
Abstract
BACKGROUND AND PURPOSE: Middle ear space is one of the most important components of the Jahrsdoerfer grading system (J-score), which is used to determine surgical candidacy for congenital aural atresia. The purpose of this study was to introduce a semiautomated method for measuring middle ear volume and determine whether middle ear volume, either alone or in combination with the J-score, can be used to predict early postoperative audiometric outcomes.
MATERIALS AND METHODS: A retrospective analysis was conducted of 18 patients who underwent an operation for unilateral congenital aural atresia at our institution. Using the Livewire Segmentation tool in the Carestream Vue PACS, we segmented middle ear volumes using a semiautomated method for all atretic and contralateral normal ears on preoperative high-resolution CT imaging. Postsurgical audiometric outcome data were then analyzed in the context of these middle ear volumes.
RESULTS: Atretic middle ear volumes were significantly smaller than those in contralateral normal ears (P < .001). Patients with atretic middle ear volumes of >305 mm3 had significantly better postoperative pure tone average and speech reception thresholds than those with atretic ears below this threshold volume (P = .01 and P = .006, respectively). Atretic middle ear volume incorporated into the J-score offered the best association with normal postoperative hearing (speech reception threshold ≤ 30 dB; OR = 37.8, P = .01).
CONCLUSIONS: Middle ear volume, calculated in a semiautomated fashion, is predictive of postsurgical audiometric outcomes, both independently and in combination with the conventional J-score.
ABBREVIATIONS:
- CAA
- congenital aural atresia
- J+
- modified J-score
- J-score
- Jahrsdoerfer grading system
- PTA
- pure tone average
- SRT
- speech reception threshold
Congenital aural atresia (CAA) comprises a spectrum of otologic abnormalities characterized by hypoplasia of the external auditory canal, malformations of the middle ear, and, less commonly, abnormalities of the inner ear. The anomalies occur in varying combinations and severity, with the rate of occurrence of 1 in 10,000 to 1 in 20,000 live births.1 Unilateral atresia is 3–5 times more common than bilateral atresia. It more commonly occurs on the right side and more commonly affects males.2
CAA is more consistently associated with conductive hearing loss, with sensorineural hearing loss seen in a minority of patients. In appropriate patients, surgical restoration of conductive hearing can be achieved through atresiaplasty, which attempts to establish the normal sound-conducting mechanism of the external and middle ear by opening an ear canal into the middle ear space, freeing the ossicular chain, constructing a tympanic membrane using the temporalis fascia, and using a skin graft to create a clean, well-epithelialized, patent external auditory canal (Fig 1).3 Two absolute criteria for surgical candidacy include audiometric or evoked-response evidence of cochlear function and imaging evidence of normal inner ear structures.4 However, surgical correction of CAA is not without potential complications, the most serious of which is facial nerve paralysis. The most common complications of surgery are chronic myringitis, sensorineural hearing loss, soft-tissue external auditory canal stenosis, lateralization of the tympanic membrane, bony regrowth, ossicular chain refixation, and acquired cholesteatoma.2,5 These complications necessitate revision surgery in 25%–33% of patients.5,6

A, Preoperative axial CT image demonstrates a deformed, fused malleus-incus complex (asterisk). The incudostapedial joint is intact (thin arrow). The stapes (thick arrow) and footplate (white arrowheads) are normal. Note the tympanic segment of the facial nerve (black arrowhead) in the normal position. B, Postoperative coronal CT image demonstrates postsurgical changes of canaloplasty and meatoplasty (dashed line). C, Postoperative axial CT image demonstrates postsurgical changes of tympanoplasty (thick white arrows). Note again the fused malleus-incus complex (asterisk), intact incudostapedial joint (thin white arrow), normal oval window (black arrowhead), and tympanic segment of the facial nerve (black arrow).
These potential complications of atresiaplasty underscore the importance of judicious patient selection for surgery. Preoperative high-resolution CT of the temporal bone plays a pivotal role in evaluating surgical candidates and planning the operation.7 While different methods for determining surgical candidacy exist in the literature, the most widely accepted is the Jahrsdoerfer grading system (J-score). The J-score is a 10-point surgical rating scale based on 8 critical areas of temporal bone anatomy on high-resolution CT and the outward appearance of the external ear.4 Each area receives 1 rating scale point, except for the presence of a stapes, which receives 2 points (Fig 2). A J-score of ≤5 disqualifies a patient from surgery; a J-score of ≥7 is most often the threshold used to establish suitable candidacy for surgical repair of CAA. In fact, a patient with favorable anatomy scoring ≥7 has an approximately 85%–90% chance of achieving normal or near-normal hearing postoperatively.8

