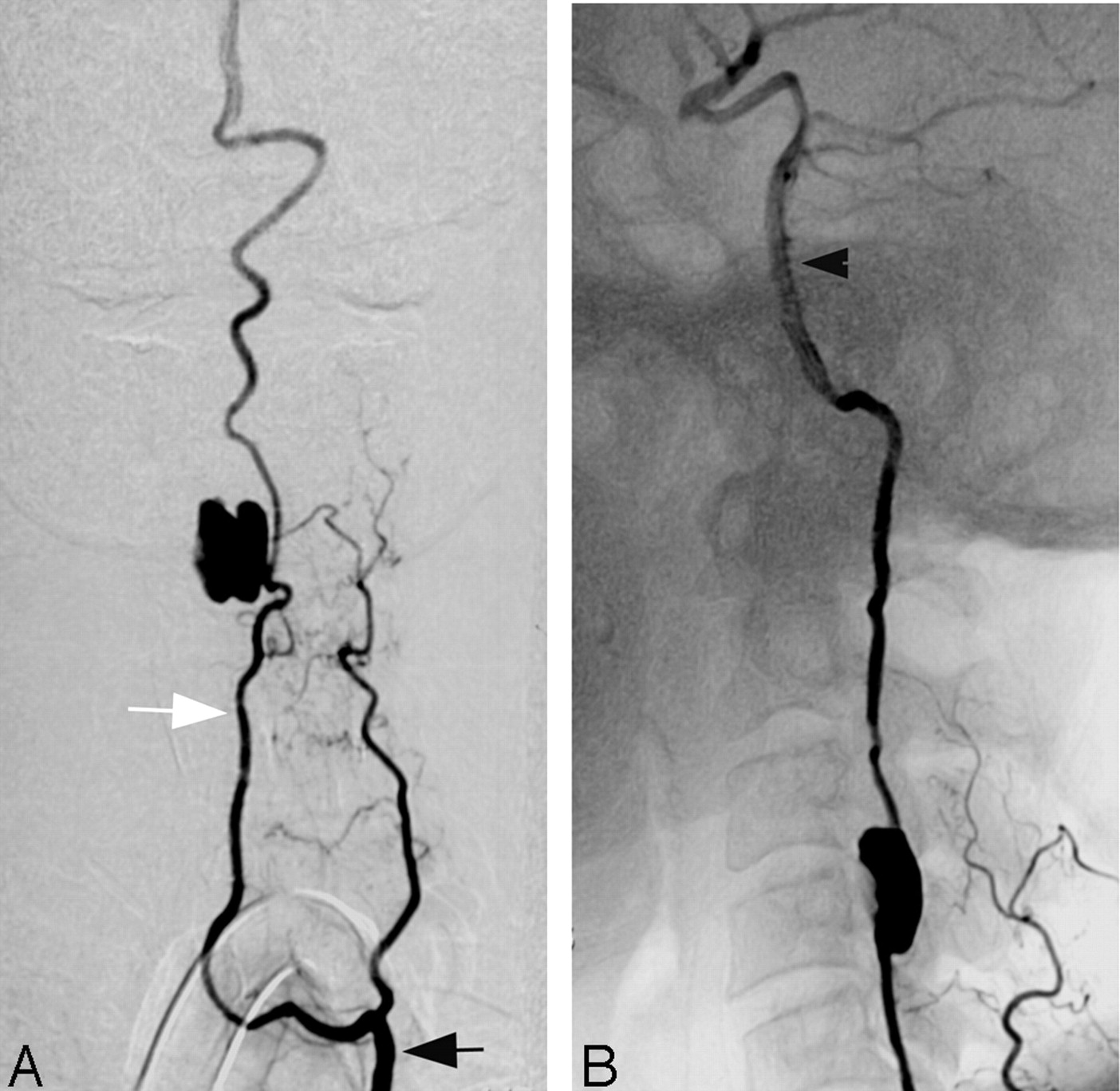
Digital subtraction angiography frontal (A) and lateral (B) projections with injection of the supreme intercostal artery (black arrow) reveal an enlarged anterior spinal artery (white arrow) arising from the supreme intercostal artery feeding the basilar artery (black arrowhead) and the intracranial circulation. A bilobed pseudoaneurysm is seen arising from the anterior spinal artery.
