
Abstract
BACKGROUND AND PURPOSE: Accurate localization of the foot/leg motor homunculus is essential because iatrogenic damage can render a patient wheelchair- or bed-bound. We hypothesized the following: 1) Readers would identify the foot motor homunculus <100% of the time on routine MR imaging, 2) neuroradiologists would perform better than nonradiologists, and 3) those with fMRI experience would perform better than those without it.
MATERIALS AND METHODS: Thirty-five attending-level raters (24 neuroradiologists, 11 nonradiologists) evaluated 14 brain tumors involving the frontoparietal convexity. Raters were asked to identify the location of the foot motor homunculus and determine whether the tumor involved the foot motor area and/or motor cortex by using anatomic MR imaging. Results were compared on the basis of prior fMRI experience and medical specialty by using Mann-Whitney U test statistics.
RESULTS: No rater was 100% correct. Raters correctly identified whether the tumor was in the foot motor cortex 77% of the time. Raters with fMRI experience were significantly better than raters without experience at foot motor fMRI centroid predictions (13 ± 6 mm versus 20 ± 13 mm from the foot motor cortex center, P = 2 × 10−6) and arrow placement in the motor gyrus (67% versus 47%, P = 7 × 10−5). Neuroradiologists were significantly better than nonradiologists at foot motor fMRI centroid predictions (15 ± 8 mm versus 20 ± 14 mm, P = .005) and arrow placement in the motor gyrus (61% versus 46%, P = .008).
CONCLUSIONS: The inability of experienced readers to consistently identify the location of the foot motor homunculus on routine MR imaging argues for using fMRI in the preoperative setting. Experience with fMRI leads to improved accuracy in identifying anatomic structures, even on routine MR imaging.
Localization of the precentral (motor) gyrus by using functional MR imaging before neurosurgical resection of brain tumors has gained acceptance clinically and is a routine procedure.1⇓–3 Two motor areas commonly mapped by using fMRI are the hand and face.4 The localization of these areas by fMRI is often validated intraoperatively by using direct cortical stimulation.2,3,5 However, localization of the foot motor homunculus in the preoperative setting in patients with brain tumor is uniquely important. First, iatrogenic damage to the foot motor homunculus and the resultant paresis of the leg can render a patient wheelchair- or bed-bound, conditions that may be more debilitating than paresis of the nondominant hand or arm. By contrast, iatrogenic compromise of the face and tongue homunculus is often compensated for by corticobulbar fibers from the contralateral hemisphere. Second, the localization of the foot motor homunculus lacks a discernible anatomic landmark such as the “reverse Ω sign” for the hand motor area.6 Anatomic localization is also rendered more difficult because the central sulcus often does not reach the hemispheric fissure.4,7 Third, the foot motor homunculus is tucked under the sagittal sinus along the interhemispheric fissure, making its localization difficult to confirm by intraoperative direct cortical stimulation.8,9 Last, there is no sulcus between the foot motor homunculus and the supplementary motor area, making distinction of the foot motor area from the supplementary motor area more difficult on routine MR imaging.4,10
Due to the importance of foot motor function preservation and the difficulties with identifying the foot motor homunculus on routine MR images, we aimed to assess the utility of fMRI of the foot in the preoperative setting. To test the utility of obtaining fMRI in cases in which the brain tumor involved the medial aspect of the high frontoparietal convexity, we asked a group of clinicians to identify the foot motor homunculus on preoperative anatomic (non-fMRI) MR images. These results were compared with those of the fMRI study performed simultaneously, to which the respondents were blinded. We hypothesized the following: 1) The respondents would identify the foot motor homunculus <100% of the time, 2) neuroradiologists would perform better than nonradiologists, and 3) those with fMRI experience would perform better than those without fMRI experience.
Materials and Methods
This study was approved by the institutional review board. The raters reviewed MR imaging data acquired previously; therefore, obtaining informed consent was waived by the institutional review board.