Schematic diagram of the ear (left) with corresponding color-coded structures used in the calculation of the Jahrsdoerfer score (right), which is used in evaluating a patient's surgical candidacy preoperatively for congenital aural atresia.
However, certain individual components of the J-score are themselves indispensable for successful surgery and often supersede the overall J-score. One such component is the middle ear space, because reduced middle ear space has been correlated independently with unfavorable postsurgical outcomes.8,9 Most surgeons will not perform atresiaplasty without a well-aerated middle ear. Yet, the exact definitions of middle ear space and surgically appropriate middle ear aeration remain quite subjective. The purpose of this study was to evaluate the efficacy of a semiautomated method of measuring middle ear space, which allows a more objective and reproducible method of ascertaining this space. In addition, we assessed whether middle ear volume derived with this method can be used, either independently or in combination with the J-score, to more accurately predict early postoperative audiometric outcomes compared with the J-score alone.
Materials and Methods
This study was a retrospective institutional review board–approved review of patients who had primary repair of their unilateral CAA by a single surgeon from January 2012 to December 2015. Patients were selected if they had adequate preoperative temporal bone high-resolution CT imaging and presurgical and postsurgical audiometric testing to include pure tone average (PTA), speech reception threshold (SRT), air-bone gap, and the speech discrimination score on both the atretic and contralateral normal ears. High-resolution CT bone windows, comprising 0.63- to 1.0-mm-thickness axial sections, were used for analysis. Coronal and sagittal multiplanar reconstructions were performed at the workstation as necessary.
J-scores were determined by the operating surgeon before the start of this study for each of the atretic ears in conventional fashion as previously detailed in the literature.10 This included assigning a single point for middle ear space based on a single linear measurement from the cochlear promontory medially to the atretic plate laterally. All patients in this study had a J-score of ≥7.
Middle ear volumes were measured in a semiautomated fashion for all atretic ears and contralateral normal ears. The boundaries of the middle ear space were defined according to conventional anatomy as follows: roof, tegmen tympani; floor, jugular fossa; medial, bony labyrinth; lateral, tympanic membrane (normal ear) or atretic plate (atretic ear); anterior, carotid wall; and posterior, mastoid antrum.
For each ear, semiautomated volumetric measurements of the middle ear were performed using the Livewire Segmentation tool in Carestream Vue PACS (Carestream Health, Rochester, New York), with all measurements performed by a single board-certified radiologist. First, manual segmentation of the middle ear space was performed on every second axial section through the volume of interest by drawing an outline around the desired space, including on the superiormost and inferiormost sections, to establish the craniocaudal boundaries of the volume. On completion of manual segmentation, the imaging tool interpolated the segmentations on the remaining intervening axial sections in an automated fashion. Manual corrections were made to the interpolated sections as necessary if the interpolated outlines veered too far from the true outline of the middle ear space as determined by the performing radiologist. Once the segmentations on each continuous axial section in the desired volume were deemed appropriate, the tool constructed a 3D space from the outlined area of interest and reported the volume of the space in cubic millimeters (Figs 3⇓–5). All segmentations and volumes were finally reviewed by a board-certified neuroradiologist and otologic surgeon for accuracy.

A normal ear with middle ear volume of 592 mm3. Coronal CT reconstruction (left) and corresponding axial CT images (right) in different regions of the middle ear demonstrate accurate semiautomated segmentation of the middle ear space.