The findings and treatment options were discussed with the patient’s family and the neurosurgical team, and endovascular obliteration of the pseudoaneurysm was chosen as the treatment. The patient’s dire clinical condition played a major role in the decision to treat the aneurysm endovascularly, rather than surgically, because the neurosurgical team did not consider the patient a good candidate for surgery. The patient returned to the interventional neuroradiology suite the following day. The pseudoaneurysm was treated by using a combination of platinum, Hydrogel (MicroVention, Aliso Viejo, Calif), and Matrix (Boston Scientific/Target, Fremont, Calif) coils. Postembolization images revealed complete obliteration of the bilobed aneurysm with continued patency of the anterior spinal artery (Fig 7A and -B). The patient recovered only minimally but, to our knowledge, has not suffered any repeat episodes of intracranial hemorrhage.
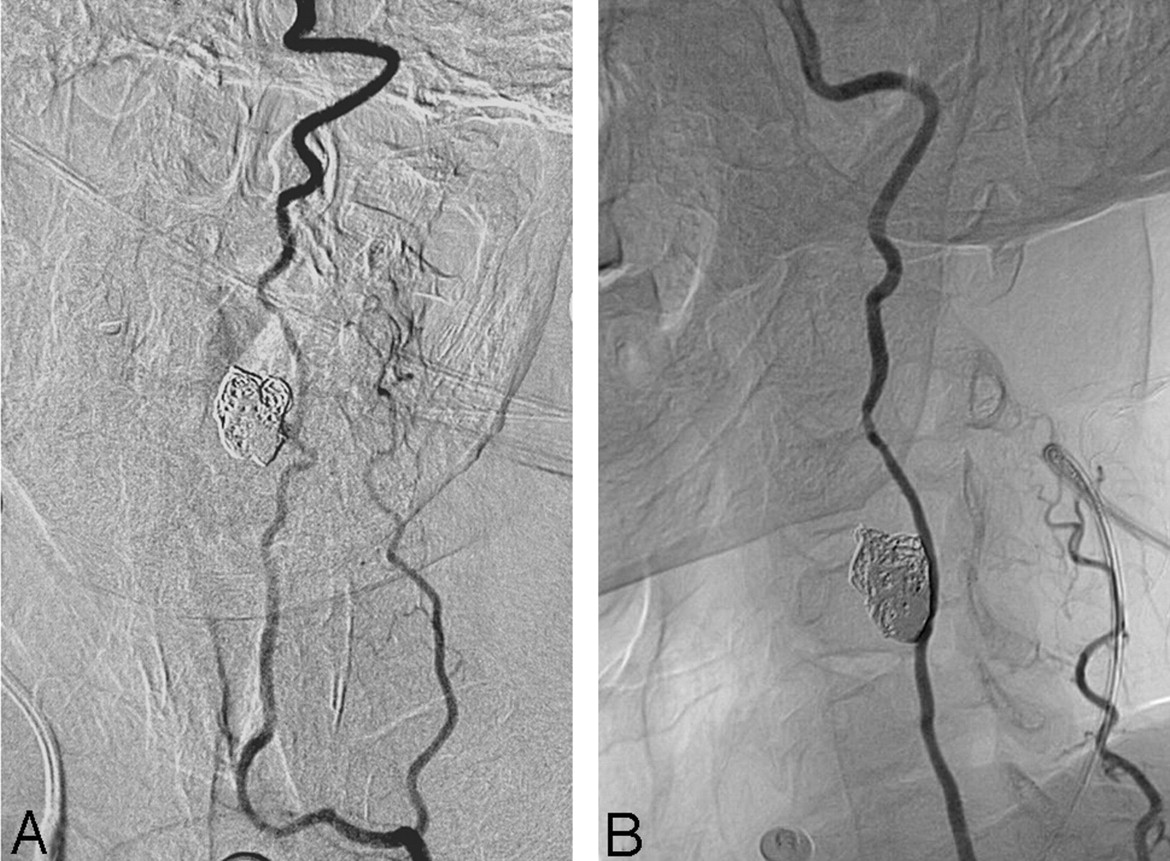
Postembolization digital subtraction angiography images in the frontal (A) and lateral (B) projections reveal a coil mass and complete obliteration of the previously noted pseudoaneurysm. Continued patency of the anterior spinal artery is demonstrated.
