
Abstract
BACKGROUND AND PURPOSE: Several trials have compared vertebral augmentation with nonsurgical treatment for vertebral compression fractures. This trial compares the efficacy and safety of balloon kyphoplasty and vertebroplasty.
MATERIALS AND METHODS: Patients with osteoporosis with 1–3 acute fractures (T5–L5) were randomized and treated with kyphoplasty (n = 191) or vertebroplasty (n = 190) and were not blinded to the treatment assignment. Twelve- and 24-month subsequent radiographic fracture incidence was the primary end point. Due to low enrollment and early withdrawals, the study was terminated with 404/1234 (32.7%) patients enrolled.
RESULTS: The average age of patients was 75.6 years (77.4% female). Mean procedure duration was longer for kyphoplasty (40.0 versus 31.8 minutes, P < .001). At 12 months, 7.8% fewer patients with kyphoplasty (50/140 versus 57/131) had subsequent radiographic fracture, and there were 8.6% fewer at 24 months (54/110 versus 64/111). The results were not statistically significant (P > .21). When we used time to event for new clinical fractures, kyphoplasty approached statistical significance in longer fracture-free survival (Wilcoxon, P = .0596). Similar pain and function improvements were observed. CT demonstrated lower cement extravasation for kyphoplasty (157/214 versus 164/201 levels treated, P = .047). For kyphoplasty versus vertebroplasty, common adverse events within 30 postoperative days were procedural pain (12/191, 9/190), back pain (14/191, 28/190), and new vertebral fractures (9/191, 17/190); similar 2-year occurrence of device-related cement embolism (1/191, 1/190), procedural pain (3/191, 3/190), back pain (2/191, 3/190), and new vertebral fracture (2/191, 2/190) was observed.
CONCLUSIONS: Kyphoplasty and vertebroplasty had similar long-term improvement in pain and disability with similar safety profiles and few device-related complications. Procedure duration was shorter with vertebroplasty. Kyphoplasty had fewer cement leakages and a trend toward longer fracture-free survival.
ABBREVIATIONS:
- AE
- adverse event
- BKP
- balloon kyphoplasty
- EQ-5D
- EuroQol-5-Domain
- KAVIAR
- Kyphoplasty and Vertebroplasty In the Augmentation and Restoration of vertebral body compression fractures
- MedDRA
- Medical Dictionary for Regulatory Activities
- ODI
- Oswestry Disability Index
- RCT
- randomized controlled trial
- VCF
- vertebral compression fracture
- VP
- vertebroplasty
Vertebral compression fractures (VCFs) are clinically recognized in 1.4 million individuals worldwide annually,1 often resulting in pain, disability, vertebral deformity,2 and considerable negative economic impact.3 Balloon kyphoplasty (BKP) and vertebroplasty (VP) are percutaneous procedures aimed at reducing pain and providing fracture stability. Balloon kyphoplasty uses orthopedic inflatable bone tamps before bone cement injection in an attempt to correct vertebral deformity and control cement distribution.4⇓–6 Vertebroplasty is similar, using needles to deliver bone cement without orthopedic balloons.7 When Kyphoplasty and Vertebroplasty In the Augmentation and Restoration of vertebral body compression fractures (KAVIAR) was initiated, no comparative randomized controlled trials (RCTs) existed, and evidence remains limited.8 Several RCTs demonstrated better clinical outcomes for kyphoplasty and vertebroplasty compared with nonsurgical management.4,7,9⇓–11 The KAVIAR study objectives were to document and compare BKP and VP safety and effectiveness in patients with osteoporosis with VCF. The primary end point, subsequent radiographic VCF incidence, was selected because stabilization and deformity correction may have an effect on new VCF occurrence.12 Secondary end points included pain, disability, and quality-of-life assessments.
Materials and Methods
Patients
A protocol steering committee, established before study enrollment (see the “Acknowledgments”), comprised kyphoplasty and vertebroplasty experts, to reduce the potential for bias and provide critical input to study design elements.
Participants had 1–3 acute, painful, VCFs from T5 to L5 due to osteoporosis and had correlative clinical findings with edema on MR imaging, uptake on radionuclide bone scans, or acute vertebral height loss within 6 months by CT, MR imaging, or x-ray. Patients were excluded if back pain was not attributable to VCF, they had >3 acute fractures, had VCFs >6 months old, had fractures due to cancer or high-energy trauma, required procedures other than BKP or VP for fracture stabilization, they had contraindications such as irreversible coagulopathy or known allergies to bone cement or contrast, or had evidence of local or systemic infection. In the absence of cancer or trauma (see exclusions above), the presence of VCF is a hallmark of osteoporosis13; therefore, the decision to perform diagnostic bone mineral attenuation examinations was determined by treating physicians and was not a study requirement. Before enrollment, participants gave written informed consent, which included risks for both procedures. The protocol and consent forms were approved by the institutional review board for enrolling sites.
Research Design
Patients were randomized to kyphoplasty (n = 199) or vertebroplasty (n = 205) by computer by using a dynamic minimization technique stratified by the number of prevalent VCFs, etiology, and study center; patients were not blinded—that is, on randomization, they were aware of the treatment assignment.