Rater Groups
Thirty-five raters, all at the attending level, were recruited for this study and included 24 neuroradiologists (attending-level experience, 1–27 years; mean, 9 years) and 11 nonradiologists (attending-level experience, 1–26 years; mean, 10 years). Each nonradiologist was board-certified, with most of their practices devoted to patients with brain tumors. All radiologists were board-certified. Each rater was given a PowerPoint file (Microsoft, Bothell, Washington) with a questionnaire asking the rater to identify their specialty, length of practice at the attending level, and number of fMRI cases viewed per month (never, ≤1, 2–5, or ≥6). The file consisted of 14 consecutive patients with brain tumors involving the high frontoparietal convexity. Each case was represented by 6 contiguous axial MR imaging sections from the most relevant diagnostic series. The patients included 5 men and 9 women (26–66 years of age; mean age, 53 years) (Table 1). The pathology of the tumors was determined through histologic evaluation of surgical biopsies. For each case, the raters were to perform or respond to the following:
Please move the “arrow” sign to indicate your estimate of the foot motor region location on the side of pathology. (The tip of the arrow sign should be in the center of the foot motor area.)
Does the tumor involve the foot motor area? (Yes/No)
Does the tumor involve the motor cortex? (Yes/No)
Summary of patient characteristics
Additional instructions were provided regarding the definition of the anatomic borders of the tumor:
On gadolinium-enhanced images, tumor is defined as enhancing lesions; the surrounding T1 hypointensity representing edema is not considered tumor for the purpose of this study.
On the FLAIR sequence, tumor is defined as FLAIR signal abnormality.
For case 4 (T2), tumor is defined as the discrete lesion with rim hypointensity; the surrounding T2 hyperintensity representing edema is not considered tumor for the purpose of this study.
Returned responses were anonymized so that each rater was identified by his or her specialty and a number only.
MR Imaging Data Acquisition
All images were acquired with either a 3T or 1.5T Signa LX scanner (GE Healthcare, Milwaukee, Wisconsin) with an 8-channel head coil. For fMRI data acquisition, we used the following imaging sequence: gradient-echo echo-planar (TR, 4000 ms; TE, 30 ms [for 3T] and 40 ms [for 1.5T]; matrix, 128 × 128; flip angle, 90°; 4.5-mm section thickness with no gap; FOV, 240-mm; 32–36 axial sections covering whole brain). T1-weighted spin-echo (TR/TE, 600/8 ms; matrix, 256 × 256; flip angle, 90°; 4.5-mm section thickness with no gap; FOV, 240 mm up to 36 sections) and axial FLAIR images (TR/TE/TI, 9000/125/2250 ms; matrix, 512 × 512; flip angle, 90°; 4.5-mm section thickness with no gap; FOV, 240 mm; up to 36 axial sections) were obtained in the same axial orientation as the fMRI data. 3D T1-weighted anatomic images were also acquired with a spoiled gradient-recalled sequence (TR/TE, 22/4 ms; matrix, 256 × 256 matrix; flip angle, 30°; 1.5-mm thickness; FOV, 240 mm). Head motion was minimized in a standard head coil by using straps and foam padding. Gadopentetate dimeglumine (Magnevist; Bayer HealthCare Pharmaceuticals, Wayne, New Jersey) was injected through a peripheral angiocatheter (18–21 ga) at a standard dose (0.2 mL/kg body weight; maximum, 20 mL).
fMRI Paradigm and Task
We used a block motor paradigm (20 seconds for the task period and 40 seconds for rest) in which each patient performed self-paced toe movement on both feet while avoiding ankle and leg motion in response to an aural cue. The task consisted of 90 images for 6 cycles. The patient's compliance with fMRI paradigms, functional brain activity, and head motion were monitored in real-time by using available software (Brainwave; Medical Numerics, Germantown, Maryland).
fMRI Data Analysis
Image processing and analysis were performed by using Analysis of Functional Neuro Images (http://afni.nimh.nih.gov). Head-motion correction was performed by using 3D rigid-body registration. Spatial smoothing (Gaussian filter with 4-mm full width at half maximum) was applied to improve the signal-to-noise ratio. Functional activity was generated by using cross-correlation analysis. Signal changes with time were correlated with a mathematic model of the hemodynamic response to neural activation. To reduce false-positive activity from large venous structures or head motion, we set to zero the voxels in which the SD of the acquired time-series exceeded 8% of the mean signal intensity. A board-certified neuroradiologist read each case for foot motor area and tumor localization.
