
Abstract
The rapid development and wider use of neurointerventional procedures have increased the demand for a comprehensive training program for the trainees, in order to safely and efficiently perform these procedures. Artificial vascular models are one of the dynamic ways to train the new generation of neurointerventionists to acquire the basic skills of material handling, tool manipulation through the vasculature, and development of hand-eye coordination. Herein, the authors present their experience regarding a long-established training program and review the available literature on the advantages and disadvantages of vascular silicone model training. Additionally, they present the current research applications of silicone replicas in the neurointerventional arena.
Similar content being viewed by others



Introduction
Neurointervention procedures and their tools have rapidly evolved over the years after the introduction of the Guglielmi detachable coils (GDCs) [13, 14] to treat aneurysms and various other vascular and neoplastic diseases previously regarded as not treatable or managed by other means. This accelerated development and wider use of neurointerventional procedures have increased the demand for a comprehensive training program for the trainees [18, 21], in order to safely and efficiently perform these techniques. Artificial vascular models are one of the dynamic ways to train the new generation to acquire the basic skills of equipment handling and material manipulation through the vasculature and development of hand-eye coordination. These basic abilities should be acquired in the lab prior to working on patients. Herein, the authors present their experience regarding a long-established training program and review the available literature on the advantages and disadvantages of vascular silicone model training. Additionally, they present the current research applications of silicone replicas in the neurointerventional arena.
Materials and methods
In vitro vascular model
The model used in our institution (Department of Neuroradiology, University Hospital of Zurich, Zurich, Switzerland) is a flow silicone vascular phantom model manufactured by Elastrat Sàrl (Geneva, Switzerland) (Fig. 1). It is made of soft, transparent silicone calibrated in shape and curvatures to mimic the human vasculature. The model incorporates the essential vasculature of the torso, neck, and cranium. Aneurysms at most common and ordinary locations are also included. The cranial part can be detached, and another model with variable configuration can be attached to avoid repetition. A pump is used to inject tap water mixed with a special liquid provided by the manufacturers in a ratio of 7:3 to reduce friction, as well as to make the circulating fluid similar in rheological properties to blood. These replicas are compatible with modern imaging modalities (subtraction angiography, computed tomography, magnetic resonance imaging, Doppler techniques). Moreover, their transparency to light makes them suitable for video and photographic monitoring.

The workstation provides a realistic environment for the simulation of endovascular procedures facilitating the learning experience (reproduced from the website: http://www.elastrat.ch/index.php?option=com_content&task=blogcategory&id=24&Itemid=83)
The endovascular environment
The endovascular environment is created based on a closed circulation circuit with the only opening being the port of vascular entry. This is big enough to allow 5, 6, and 7 F catheter insertion in the femoral artery. The fluid is pumped using an electric motor, and the flow is directed in such a way as to mimic the flow in the human body, with downward flow in the aorta and upward flow in the cervical and cranial vessels.
Training system
The training system is made as realistically as possible, in the context of a uniplane angiographic suite with capabilities of digital subtraction, road mapping, and video recording. The silicone model is positioned on the table instead of a patient. Fellows are taught to handle the tools and materials and improve their manipulation techniques. They are allowed to work on the model under supervision, strictly following the technical principles of interventional neuroradiology. Evaluation in real time can be done through the monitors that are located inside and outside the angio suite.
Results
In the time period 1996–2012, 178 fellows from 33 countries took part in the formal International Fellowship Program on Interventional Neuroradiology offered by our department.
Training on the dedicated neuroendovascular models takes place in the neuroangiographic laboratory for training, research, and development of our department. It is completed in three phases:
-
Phase 1:
-
1.
Working in larger arteries, with 5 and 6 F catheters, learning to safely hook each of the major vessels and to do catheter exchange (Fig. 2).
-
2.
Doing road map and navigating within the map.
Fig. 2 
Left internal carotid artery injection
-
1.
-
Phase 2:
-
1.
Handling and manipulating the microcatheters.
-
2.
Shaping of microcatheters and guidewires.
-
3.
Navigating through the cranial circulation with various vessel combinations.
-
4.
Obtaining the working projection.
-
1.
-
Phase 3:
-
1.
Learning the selection, delivery, and detachment of the coils with adequate packing of the aneurysm.
-
2.
Learning balloon- and stent-assisted coiling of wide-necked aneurysms, familiarizing with the double-microcatheter techniques, and getting accustomed to the use of nondetachable silicone balloons and stents (Fig. 3).
Fig. 3 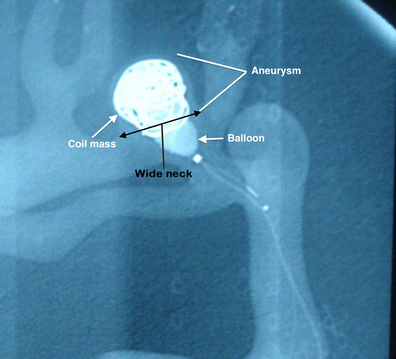
Balloon remodeling technique application in a wide-necked aneurysm
-
1.