Investigator requirements were 50 lifetime procedures or 20 in the last year for each procedure. Investigators qualified for only 1 procedure could participate as a team—that is, they could partner with an investigator qualified in the other technique to treat patients randomized to the alternative treatment. Treating physicians partnering as a team were to consult on patient screening (before enrollment and randomization) to ensure agreement that the patient could be treated with either VP or BKP. Tools and polymethylmethacrylate bone cement used were approved or cleared by the FDA for treating VCFs by using BKP and VP, respectively. BKP was performed by using a bilateral approach as previously described (Kyphon Osteo Introducer Systems, Inflatable Bone Tamps, HV-R Bone Cement, Bone Filler Devices, and other BKP devices were manufactured by Medtronic Spine, Sunnyvale, California).4⇓–6,14 VP was performed according to local practices.
The primary end points were 12- and 24-month new radiographic VCF (including any new or worsening index fracture) incidence by using the method of Genant et al.15 Originally, the 1234 enrollment goal stemmed from an 8.7% difference in subsequent radiographic fracture (40% in VP, 31.3% in BKP), 20% withdrawal, 80% power, and 5% α. Due to high unanticipated withdrawal (38%) and limited enrollment, the sponsor, unaware of outcomes, terminated the study with only 404/1234 patients enrolled. This decision was discussed with the protocol steering committee and data safety monitoring board members (see the “Acknowledgments”) with subsequent investigator notification. Enrolled patients were terminated without additional follow-up except that any not reaching the 1-month visit were followed to collect 30-day safety data. Investigators reviewed and signed case report forms in an Electronic Data Capture system (Outcome, Cambridge, Massachusetts), and data were 100% source-verified.
All adverse events (AEs) were collected, reported, and evaluated by investigators for device and procedure relationship. AEs were systematically classified into preferred terms and system organ class according to the Medical Dictionary for Regulatory Activities (MedDRA)16 by using the verbatim language reported by investigators into Electronic Data Capture. An independent data safety monitoring board reviewed safety data and associated MedDRA coding for the trial. New clinical fractures were defined as subsequent, painful vertebral fractures coming to clinical attention. Data were derived from specific, subsequent fracture and adverse event data entered by sites in the Electronic Data Capture.
Secondary outcomes at 1, 3, 12, and 24 months included the SF-36 Physical Component Summary,17 the EuroQol-5-Domain (EQ-5D) questionnaire,18 a numeric rating scale for back pain,19 and the Oswestry Disability Index (ODI) (Section 8, regarding sexual activity, was removed from the ODI questionnaire and therefore not asked of these typically elderly patients).20 Back pain was also assessed 7 days postoperatively. For EQ-5D, US utilities were applied.21
Standing lateral spine radiographs were obtained at baseline, postoperatively, and at 3, 12, and 24 months. Standing lateral images were used for determining new radiographic fracture by using the method of Genant et al15; and vertebral kyphotic angulation, by using quantitative morphometry.22 The angle formed by lines drawn parallel to the caudal and cranial fractured vertebral body endplates determined the kyphotic angulation. A postprocedural CT scan was obtained through treated levels and was used for determining cement volume and leakage. All images were read centrally (Synarc, Newark, California) by a blinded radiologist. Cement volume was determined by cement injected intraoperatively as reported by investigators, and an independent radiologist used postoperative CTs and computer-assisted segmentation of vertebrae, with cement defined as voxels >850. Image segments were inspected, and voxels >850 were removed if clearly part of native bone.
Statistical Methods
Modified intention to treat was used, including all data available from the 381 patients randomized and treated. Eight patients with BKP and 15 with VP enrolled, withdrew before surgery, and were therefore not analyzed. All other subjects underwent surgery as assigned. Four patients with BKP and 7 with VP underwent a crossover surgery for a subsequent VCF. For any subject having surgery for a new VCF, the last observation before surgery was carried forward to later visits. Continuous variables were analyzed by ANCOVA by using the baseline as a covariate. For categoric variables, between-group comparisons were assessed by using the χ2 or Fisher exact test. For cement leakage, cement volume, and kyphotic angulation, analyses were based on treated levels. P ≤ .05 was statistically significant.
Funding Source
Medtronic Spine sponsored this study and contributed to study design, data monitoring, statistical analysis, and reporting of results and paid for independent core laboratory and data safety-monitoring board services.