Scoring Method and Statistical Analysis
For question 1, we measured the distance from the arrow placement to the centroid of fMRI activation in the foot motor area (defined as the 10 most statistically activated pixels) and recorded whether the arrow was in the motor gyrus binarily (on the basis of the fMRI data). Distance measurements were made by using the PACS Web system. Rater responses and patient fMRI reports for arrow and foot activation centers were made for placement on corresponding images in the PACS Web system. Intrinsic rulers were used for the measurements. For questions 2 and 3, responses were scored as correct/incorrect on the basis of the fMRI data. The ground truth locations of the foot motor homunculi were defined as the centroid of fMRI foot motor activation. Scores and distances were recorded for each rater and case, and summary statistics were calculated and compared by using the Mann-Whitney U test. Statistical significance was defined as P = .05. Comparisons were made across rater groups according to fMRI usage and specialty.
Results
All Rater Results
No single rater scored 100% correct for the criteria used in this study. The average arrow placement was 17 ± 11 mm from the centroid of foot motor fMRI activation; 57% of the raters correctly placed the arrow in the motor gyrus. Raters correctly identified whether the tumor was in the foot motor cortex 77% of the time and whether the tumor was in the motor gyrus 71% of the time.
Distance Measurements
fMRI Experience.
Raters were split into 2 groups: those without fMRI experience (18 raters; 11 neuroradiologists, 7 nonradiologists) and those with fMRI experience (17 raters; 13 neuroradiologists, 4 nonradiologists) (Table 2). If we considered all cases, the group with fMRI experience was significantly closer to the foot motor cortex center with their arrow placements than the group without fMRI experience (13 ± 6 mm versus 20 ± 13 mm, P = 2 × 10−6).
Rater comparisons: no versus any fMRI experiencea
Experience Gradient.
Raters were categorized on the basis of fMRI experience along a gradient into 3 groups: no experience (18 raters), ≤1 per month (14 raters; 10 neuroradiologists, 4 nonradiologists), and 2–5 per month (3 raters; 3 neuroradiologists) (Table 3). Both the ≤1 per month (13 ± 6 mm from the foot motor cortex center) and 2–5 per month (12 ± 7 mm) rater groups scored significantly better than those without experience (P = 2 × 10−6 and P = 2 × 10−5, respectively). The groups with experience did not differ significantly (P = .204).
Rater comparisons by fMRI experiencea
Specialties.
As a whole, neuroradiologists scored significantly better than nonradiologists (15 ± 8 mm versus 20 ± 14 mm from the foot motor cortex center, P = .005) (Table 4). We then compared within and across specialties on the basis of fMRI experience (no experience versus any experience). In the raters without experience, neuroradiologists were significantly closer than nonradiologists (18 ± 10 mm versus 23 ± 16 mm, P = .036). In raters with experience, there was no significant difference between neuroradiologists (13 ± 6 mm) and nonradiologists (14 ± 6 mm, P = .565). Within specialties, both neuroradiologists and nonradiologists with experience were significantly closer than those without experience (P = 2 × 10−6 and P = 2 × 10−4, respectively). When we crossed both experience and specialties, neuroradiologists with experience were significantly closer than nonradiologists without experience (P = 1.4 × 10−5) and nonradiologists with experience were significantly closer than neuroradiologists without experience (P = .01).
Rater comparisons by specialtya
Arrow Placement in the Motor Gyrus
Raters with fMRI experience correctly placed the arrow in the motor gyrus significantly more often than raters without fMRI experience (67% versus 47%, P = 7 × 10−5). On a gradient, raters in the ≤1 per month group (68%) were correct significantly more often than those without experience (P = 1.1 × 10−4). There were no significant differences between the 2–5 per month (64%) and no experience groups (P = .067) or the 2–5 per month and the ≤1 per month groups (P = .717).
