
Abstract
SUMMARY: We report the case of a child with multiple pituitary hormone deficiencies and a truncated pituitary stalk on MR imaging who had recovery of normal secretion of pituitary hormones in early adulthood. Follow-up MR imaging examination after recovery revealed marked enlargement of the proximal pituitary stalk. The case of our patient helps to explain the mechanism whereby some patients experience recovery of hormonal function.
Pituitary stalk interruption syndrome was first described in children with growth failure and pituitary hormone deficiencies after the advent of MR imaging.1,2 It is characterized by an absent, truncated, or thinned pituitary stalk, an ectopic posterior pituitary gland, and a hypoplastic or normal anterior pituitary gland. Patients with a thinned or truncated pituitary stalk predominantly have isolated growth hormone deficiency (IGHD), whereas those with an absent stalk generally have multiple pituitary hormone deficiencies (MPHD).3,4 Although recovery of hormonal production is not uncommon in patients with IGHD, it is rare with MPHD.5
Case Report
A 4¾-year-old boy was referred to Georgetown University Medical Center for evaluation of delayed growth and development. A growth chart showed him at the 50th percentile at birth and the fifth percentile at 9 months; thereafter, growth gradually fell to well below the third percentile. On examination, the boy had the height and appearance of an average 3-year-old child. A radiographic examination of the wrist indicated a bone age of between 3 and 3½ years.
Routine biochemical and hematologic determinations were within normal limits, as were results of thyroid function tests and baseline serum growth hormone levels. Insulinlike growth factor 1 (IGF-1) was below the sensitivity of the radioimmunoassay. Growth hormone deficiency was confirmed by appropriate stimulation tests.
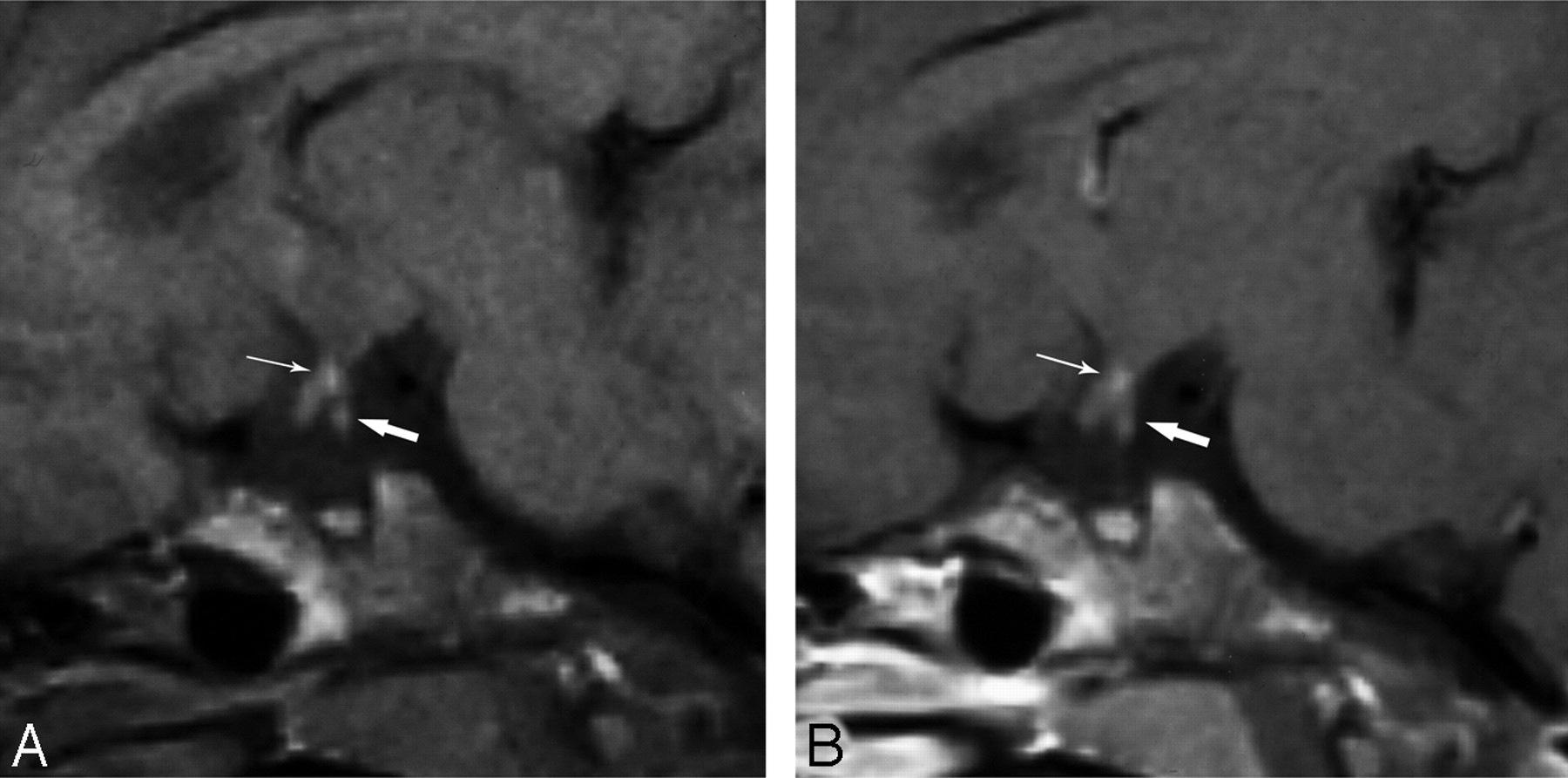
At the time of diagnosis, results on MR imaging revealed a small adenohypophysis and a truncated pituitary stalk. The proximal third of the stalk was slightly thickened, and the distal two thirds were very thin. A hyperintense signal intensity at the median eminence represented an ectopic posterior pituitary (Fig 1).