Results
Patient Disposition and Demographics
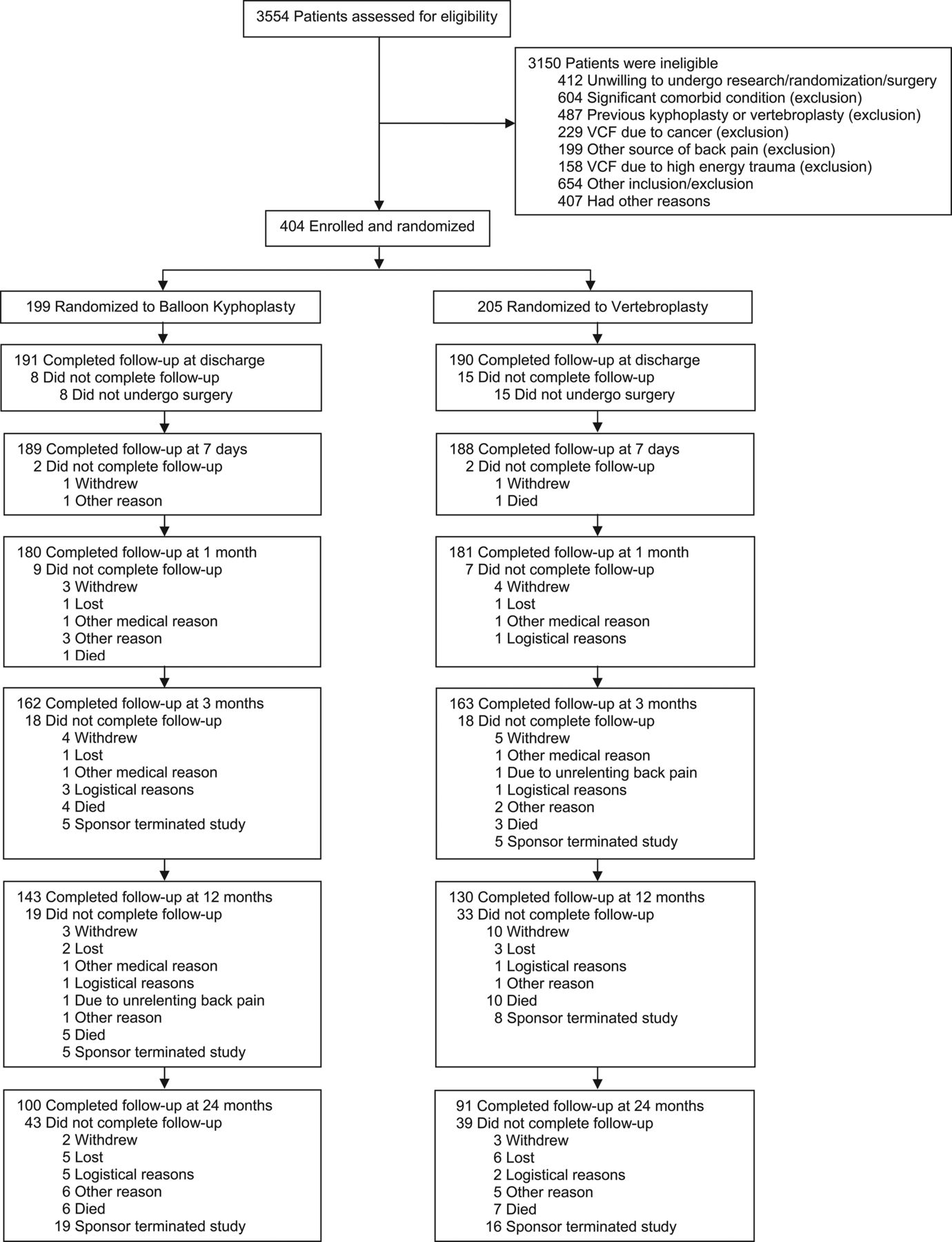
Patients were enrolled and randomized between October 2006 and May 2011. Figure 1 shows patient disposition.
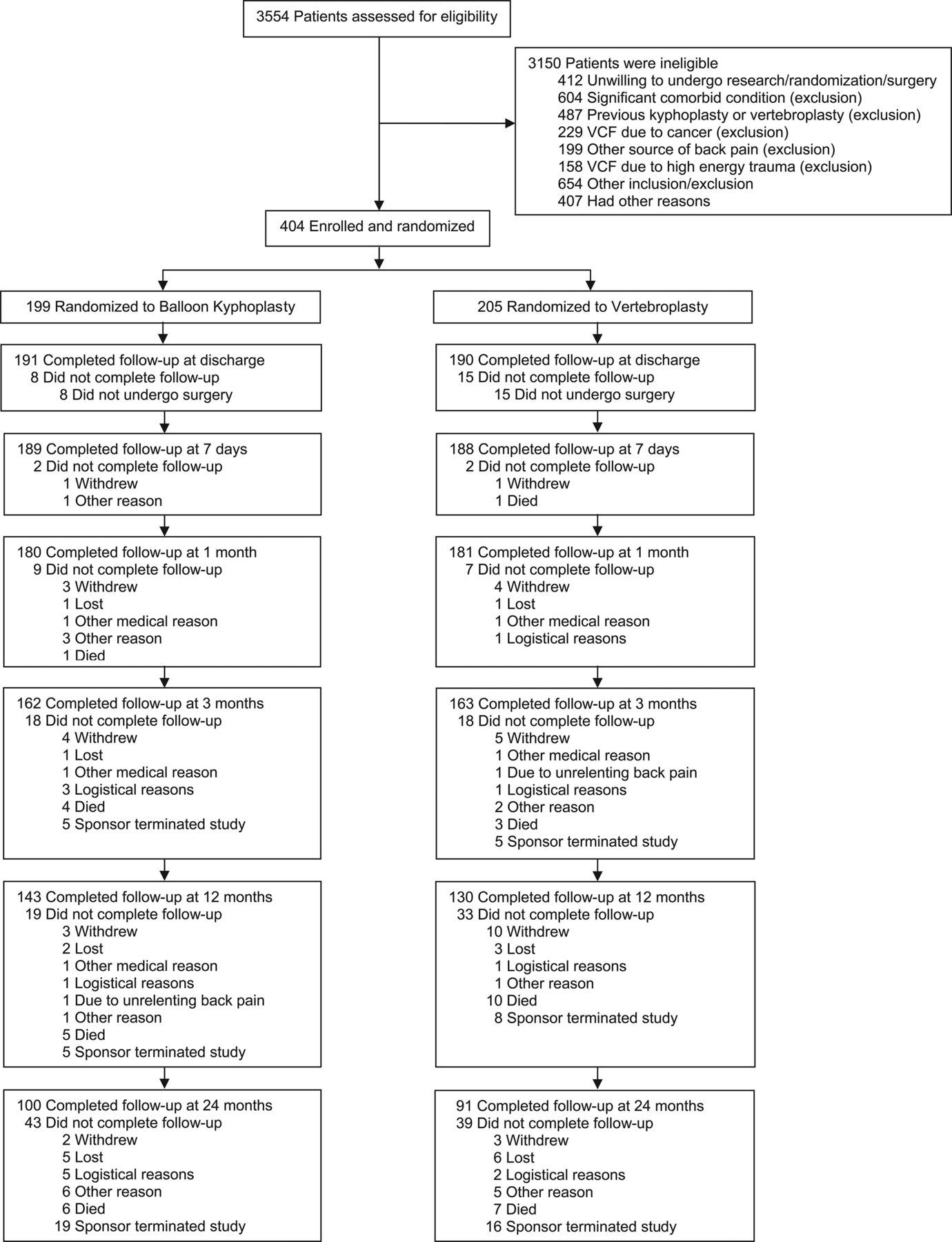
Patient accountability.
The average age of patients was 75.6 years, 77.4% were women, and 78.5% had single fractures treated (On-line Table). The baseline proportion of patients using bisphosphonates, calcium, and vitamin D is shown in the On-line Table; 151/261 (57.9%), 