Neuroradiologists were correct significantly more often than nonradiologists (61% versus 46%, P = .008). In raters without fMRI experience, neuroradiologists were correct significantly more often than nonradiologists (54% versus 35%, P = .012). In raters with experience, there was no significant difference between the specialties (neuroradiologists = 68%, nonradiologists = 66%, P = .87). Within specialties, both neuroradiologists and nonradiologists with experience were correct significantly more often (P = .031 and P = .001, respectively). When we crossed both experience and specialties, neuroradiologists with experience were correct significantly more often than nonradiologists without experience (P = 7.68 × 10−6). Nonradiologists with experience did not differ significantly from neuroradiologists without experience (P = .176).
Tumor in the Foot Motor Cortex
In determining whether the tumor was located in the foot motor cortex, there was no significant difference in correct responses based on fMRI experience (no experience = 73%, fMRI experience = 81%, P = .121). Likewise, there was no significant difference among any of the groups along a gradient (0 per month = 73%, ≤1 per month = 80%, 2–5 per month = 86%, P > .174). As a whole, there was no significant difference between the specialties (neuroradiologists = 78%, nonradiologists = 74%, P = .515). Additionally, there was no significant difference between the specialties in those without experience (neuroradiologists = 72%, nonradiologists = 73%, P = .852) or with experience (neuroradiologists = 82%, nonradiologists = 75%, P = .401) or within specialties (neuroradiologists, P = .102; nonradiologists, P = .876). There were no significant differences between neuroradiologists with experience and nonradiologists without experience (P = .217) or nonradiologists with experience and neuroradiologists without experience (P = .746).
Tumor in the Motor Gyrus
In determining whether the tumor was located in the motor gyrus generally, while trending toward significance, there was no significant difference in correct responses based on fMRI experience (no experience = 66%, fMRI experience = 76%, P = .06). Likewise, there was no significant difference among any group along a gradient (0 per month = 66%, ≤1 per month = 74%, 2–5 per month = 83%, P > .076). As a whole, there was no significant difference between the specialties (neuroradiologists = 72%, nonradiologists = 69%, P = .569). Additionally, there was no significant difference between the specialties in those without experience (neuroradiologists = 68%, nonradiologists = 64%, P = .664) or with experience (neuroradiologists = 76%, nonradiologists = 77%, P = .913) or within specialties (neuroradiologists: P = .190, nonradiologists: P = .197). There were no significant differences between neuroradiologists with experience and nonradiologists without experience (P = .111) or nonradiologists with experience and neuroradiologists without experience (P = .304).