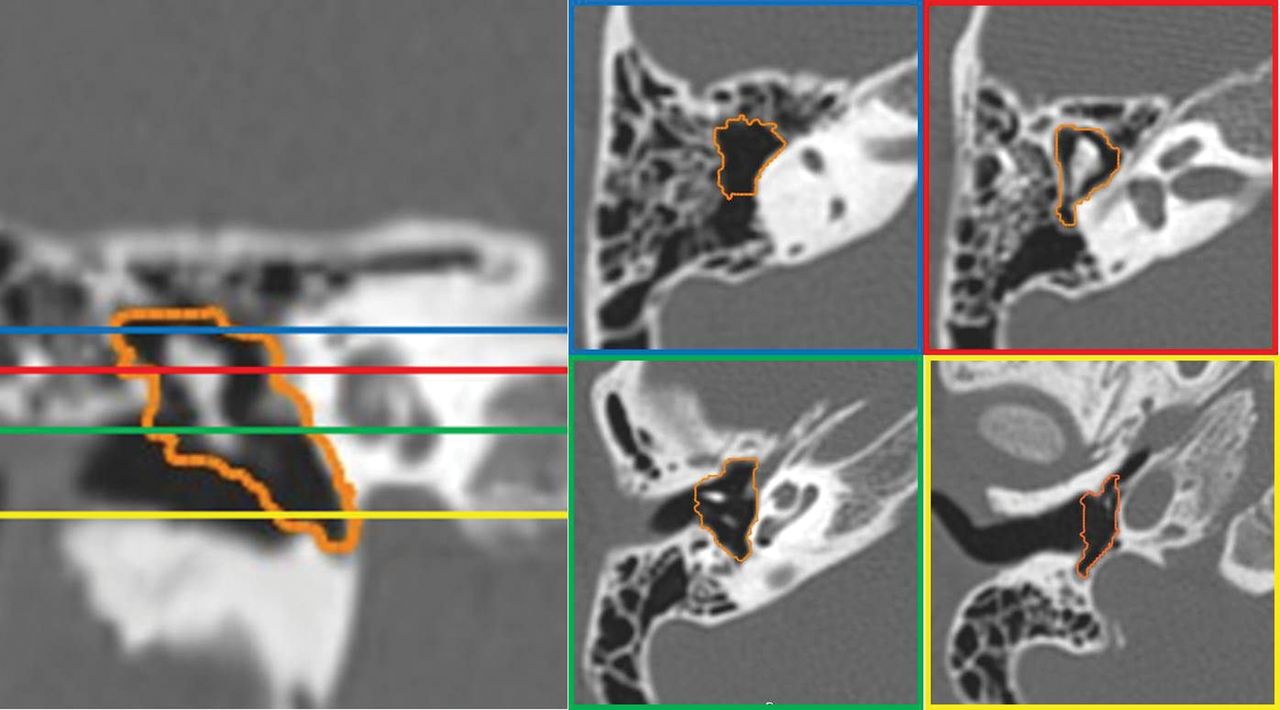
An atretic ear with middle ear volume of 362 mm3 and a J-score of 8. Coronal CT reconstruction (left) and corresponding axial CT images (right) in different regions of the middle ear demonstrate accurate semiautomated segmentation of the middle ear space.

An atretic ear with middle ear volume of 251 mm3 and a J-score of 7. Coronal CT reconstruction (left) and corresponding axial CT images (right) in different regions of the middle ear demonstrate accurate semiautomated segmentation of the middle ear space.
Comparison among independent group means was performed using a Student t test; and among dependent data, using paired t testing. The Pearson correlation coefficient (r) and linear regression (R2) were used to assess association among variables. The Fisher exact test was used to compare postoperative auditory outcomes among groups, and statistical significance was set at a P value < .05. Postoperative normal audiometric thresholds were defined as <30-dB sound pressure level. Calculations were performed on GraphPad Prism software (GraphPad Software, San Diego, California).
Results
Eighteen patients with unilateral CAA met the inclusion criteria and were used in our data analysis. Thus, 18 atretic ears and 18 contralateral normal ears were used for comparative analysis. There were more males than females, and most atretic ears affected the right side in our data. Audiometric follow-up testing occurred at least 6 weeks after surgery (average, 9 weeks; range, 6–35 weeks). All patients had improved PTA and SRT thresholds after primary atresia repair. Eight of the atretic ears (44.4%) achieved normal postoperative PTA, and 13 (72.2%) achieved normal postoperative SRT levels. Complete demographics of our patient population may be found in Table 1.
Patient demographics
Traditional Jahrsdoerfer Score
Although there was a positive trend, traditional J-scores did not significantly correlate with atretic middle ear volume (Pearson r = 0.4122, R2 = 0.1699, P = .0892). Thus, higher J-scores were not associated with larger middle ear volumes. However, higher J-scores correlated with better postoperative PTA and SRT (Pearson r = −0.4759, R2 = 0.2265, P = .04637; and Pearson r = −0.5024, R2 = 0.2524, P = .0336, respectively). J-scores of ≥8 were not significantly associated with normal postoperative PTA (P = .2174) or with normal postoperative SRT thresholds (P = .0770).
Middle Ear Volume
Atretic middle ear volumes were significantly smaller than contralateral normal ears (346 versus 627 mm3, P < .0001). Middle ear volume alone did not correlate with postoperative PTA or SRT (Pearson r = −0.2816, R2 = 0.0793, P = .2577; and Pearson r = −0.4242, R2 = 0.18, P = .0793, respectively). Using regression analysis to maximize sensitivity and specificity, we found that patients with atretic middle ear volumes of >305 mm3 had significantly better postoperative PTA and SRT thresholds compared with patients with smaller volumes (P = .0098 and P = .0062, respectively) (Fig 6). Middle ear volume above 305 mm3 was not significantly associated with normal postoperative PTA (P = .1185) but was significantly associated with normal postoperative SRT thresholds (P = .0368).