212/261 (81.2%), and 214/261 (82.0%) were using bisphosphonates, calcium, and vitamin D at 12 months respectively; and 93/191 (48.7%), 149/191 (78.0%), and 151/191 (79.1%), at 24 months. Use of these medications was not statistically significant between groups.
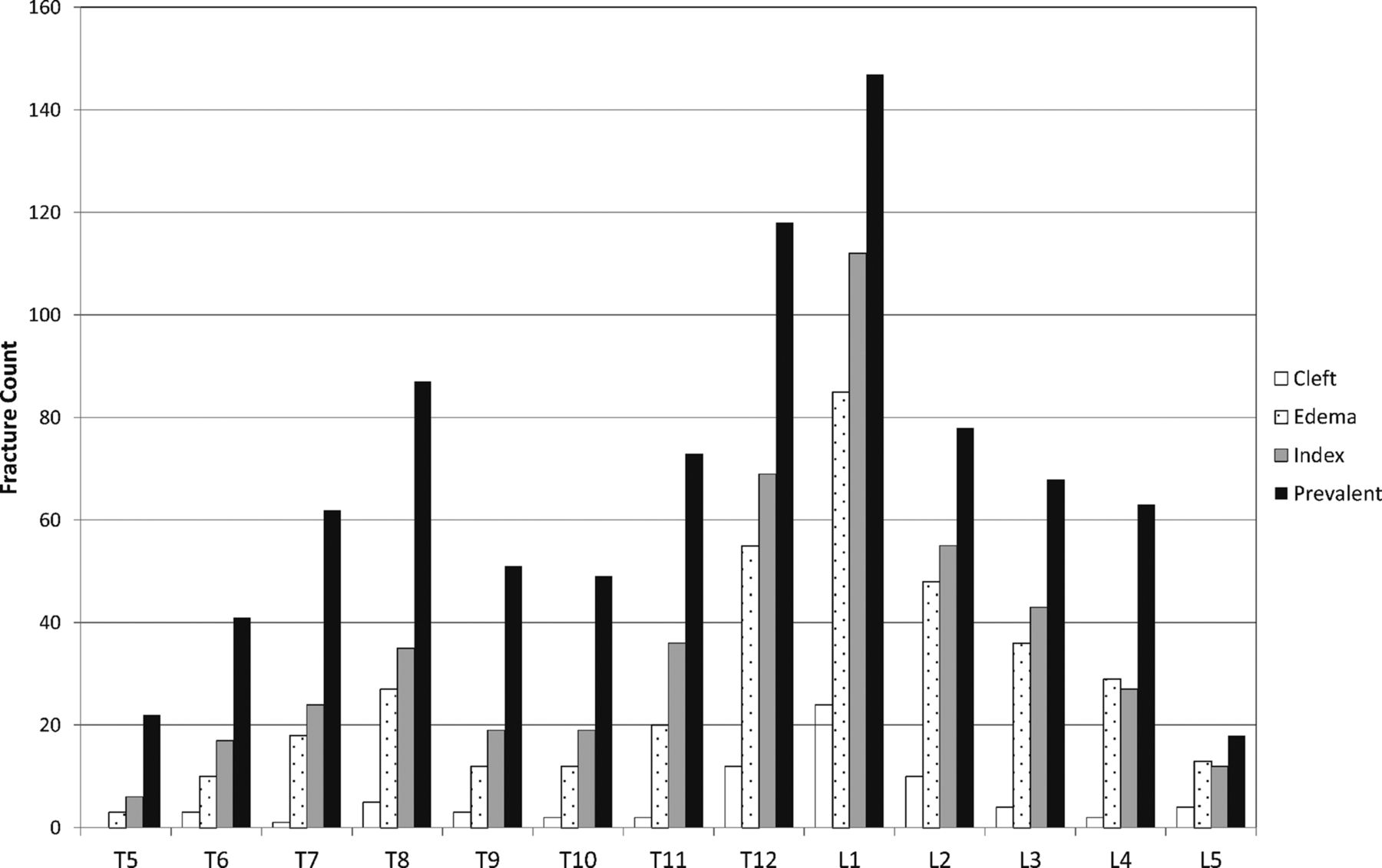
There was a higher radiographic fracture prevalence than identified clinically, and most treated fractures had active lesions confirmed on MR imaging (Fig 2). Most fractures occurred at T12 and L1.