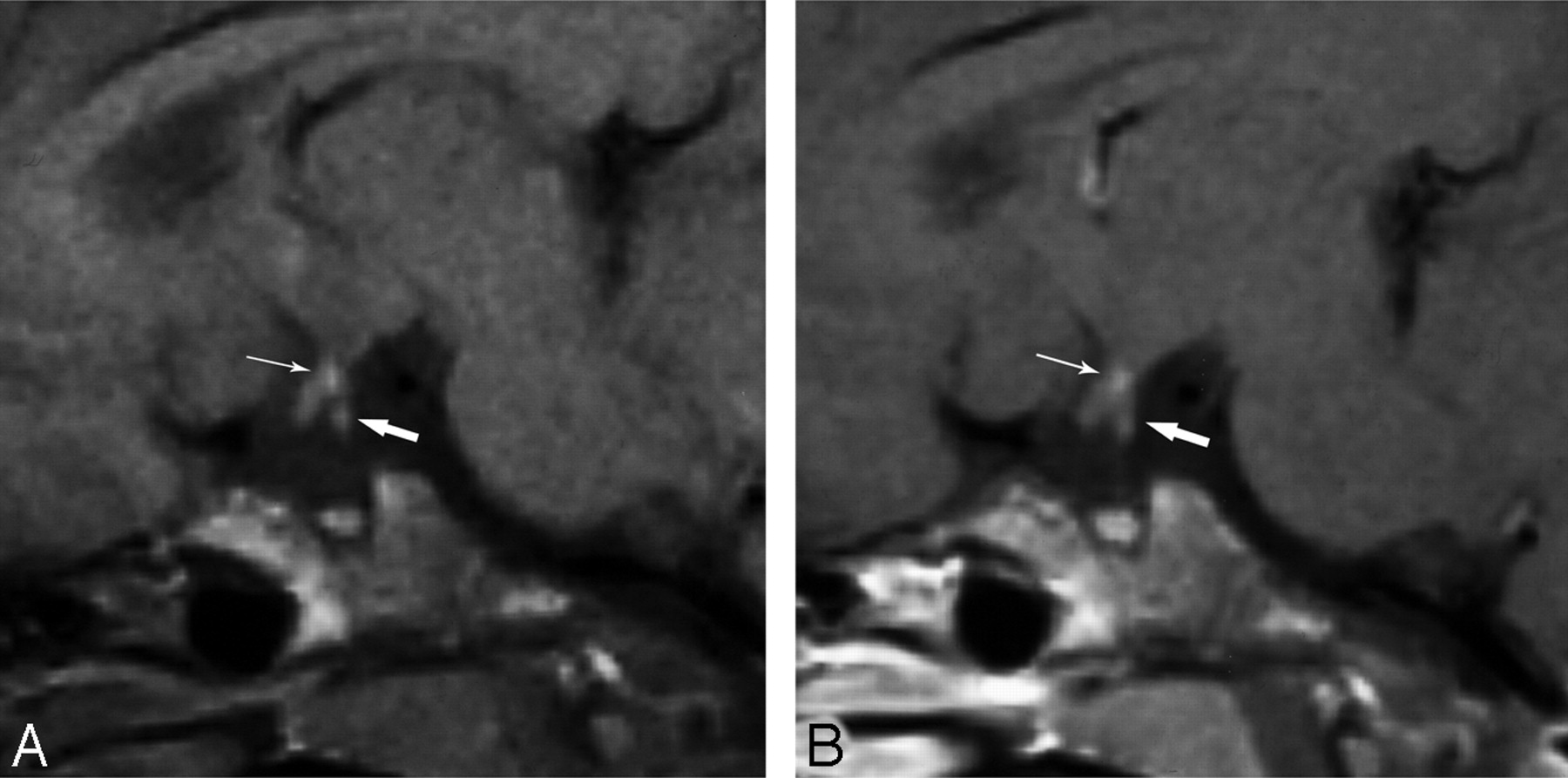
Sagittal unenhanced (A) and contrast-enhanced (B) T1-weighted (TR, 600 ms; TE, 15 ms) MR images in our patient at age 5 years show a slightly thickened proximal stalk (thick arrow) and a threadlike distal stalk. Ectopic posterior pituitary hyperintense signal intensity (thin arrow) is located at the median eminence. The adenohypophysis and sella turcica are small. The apparent lack of enhancement of the proximal stalk (B) is from a delay in imaging after the contrast injection. Coronal images (not shown), which were obtained before the sagittal images, demonstrated enhancement.