Case Example
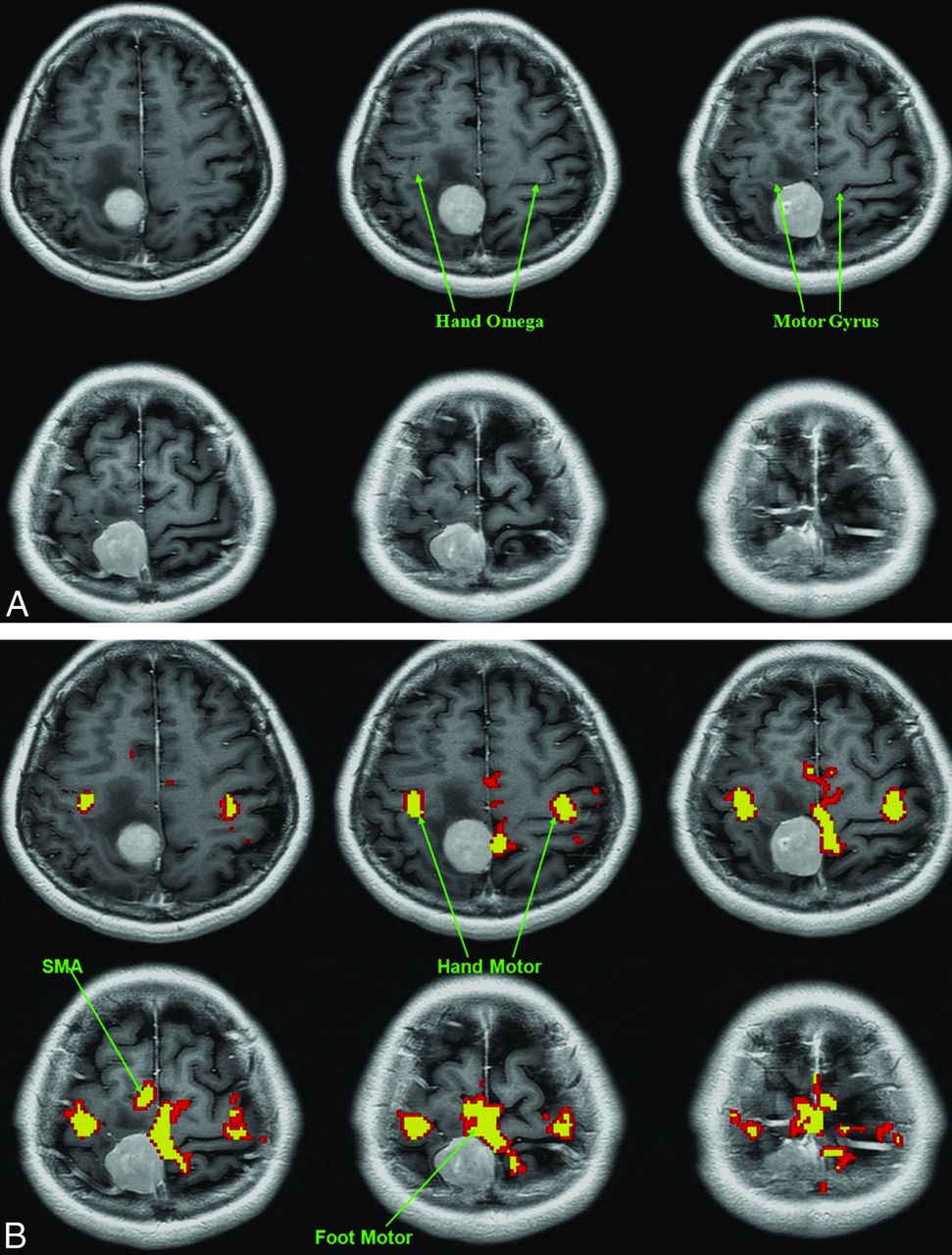
One of the more difficult cases for the raters was patient 13 (Figure). The average distance from the foot motor center in arrow placement was 16 mm in those with fMRI experience and 23 mm in those without experience. Sixty-five percent of raters with fMRI experience and 50% of raters without fMRI experience placed the arrow in the correct gyrus. Eighteen percent and 33% of raters with and without fMRI experience respectively, correctly identified the tumor as not being located in the foot motor cortex. Last, 35% and 39% of raters with and without fMRI experience, respectively, correctly identified the tumor as not being located in the motor gyrus.

Axial T1-weighted without (A) or with (B) coregistered functional MR images obtained during a bilateral finger-tapping and foot motor paradigm. The raters were asked to identify the foot motor homunculus solely on the basis of the anatomic images (A) without the benefit of fMRI (B). fMRI places the extra-axial lesion just posterior to the primary motor gyrus, including the foot motor portion of the motor homunculus. Edema extends to involve both the precentral and postcentral gyri. The average arrow placement from the foot motor center was 16 mm in those with fMRI experience and 23 mm in those without it. A higher percentage of raters with fMRI experience than those without it placed the arrow in the motor gyrus (65% versus 50%). Eighteen percent of raters with fMRI experience correctly identified the tumor as not being located in the foot motor cortex, while 33% of raters without fMRI experience did so. Last, 35% and 39% of raters with and without fMRI experience, respectively, correctly identified the tumor as not being located in the motor gyrus. Most of the incorrect arrow placements were due to the arrow being placed in a gyrus posterior to the motor gyrus.
Discussion
Accurate preoperative identification of eloquent cortices adjacent to brain tumors is essential and has been demonstrated to improve outcomes.8,11 Localization of the foot motor homunculus presents a number of unique challenges because this structure lacks a discernible anatomic landmark on MR imaging such as the “reverse Ω sign” for the hand motor area6 and is difficult to approach and confirm intraoperatively by direct cortical stimulation.8,9 However, accurate localization of the foot motor homunculus is essential because iatrogenic damage and the resultant paresis of the leg can render a patient wheelchair- or bed-bound. In this study, we assessed the ability of physicians from different specialties and with varying fMRI experience to accurately identify the foot motor homunculus on routine MR images.