Distribution of index and prevalent fractures and those with edema and vacuum cleft for the BKP and VP groups combined. Index levels (those identified as treatment levels) and prevalent fractures (all radiographic fractures assessed by the core laboratory) are shown, identified from standing lateral x-ray films with 379 of 381 treated patients contributing data. The distribution of levels with edema and those with vacuum cleft is shown on the basis of available MR imaging at baseline (294 of 381 treated patients).
Procedure Characteristics
Most patients (70.3%) had local anesthesia with conscious sedation (Table 1). Fewer radiologists performed kyphoplasty (150/191, 78.5%) compared with vertebroplasty (165/190, 86.8%). Vertebroplasty had a shorter mean procedure duration (BKP, 40.0 minutes; VP, 31.8 minutes; P < .001) and median hospitalization duration (BKP, 22 hours; VP, 8 hours; P = .010). For vertebroplasty, 152/189 (80.4%) procedures were performed by using an injector kit. Kyphoplasty had statistically significantly higher cement volumes assessed by CT (Table 1).
Procedure characteristics
Subsequent Vertebral Fracture
Regarding the primary end points (Table 2), 7.8% fewer patients with BKP had subsequent radiographic fractures compared with those who had VP at 12 months (P = .21), and 8.6% fewer, at 24 months (P = .23); but results were not statistically significant. Because subsequent radiographic fractures included any worsening index fractures, we analyzed those separately; 4 of 140 (2.9%) subjects with BKP and 10 of 131 (7.6%) subjects with VP had worsening index fractures (P = .10) at 12 months. No additional worsening index fractures were detected at 24 months.
Patients with new radiographic fracturesa
Kaplan-Meier analysis of new clinically identified fractures (Fig 3) approached statistical significance for longer fracture-free survival in the BKP group (Wilcoxon test, P = .0596). For the 88 subjects with new clinically recognized fractures (Fig 3), 85 of 88 (96.6%) were specifically associated with new-onset pain. Sixty-three (71.6%) subjects had a VCF confirmed by MR imaging; 15 (17.0%) had VCF confirmed by using x-ray only, which consisted of a change of at least 1 Genant grade. Six (6.8%) had CT, 2 (2.2%) had bone scans, and 2 (2.2%) had an imaging technique not specified. With regard to subsequent treatment, 70 (79.5%) had vertebral augmentation for at least 1 VCF, 16 (18.1%) had nonsurgical care alone, 1 (1.1%) had subsequent fusion surgery with instrumentation, and 1 (1.1%) had therapy not identified.

Kaplan-Meier survival analysis for new clinical fractures.
Pain, Disability, and Quality of Life
Kyphoplasty and vertebroplasty groups had similar baseline back pain, SF-36 Physical Component Summary, and EQ-5D quality-of-life and ODI scores. For each outcome, statistically significant improvements from baseline were observed for each group, but differences between treatment groups were not significant (Fig 4). Concomitant with pain relief, use of opioid medications dropped from 73.9% (122/165) of patients at baseline (On-line Table) to 17.6% (25/142) for BKP and from 74.6% (126/169) to 23.9% (34/142) for VP at 6 months (P = .24). Results were 17.6% (16/91) for BKP and 25.6% (21/82) for VP at 24 months (P = .26).

Quality-of-life, disability, and pain assessments at baseline and after balloon kyphoplasty or vertebroplasty. Means and 95% confidence intervals are shown for balloon kyphoplasty (solid lines) and vertebroplasty (dashed lines) for the SF-36 Physical Component Summary (scale 0–100) (A); the total EQ-5D scores (scale 0–1) (B); back pain (scale 0–10) (C); and the Oswestry Disability Index (scale 0–100) (D). The treatment P value in each panel indicates the comparison between groups. Below each panel, the n for each group is shown for baseline, 3, 12, and 24 months and the group average for change from baseline and 95% CI for 3, 12, and 24 months. The asterisk indicates P < .001 for all change from baseline scores.