Atretic middle ear volumes of >305 mm3 had significantly better postoperative pure tone average and speech reception threshold than atretic ears below this threshold volume.
Modified J-Score
The calculated middle ear volume was incorporated into the traditional J-score as an objective measure. A volume of ≥305 mm3 was given 1 point, and a volume of less than this was not given a point in the middle ear space category. Using this objective measure, we assessed the modified J-score (henceforth referred to as the J+ score) for its correlation to postoperative hearing outcomes in the atretic ears. Higher J+ scores were associated with better postoperative PTA and SRT (Pearson r = −0.6327, R2 = 0.43, P = .0048; and Pearson r = −0.6784, R2 = 0.4602, P = .002, respectively) (Fig 7). Atretic ears with a J+ score of ≥8 were found to have better postoperative PTA and SRT thresholds than those below this score (P = .0042 and P = .0017, respectively) (Fig 8). A J+ score of ≥8 was not significantly associated with normal postoperative PTA (P = .2451) but was significantly associated with normal postoperative hearing (SRT ≤ 30 dB, P = .0123). Table 2 demonstrates the number of patients with normal postoperative PTA and SRT stratified by the traditional J-score, middle ear volume, and J+ score.

Higher J+ scores were associated with better postoperative pure tone average and speech reception threshold.