In this cohort of specialists, we found that experience with fMRI confers a positive effect on reading routine MR imaging examinations in terms of locating the relationship of a tumor to the foot motor homunculus. This effect was seen in those with fMRI experience performing significantly better in foot motor cortex center predictions and arrow placement in the motor gyrus than raters without fMRI experience. This advantage may be linearly related to the degree of fMRI experience, but we did not have the statistical power to show this relationship. There was no significant difference between the 2–5 cases per month group (64% correct) and the ≤1 case per month group (68%). The probable reason that there was no statistically significant difference between the 2–5 cases per month group (64% correct) and the no fMRI experience group (47% correct) was that the 2–5 cases per month group was underpowered: There were 3 raters in the 2–5 cases per month group versus 18 raters in the no experience group and 14 raters in the ≤1 case per month group. Additionally, at the specialist level, neuroradiologists performed significantly better than nonradiologists in foot motor cortex predictions and arrow placement in the motor gyrus. In our study, only 4 nonradiologists had fMRI experience, so how their results would compare with neuroradiologists without fMRI experience in a larger sample size is not known.
In our study, none of the raters, including highly experienced individuals, were 100% correct in identifying the foot motor homunculus on the anatomic MR imaging. Even in healthy volunteers, interobserver agreement on the location of the central sulcus by using MR imaging has been reported to be as low as 76%.12 Therefore, the inability of even expert readers to correctly identify the location of the foot motor homunculus by anatomy alone appears to encourage the use of fMRI in such cases. Localization of the foot motor cortex is of particular importance in preoperative planning in the medial frontoparietal region of the brain.13 If we took the results of previous studies showing comparable motor mapping between fMRI and intraoperative corticography and direct cortical stimulation, fMRI appears to have both validity and utility.11,14
One finding is that the raters did not perform as well in placing the arrow in the motor gyrus as they did in nominally determining whether the tumor was in the motor cortex or in the foot motor area. One reason may be that tumors can span >1 gyrus, thus making it easier to determine whether the motor cortex or foot motor area is affected rather than placing an arrow in the correct gyrus. Another reason for the discrepancy may be that the edema accompanying the tumors increased the difficulty by blurring sulcal boundaries.
The current study has limitations and provides for future directions. One limitation is the sample size of specialists. Future studies might look at a larger number of specialists, include more specialties, and have a wider range of fMRI usage among the cohort to elucidate these comparisons further and inform training programs as to the extent of necessary fMRI training in anatomic determinations such as the foot motor region. Additionally, with the raters given 1 series of axial images for each case, whether additional imaging series might have facilitated foot motor localization is not known. Another consideration would be to see whether the addition of fMRI data actually influenced the surgical decision-making process as in Petrella et al.11 A possible additional limitation is that some of the patients underwent previous surgery. Posttreatment changes, especially involving infiltrative tumors, may limit the determination of the tumor margin, which could affect the results. In addition, a study limitation may be that different tumor types were included, which could have affected the results. However, the current study supports the utility of fMRI for foot motor localization in preoperative planning.
Conclusions
In the current study, we evaluated the ability of neuroradiologists and nonradiologists to identify the foot motor homunculus on MR imaging in patients with brain tumors. None of the 35 raters scored 100% correct. Notwithstanding the expertise of the raters, they were only able to correctly identify whether the tumor was in the foot motor cortex 77% of the time. The inability of experienced readers to consistently identify the location of the foot motor homunculus on routine MR images argues for the use of fMRI in the preoperative setting. In addition, raters with prior fMRI experience were significantly better than raters without experience at foot motor fMRI centroid predictions and arrow placement in the motor gyrus. Therefore, experience in fMRI leads to improved accuracy in identifying anatomic structures even on routine MR imaging. Neuroradiologists were significantly better than nonradiologists at foot motor fMRI centroid predictions and arrow placement in the motor gyrus.
Footnotes
Disclosures: Andrei Holodny—UNRELATED: Other: fMRI Consultants, LLC (a purely educational enterprise).
References
- Received November 20, 2014.
- Accepted after revision January 13, 2015.
- © 2015 by American Journal of Neuroradiology









{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.