Secondary Radiographic End Points
Investigators were to attempt vertebral deformity correction, regardless of treatment; 154/191 (80.6%) patients with BKP and 142/189 (75.1%) with VP had perioperative postural reduction. Compared with the preoperative condition, average postoperative kyphotic correction was statistically significant at each time point for both the BKP and VP groups (Table 3). Postoperatively, the ANCOVA estimate of mean difference between groups was 0.21° (95% CI, −0.73°–1.14°) and was not statistically different (P = .663). At 24 months, kyphosis correction was better in the BKP group with a mean difference between groups of 1.42° (95% CI, 0.10°–2.74°), which was statistically significant (P = .036).
Index vertebral body kyphotic angulation correction
Safety
The most common AEs (classified according to MedDRA) within 30 days of surgery were procedural pain (BKP: 12/191, VP: 9/190), back pain (BKP: 14/191, VP: 28/190), and new symptomatic fracture (BKP: 9/191, VP: 17/190). Common during 2 years were bronchitis (BKP: 10/191, VP: 10/190), pneumonia (BKP: 15/191, VP: 12/190), urinary tract infection (BKP: 11/191, VP: 19/190), falls (BKP: 47/191, VP: 46/190), procedural pain (BKP: 12/191, VP: 9/190), arthralgia (BKP: 18/191, VP: 12/190), back pain (BKP: 49/191, VP: 59/190), lumbar vertebral facture (BKP: 9/191, VP: 13/190), and thoracic vertebral fracture (BKP: 20/191, VP: 21/190). Device- and procedure-related AEs during 2 years are detailed in Table 4; most were observed within 30 days postsurgery. All AEs are posted on www.clinicaltrials.gov (NCT00323609). A few AEs, including procedural pain (BKP: 3/191, VP: 3/190), back pain (BKP: 2/191, VP: 3/190), new fractures (BKP: 2/191, VP: 2/190), cement embolism (BKP: 1/191, VP: 1/190), muscle spasm (BKP: 1/191, VP: 0/190), arthralgia (BKP: 1/191, VP: 0/190), bone marrow edema (BKP: 0/191, VP: 1/190), and implant-site extravasation (BKP: 0/191, VP: 1/190), were specifically considered to be device-related (Table 4). Five BKP AEs (constipation, procedural nausea, procedural hypotension, hallucination, exacerbated chronic obstructive pulmonary disease) and 5 VP AEs (hypersensitivity, mental status changes, hypoxia, respiratory failure, hematoma) were considered anesthesia- or procedure-related (Table 4). No deaths were noted as device- or procedure-related.
Device/procedure/anesthesia–related adverse events during 2 years
Overall cement extravasation, assessed by postoperative CT (Fig 5), was lower (P = .047) for BKP (157/214 levels treated) compared with VP (164/201 levels treated). There was lower intravascular extravasation for BKP (59/214 levels treated) compared with VP (76/201 levels treated, P = .028). As indicated in Table 4, 1 patient with BKP and 1 with VP each presented with symptoms and were found to have cement embolism. One patient with VP had a new symptomatic fracture occur within 2 days postoperatively (inferior to the index level), with inferior cement leakage that was considered possibly bone cement–related.

Cement extravasation. The percentage of treated vertebrae in each treatment group having cement extravasation, measured by using postoperative CT, is shown; results are based on evaluable CT data for 168/191 patients with BKP and 160/190 with VP, accounting for 214/244 and 201/233 levels, respectively. Fischer exact P values comparing the 2 treatment groups for each category are shown.
Discussion
This was the first large-scale RCT of BKP and VP with long-term follow-up. Both treatments provided similar sustained improvement from baseline in pain, disability, and quality of life that lasted for 2 years. These improvements were statistically significant and clinically relevant but were not statistically different between groups. Safety data support the safe use of both BKP and VP. Kyphoplasty trended toward fewer fractures, had lower cement extravasation, and more kyphotic deformity correction at 24 months. With vertebroplasty, there was slightly more local anesthesia use, more outpatient procedures, and a shorter duration of stay; it is likely that these findings are due to the different physician profiles performing the procedures (Table 1) and associated practice patterns.23,24 Differences in physician profile likely stem from the study design allowing investigators to participate as a team (see Material and Methods). Shorter procedure and fluoroscopy duration for VP may be related to more unipedicular vertebral access during VP treatment (Table 1).