The patient received recombinant human growth hormone (hGH) replacement therapy with a dramatic response. At age 14 years, he was at the 25th percentile for height and the 10th percentile for weight. Results of routine laboratory tests and thyroid hormone, serum cortisol, and urinary free cortisol levels were normal. His serum testosterone and gonadotropins (follicle-stimulating hormone and leuteinizing hormone levels) were low in keeping with his prepubertal state. The bone age was 13 years. Results of a luteinizing hormone-releasing hormone (LHRH) test showed no response. The low testosterone and gonadotropin levels and lack of response to LHRH stimulation were considered evidence of gonadotropin deficiency. Depot-testosterone injections were added to the hGH replacement therapy. This treatment resulted in a growth spurt and additional pubertal development. At age 18 years, his height was 175.0 cm and he weighed 68.9 kg. In preparation for his attending college, his therapy was changed to AndroGel.
When he was seen at age 19 years, he had not had any hGH injections in the 4 months since starting college and had run out of AndroGel some weeks earlier. Despite not taking the prescribed medications, serum testosterone and IGF-1 levels were within normal limits. He remained off therapy until the end of the school year. When reevaluated 4 months later, all hormone levels were within normal limits, confirming recovery of endogenous hormone secretion. Repeat MR imaging examination revealed marked enlargement of the proximal pituitary stalk (Fig 2). The adenohypophysis remained small.
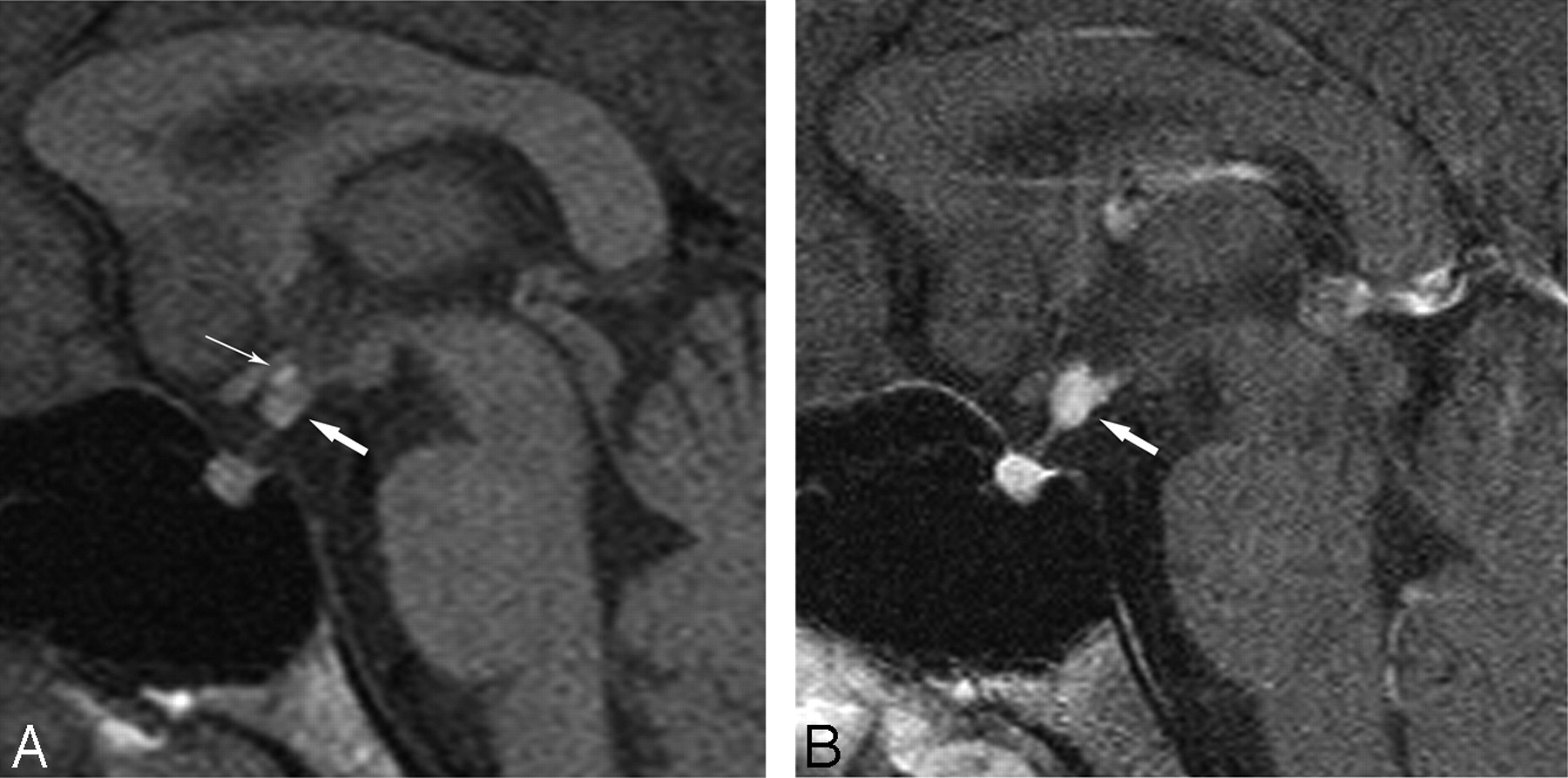
Sagittal unenhanced (A) and contrast-enhanced (B) T1-weighted (TR, 600 ms; TE, 15 ms) MR images in our patient at age 19 years show a markedly enlarged proximal stalk (thick arrow) and a thin distal stalk. Ectopic posterior pituitary hyperintense signal intensity (thin arrow) is seen at the median eminence on the unenhanced images but is obscured by contrast on the enhanced images. The adenohypophysis and sella turcica remain small.
Discussion