Atretic ears with a J+ score of ≥8 had significantly better postoperative pure tone average and speech reception threshold than those below this threshold score.
Number of patients who achieved normal postoperative audiometric outcomes
Discussion
Middle ear aeration is regarded by many as the most important component of the J-score when determining surgical candidacy. Specifically, reduced middle ear space has been independently associated with unfavorable postsurgical outcomes.8,11 Lack of middle ear aeration may result in difficulty identifying a middle ear space and ossicular chain during drilling, refixation of the ossicular chain postoperatively, and postoperative stenosis with a constricted middle ear space and smaller tympanic membrane.8 However, the definition of middle ear space remains vague and subject to individual interpretation. In most cases of CAA, the middle ear space is indeed small, and a threshold for discriminating surgical adequacy is not well-established in the literature.
As part of the J-score, middle ear space is defined as a single linear measurement from the cochlear promontory medially to the atretic plate laterally, with a measurement of <3 mm receiving no point on the scale.10 This region of the tympanic cavity is likely chosen due to its surgical relevance because smaller sizes may be associated with ossicular fixation and poorer hearing outcomes. However, using a single linear measurement within the middle ear space has the adverse potential of mischaracterizing the totality of the middle ear space and ultimately mischaracterizing surgical candidacy.
Attempts at more comprehensive measurement of the middle ear space have been described more recently in the literature. Specifically, middle ear space has been defined using 6 CT linear dimensions of the middle ear that have surgical relevance and are key indicators of topographic anatomy.11 These linear measurements were used to derive mesotympanic volume, modeled as a rectangular prism as the product of mesotympanic length, width, and height. However, modeling the middle ear space as a rectangular prism is not anatomically sound because the irregular shape and contours of the middle ear prohibit simple geometric modeling and inevitably result in imprecise volume determinations. In addition, the process of measuring 6 different dimensions at specific landmarks is relatively cumbersome for routine clinical practice and is more prone to interobserver variability.
In our experience, the semiautomated method proposed in this study not only measures the entire middle ear volume more efficiently than any method in existing literature but does so more accurately by conforming to the abrupt contour changes of the tympanic cavity by outlining the desired space on each continuous axial section (either manually or through interpolation). Using this method, we demonstrate that middle ear volumes of >305 mm3 had significantly better postoperative PTA and SRT compared with atretic ears below this threshold volume. When this threshold volume of 305 mm3 is used as part of the new J+ score as described above, a J+ score of ≥8 is predictive of better postoperative PTA and SRT. Furthermore, the J+ score correlates with better postoperative audiometric outcomes than the classic J-score. Thus, semiautomated derivation of middle ear volume is predictive of postsurgical audiometric outcomes both independently and in combination with the classic J-score.
Our numeric volume measurement of a normal middle ear volume of 627 mm3 is in agreement with existing literature, which describes a normal adult middle ear cavity volume of 640 mm3.12 Our results are also in concordance with existing literature, which describes middle ear volume calculation by full manual segmentation.13 In their study, using the same anatomic boundaries of the middle ear space as in our study, Osborn et al13 demonstrated a statistically significant difference in mean volume between surgical candidate ears versus those of noncandidates and concluded that volumes derived through manual segmentation can serve as independent predictors of overall surgical candidacy. We believe our study improves on the methodology by using semiautomated segmentation instead of full manual segmentation and correlates middle ear volumes with postsurgical audiometric data rather than just discriminating between candidate and noncandidate ears.
The importance of judicious patient selection for atresiaplasty has become more significant due to recent literature suggesting suboptimal audiometric outcomes after atresiaplasty for CAA. Specifically, in a large systematic review, audiometric outcomes of patients undergoing atresiaplasty were shown to be poorer in comparison with audiometric outcomes of patients receiving an osseointegrated bone-conduction device.14 Certainly much of this finding is attributable to the considerable difficulty in performing atresiaplasty, which is considered one of the more difficult otologic operations due to intricate anatomic considerations and a high risk of complications. However, patient selection for atresiaplasty may also play a considerable role. This makes the results of our study more engaging because our demonstration of the improved association of the J+ score with normal postoperative hearing may provide an opportunity for more appropriate selection of patients who would benefit most from atresiaplasty.
However, there are several limitations to this study, specifically regarding the semiautomated methodology of segmentation. First, while the boundaries of the tympanic cavity are well-defined anatomically, their identification on high-resolution CT images is often inexact and subject to individual interpretation, resulting in the possibility of significant interobserver variability. Future work in implementing this method should include interobserver data validation to confirm the precision of middle ear volume measurement. Second, manual corrections to the interpolated outlines were required in most cases due to the abrupt irregular contour changes of the middle ear space on serial sections, which can only be negotiated by computer software to a limited extent. However, the manual corrections required can be performed rather quickly with the segmentation tool; thus, they still result in substantial overall time savings compared with complete manual segmentation. Finally, only patients with a J-score of ≥7 were included in our analysis. This is a limitation inherent with any study that includes atresia repair outcomes because patients with a J-score of <7 are unlikely to undergo surgery.
While we show a statistically significant correlation between middle ear volume and postsurgical outcomes, questions remain as to the intuitive importance of the entire middle ear space surgically. The epitympanum is known to be important surgically because it serves as the entry point into the middle ear during atresiaplasty. Similarly, the surgical relevance of the mesotympanum lies in its housing of critical middle ear components, including the stapes and oval window. However, the hypotympanum is rarely visualized during atresiaplasty and is not particularly relevant for surgery.11 Therefore, in future work, it may be prudent to exclude the hypotympanum in middle ear volume calculations and evaluate whether similar, or perhaps stronger, correlation is found with postsurgical audiometric outcomes.
Further work may also focus on long-term postsurgical audiometric outcomes and whether improved outcomes persist several years after the operation if such data are available. Additional investigation may also be needed into the appropriateness of using a universal cutoff value for middle ear volume in determining surgical candidacy for atresiaplasty, regardless of age, because one can reasonably assume that middle ear volumes may increase during childhood. However, no normalized values for middle ear volumes as a function of age are currently available to aid in developing potential age-specific middle ear volume thresholds.
Conclusions
Middle ear aeration may be the most important predictor of surgical success for CAA. Yet, the characterization of adequate middle ear space in the context of surgical candidacy for CAA remains ambiguous. Current definitions of middle ear space are predominantly composed of linear measurements at arbitrarily chosen landmarks, which fail to adequately encompass the totality of the middle ear cavity. This study introduces a semiautomated method of measuring the entire volume of the middle ear using segmentation software, which the authors believe is a more useful representation of middle ear space in a surgical context. Middle ear volumes derived in this fashion are associated with better postsurgical audiometric outcomes, both independently and in combination with the J-score (J+ score) when a threshold value of 305 mm3 is used to assign a point on the scale. The J+ score correlates with postoperative hearing outcomes better than either the classic J-score or middle ear volume alone and may be used preoperatively to better determine surgical candidacy.
Footnotes
Disclosures: Bradley W. Kesser—UNRELATED: Payment for Lectures Including Service on Speakers Bureaus: DePuy Synthes, Comments: I received a single honorarium for a lecture and taught a temporal bone course*; Royalties: Nasco, Comments: I received royalties for an ear simulator that I and my colleagues patented and licensed to Nasco*. *Money paid to the institution.
Paper previously present as an abstract at: Annual Meeting of the American Society of Neuroradiology and the Foundation of the ASNR Symposium, April 22-27, 2017; Long Beach, California.
References
- Received July 12, 2017.
- Accepted after revision October 3, 2017.
- © 2018 by American Journal of Neuroradiology









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.