Minimally clinically important differences are commonly used thresholds to estimate the clinical significance of outcomes.25 Improvements from baseline in the SF-36 Physical Component Summary were >7.5 points at 12 and 24 months for both groups, exceeding the estimated minimally clinically important difference of 3.5–4.3 points.25 Similarly, improvements of ≥4 points exceeded the 1- to 2.5-point threshold for back pain,19,25 improvements of >25 points exceeded the 10- to 15-point threshold for ODI,20,25 and improvements of ≥0.28 points exceeded the 0.08 threshold for EQ-5D.26
Cumulative evidence demonstrates that kyphoplasty and vertebroplasty provide better outcome than nonsurgical management in RCTs and meta-analyses4,5,7,9⇓–11,27,28 and acceptable cost-effectiveness ratios.11,29⇓–31 Several large retrospective studies using claims data, investigating BKP, VP, and nonsurgical management, provide additional evidence.32⇓⇓–35 Although 2 blinded RCTs concluded that vertebroplasty was similar to a local anesthetic “sham” intervention,36,37 these trials have several important limitations, including atypically broad inclusion criteria, allowance of chronic fractures, small sample size, and, in 1 study, high crossover, all of which preclude definitive conclusions.28,38,39 For example, in 1 study, higher crossover in the sham group compared with vertebroplasty (51% versus 13%, P < .001) at 3 months suggests that any short-term effects of the sham intervention are not long-lasting.36 Here, and in several other RCTs, kyphoplasty and vertebroplasty had statistically significant and sustained clinical improvement from baseline in pain, disability, and quality-of-life outcomes for 1 and 2 years; and compared with nonsurgical management, benefits persisted throughout 1 and 2 years for several outcomes.7,9⇓–11 Such results are inconsistent with placebo effects.
Currently, there is 1 small randomized study showing similar pain outcomes for BKP and VP but statistically significantly better height restoration for BKP.8 Nonrandomized comparisons show similar results.40,41 Here, postsurgery kyphotic angulation correction was similar between groups. There was some loss of correction in both groups at 3 months; however, for VP, the trend was more loss, with a statistically significant 24-month difference between groups (Table 3). Our postoperative results of approximately 3° of kyphosis correction are consistent with 2 other BKP RCTs5,6; one with long-term follow-up reported minimal correction loss during 2 years.5 Postural reduction has been shown to provide deformity correction for vertebroplasty,42,43 achievable in 35%–50% of acute fractures that have dynamic mobility.6,43 Likewise, in several BKP studies, substantial postural reduction with additional inflatable bone tamp contributions of 27%–100% has been documented.6,44,45 With KAVIAR, 75% of patients with VP had postural reduction, accounting for deformity correction in the VP group, and this finding may explain less postoperative correction in VP (compared to BKP) reported in other studies.8,40,41
The subsequent radiographic fracture rate is similar to that in another RCT5,10 and is likely due to the high number of prevalent fractures at baseline, a potent risk factor.13 This finding underscores the importance of additional therapeutic measures such as pharmacologics to help reduce fracture risk. Because randomization was stratified by baseline fracture prevalence, BKP and VP groups were well-balanced. Although not statistically significant, likely due to lack of statistical power, the BKP group was 7.8%–8.6% lower in 1- and 2-year radiographic fracture rates, consistent with the prespecified protocol originally powered to detect an 8.7% difference. Furthermore, the Kaplan-Meier analysis of new clinically recognized fractures approached statistical significance for a longer time to first clinical fracture within the BKP group. These results are consistent with several meta-analyses showing fewer new VCFs in BKP.46⇓–48
Kyphoplasty and vertebroplasty were found to be safe in this population, having similar safety profiles (Table 4). A similar number of patients in each group had device-related cement embolism (1 BKP, 1 VP), back pain (2 BKPs, 3 VPs), procedural pain (2 BKPs, 3 VPs), and new fractures considered to be related to the procedure (2 BKPs, 2 VPs). Several meta-analyses suggested that while both procedures have a low complication rate, BKP may have a lower rate of serious and symptomatic complications.47⇓–49 The similar safety profile observed here may be due to highly experienced physicians required by the protocol.
CT assessment showed significantly less cement extravasation in BKP- (73%) versus VP-treated (82%) vertebrae (P = .047). These rates are higher than those in most reports, likely relating to use of CT, but are consistent with leakage being lower in BKP.46⇓⇓–49 Most other studies reported cement leakage on the basis of investigator assessment, by using reviews of conventional x-ray images, which are prone to interpretation bias and are less sensitive. These results are similar to those in another study using CT, also reporting less leakage in BKP (49%) versus VP (87%).50 Leakage into the perispinal vasculature was significantly less (P = .028) for BKP. Meta-analyses of complications suggest that BKP results in fewer symptomatic cement leakages, which include embolism and spinal cord compression.46⇓–48
The primary limitations in this study were the lack of patient blinding, substantial loss to follow-up, and early termination, which resulted in lack of statistical power for the primary end point. Vertebroplasty treatment was not standardized among centers. This lack of standardization may be viewed as a limitation and likely accounts for observed differences between groups in bilateral treatment and may, at least partially, account for differences in cement volumes and leakage. Differences in bilateral treatment, in turn, may have had an effect on the statistically significant changes between groups in kyphotic angulation at 24 months. However, because there is no established standard for vertebroplasty, for generalizability, every study center was asked to provide care consistent with local practices. Nonetheless, the strengths are the randomized, multicenter design, a relatively large sample size, and long-term follow-up. The results of this trial confirm the effectiveness of vertebral body cement augmentation for patients with osteoporosis with ongoing pain at index levels correlated by physical examination and imaging. Our results are consistent with recently updated guidelines published by the National Institute for Health and Care Excellence in the United Kingdom.51
Conclusions
Kyphoplasty and vertebroplasty had similar statistically significant sustained clinical improvement in pain and disability with similar AE profiles. Procedure duration and hospitalization were shorter with vertebroplasty. Kyphoplasty had fewer cement leakages, a trend of longer fracture-free survival, and less loss of kyphotic-deformity correction during 2 years.