Discussion
Moyamoya is a rare cerebrovascular disease characterized by progressive bilateral supraclinoid internal cerebral artery occlusion extending to the anterior and middle cerebral arteries.1,2 As a result, parenchymal, leptomeningeal, and transdural collateral or Moyamoya vessels develop. Yamada et al have shown that the posterior circulation is also affected in patients with Moyamoya and that these lesions increase in frequency along with the severity of the internal carotid artery stenosis.3 Posterior cerebral artery lesions are not currently part of the criteria for diagnosis of Moyamoya disease. Numerous case reports have reported unusual collateral formation and aneurysm development in patients with Moyamoya.4-6 Our case demonstrates a dominant collateral to the posterior circulation from the anterior spinal artery via the supreme intercostal artery with subsequent development of a pseudoaneurysm of the anterior spinal artery. This was a most unusual source of SAH in this patient with Moyamoya that eluded detection until the catastrophic development of quadriplegia necessitated detailed evaluation of the extracranial circulation.
Ischemia is the most common presentation of Moyamoya in children, whereas adults more often present with intracranial hemorrhage.7,8 Aneurysm and pseudoaneurysm formation has been described in numerous locations in patients with Moyamoya; they are felt to arise because of the increased hemodynamic stress applied to the frail collateral blood supply.7 In both the adult and pediatric population, the incidence of aneurysm formation in Moyamoya has been reported to be 3%–4%. In adults, they are more common, particularly in patients who present with SAH.6,7 The location of hemorrhage is a relevant clue in discovering the source of intracranial hemorrhage in Moyamoya, with rupture from lenticulostriate vessels, the circle of Willis vessels, and the choroidal arteries resulting in intracerebral, SAH, and intraventricular hemorrhage, respectively.
The rate of recurrent hemorrhage in untreated aneurysmal SAH in Moyamoya approaches 30%, and therefore definitive treatment is necessary to avoid increased morbidity and mortality in these already frequently compromised patients.9 Treatment options include both endovascular and surgical techniques. Endovascular approaches to the aneurysms include the use of glue and coils, depending on the size and location of the aneurysm; however, surgical intervention such as vascular bypass is often necessary if treatment of the aneurysm could result in obliteration of an important collateral vessel supplying the intracranial circulation. In this case, although endovascular placement of a coil mass within the spinal canal was not considered to be the ideal treatment, surgery was not considered, because of the patient’s highly compromised clinical condition. More important, cessation of recurrent episodes of SAH was considered a priority. In addition, the pseudoaneurysm was easily accessed and had a favorable configuration for endovascular treatment.
Beyond the presentation of a highly unusual pseudoaneurysm arising in a patient with unique extra- and intracranial vasculature, our case emphasizes the need to define these atypical collateral vascular pathways in patients with Moyamoya and intracranial hemorrhage without an identifiable source. Although SAH can be seen in these patients, the intracranial, spinal, and upper thoracic circulation must be evaluated to exclude an aneurysm or pseudoaneurysm and thus a potentially treatable source of bleeding. Rapid diagnosis and treatment of such lesions is imperative to avoid high rebleeding rates with the associated morbidity and mortality.
Footnotes
Presented at the 43rd annual meeting of the ASNR, Toronto, Ontario, Canada, May 21–27, 2005.
References
- Received July 18, 2005.
- Accepted after revision August 30, 2005.
- Copyright © American Society of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}