The morphologic features of the pituitary stalk on MR imaging have been found to correlate closely with the degree of hormone deficiency and rate of progression from IGHD in childhood to MPHD later in life. In 2 retrospective studies consisting of 69 children, most subjects with an absent pituitary stalk had MPHD, whereas most of the children with a truncated or thinned stalk had IGHD.3,4
Our patient was diagnosed with MPHD in childhood. At age 19 years, he unexpectedly had recovery of pituitary hormone secretion. This recovery coincided with a morphologic change in the proximal pituitary stalk on MR imaging. Unlike most patients with MPHD, our subject had partial preservation of the pituitary stalk. The stalk contains the hypothalamohypophyseal tract (the neural connection between the hypothalamus and posterior pituitary gland) and the hypophyseal portal system of blood vessels, which extend into the median eminence, surround the pituitary stalk, and supply the sinusoids of the adenohypophysis below. The hypophyseal portal system conveys the hypothalamic releasing factors that stimulate secretion of anterior pituitary hormones. Disruption of this system is considered the cause of hypopituitarism in patients with a thin or absent pituitary stalk.
A narrow sliver of adenohypophyseal tissue (pars tuberalis) extends upwards along the pituitary stalk. Although the pars distalis comprises the bulk of the adenohypophysis and is generally the source of hormone production, the pars tuberalis is known to occasionally be the site of hormone-producing pituitary adenomas.6 One might hypothesize that the marked enlargement of the proximal pituitary stalk in our patient represents growth of functioning adenohypophyseal tissue, rather than tumor. This “new” pituitary gland could be supplied by the hypophyseal portal system because it is above the level of the stalk disruption.
In conclusion, we present the case of a patient with spontaneous recovery from MPHD associated with development of a markedly enlarged proximal pituitary stalk. We hypothesize that the enlargement of the stalk might be because of growth of functioning adenohypophyseal tissue within the stalk.
- Received January 29, 2008.
- Accepted after revision February 5, 2008.
- Copyright © American Society of Neuroradiology
In this issue









{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.