Acknowledgments
The authors are indebted to all participating staff at the investigational centers and the patients who consented to participate in the KAVIAR trial, and they thank Li Ni, PhD, and Feng Tang, PhD, (Medtronic Spine) for contributions to statistical analysis. The authors gratefully acknowledge the KAVIAR protocol steering committee members, Drs Jacques Dion, Michael Ford, Joshua Hirsch, Mary Jensen, Reginald Knight, Isador Lieberman, James Lindley, Mark Myers, Wayne Olan, Frank Phillips, and Gregg Zoarski for contributions to the study design and the data safety monitoring board members, Drs Gunnar Andersson, Harry Cloft, Deborah Kado, Kern Singh, and Joel Verter, for contributions in monitoring patient safety throughout the trial.
Appendix
KAVIAR Investigators
Principal investigator, city, state (number of patients enrolled), for enrolling centers:
United States.
G. Fueredi, Burlington, Wisconsin (42); G. So, Torrance, California (39); M. Dohm, Grand Junction, Colorado (36); L. Haikal, Huntington, West Virginia (28); C. Black, Provo, Utah (26); J. Milburn, New Orleans, Louisiana (22); R. DiSalle, Toledo, Ohio (21); A. Dacre, Billings, Montana (20); J. Neil, Scottsdale, Arizona (19); N. Cooper, Atlanta, Georgia (19); P. Chesis, Kansas City, Missouri (17); D. Sacks, Reading, Pennsylvania (17); S. Pledger, Middletown, Ohio (17); J. Small, Temple Terrace, Florida (16); P. Minor, Milwaukee, Wisconsin (12); H. Haykal, Houston, Texas (9); M. Montgomery, Temple, Texas (5); C. Kazmierczak, Royal Oak, Michigan (5); S. Bukata, Rochester, New York (4); A. Padidar, San Jose, California (4); P. Schloesser, Murray, Utah (4); B. Ward, Bend, Oregon (3); V. Lewis, Roanoke, Virginia (3); D. Beall, Oklahoma City, Oklahoma (3); C. Graham, Columbia, South Carolina (1).
Canada.
C. Guest, Barrie, Ontario (12).
Footnotes
Disclosures: Michael Dohm—RELATED: Fees for Participation in Review Activities such as Data Monitoring Boards, Statistical Analysis, Endpoint Committees, and the Like: Medtronic Spine,* Comments: The Western Slope Study Group was compensated for study-specific data collection related to this study only. I received no money because the Western Slope Study Group is a quality-improvement organization, 501 (c) 3, and I am not a paid employee. I received no compensation at any time, in any form from Medtronic. Carl M. Black—RELATED: Grant: Kyphon/Medtronic,* Comments: Utah Valley Regional Medical Center received remuneration for administrative support during the research trial; Support for Travel to Meetings for the Study or Other Purposes: Kyphon/Medtronic, Comments: for inservice and training on research protocol; Provision of Writing Assistance, Medicines, Equipment, or Administrative Support: Kyphon/Medtronic*, Comments: data collection and statistical support; Other: As a study investigator, my institution received compensation from Medtronic Spine for study-specific data collection. Alan Dacre—RELATED: Provision of Writing Assistance, Medicines, Equipment, or Administrative Support: Kyphon/Medtronic,* Comments: to support the collection of data for the study; Other: As a study investigator, my institution received compensation from Medtronic Spine for study-specific data collection; UNRELATED: Consultancy: Medtronic, Comments: I have an agreement but have not done any remunerable work. John B. Tillman—RELATED: Other: Medtronic, Comments: employed as a Clinical Program Director; UNRELATED: Stock/Stock Options: Medtronic. George Fueredi—RELATED: Grant: Aurora Medical Group*; Other: As a study investigator, my institution received compensation from Medtronic Spine for study-specific data collection and has received compensation for consulting for Medtronic Spine. *Money paid to the institution.
This work was sponsored and funded by Medtronic Spine.
Indicates open access to non-subscribers at www.ajnr.org
References
- Received June 15, 2014.
- Accepted after revision August 25, 2014.
- © 2014 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Outcomes and Safety Comparison of Vertebroplasty, Balloon Kyphoplasty, and Vertebral Implant for Treatment of Vertebral Compression Fractures
- Review of Vertebral Augmentation: An Updated Meta-analysis of the Effectiveness
- Vertebroplasty and Kyphoplasty for Osteoporotic Vertebral Fractures: What Are the Latest Data?
- Response to: Randomized controlled trial of vertebroplasty versus kyphoplasty in the treatment of vertebral compression fractures
- Randomized controlled trial of vertebroplasty versus kyphoplasty in the treatment of vertebral compression fractures
- Randomized controlled trial of vertebroplasty versus kyphoplasty in the treatment of vertebral compression fractures
- Outcomes of vertebroplasty compared with kyphoplasty: a systematic review and meta-analysis
- Anterior spinal fixation for recollapse of cemented vertebrae after percutaneous vertebroplasty