As the training progresses, the trainees are periodically assessed as to the improvement in their performance for the following factors:
-
1.
Manipulation of the angiographic machine and the table in a coordinated fashion.
-
2.
Tool and material handling.
-
3.
Hand-eye coordination.
-
4.
Endovascular techniques.
In our institution, apart from training the beginners, the models are also used for testing newer devices such as new coils, stents, and thrombectomy devices, before being used in patients. In particular, their physical characteristics and their behavior are tested, and the technique of using the device is practiced. We found that this approach improves both the familiarity and the ease of handling the devices. During this process, some devices were evaluated as appropriate to use while others were not favored.
Discussion
The necessity of such programs
Neuroendovascular operations are among the complex and the highest-risk operations in medicine. The cerebral circulation is different from that of other organs not just by virtue of its complex anatomy and vascular pathology, but more importantly by virtue of the impact of inadvertent complications. The need for excellent technical training backed up by a thorough knowledge of the diseases of the neurovascular system is self-evident [23]. As the number of specialized centers around the world is increasing, there are relatively fewer cases in each center treated. So, acquisition of technical skills by the next generation of neurointerventionists is based mainly on alternative methods of learning, like animal models, silicone models, and computer-based simulation technology. Among the aforementioned training methodologies, silicone model training exhibits considerable advantages. These together with some unavoidable drawbacks are illustrated below.
Advantages of silicone models
To start with, learning to handle the endovascular tools and the angiographic machine properly (follow the catheter, road mapping technique, etc.) is of utmost importance. Most microwires and microcatheters are fine; they have to be handled meticulously to avoid damage before and during their usage. Learning the basic operative skills, like hooking of a vessel, guidewire manipulation, catheter exchange, shaping of microcatheters and guidewires, and coil placement, are all learned in a stepwise manner effectively and as realistically as possible. Initially, the learning is voluntary with conscious orientation of hand-eye coordination. However, after repeated learning cycles, the manipulation becomes subconscious.
The models are also useful for testing new materials or devices [11, 20, 24, 26, 29, 33, 35]. Not only is the technique of their deployment learned, but also their physical behavior is controlled, before these are used in patients [22, 41]. The silicone models provide a fair sample of the real anatomy along with an opportunity to practice a number of technical and problem-solving skills [23, 36]. The anatomy may well be modified by introducing more challenging situations to refine techniques and to learn new tricks. The silicone models, apart from being compatible with angiographic studies [3, 22, 33], are transparent enough to allow direct visualization [13, 33, 36] to learn the three-dimensional (3D) behavior of coils during deployment [3, 17, 22]. Another distinct advantage is the sparing of expensive animal models [33]. Moreover, in animal models, extracranial vascular territories are used which are not a representative of the cerebrovascular system, whereas in silicone models, numerous solutions for modifying the perivascular environment exist (i.e., simulating the petrous canal with mold materials or simulating the brain with ballistic gel). The silicone models are good enough for basic training purposes as they provide artificial but realistic, safe, and reproducible test conditions [23, 33].
Disadvantages of silicone models
The training in silicone models is not without disadvantages. One of the major drawbacks encountered is the higher coefficient of friction and thus the higher resistance to catheters and guidewires during manipulation compared with real patients, especially when passing various devices through curved vessels [36]. To reduce the friction in our models, the circulating fluid is made slimier with the lubricating fluid supplied by the manufacturing company. Still friction remains a significant limiting factor. As stated by Cheuh et al. [5], models made of polyvinyl alcohol-hydrogel (PVA-H) are an alternative. PVA-H models demonstrate much lower friction, more elasticity, and allow pulsatile flow but have much shorter life than silicone models. To overcome the problem, the same authors have also suggested coating the inner layer of the silicone models with parylene or liquid silicone rubber (LSR) top coat [5]. An additional inherent drawback of silicone models is the need to remove devices from the replicas once deployed so that the models can be reused. This, although sometimes troublesome, can be done through the connection points of the models.
Admittedly, vascular models are few and fixed with limited variations [13, 36]. The trainees quickly learn the manipulation in few attempts in each of the models and, in this sense, the capability of the trainees is not fully tested. In the models, the aneurysmal wall has the same thickness as the other parts of the models, lacking fragility [13]. Moreover, the feeling of controlled deployment is not attained while coiling such thick walled cavities, and percutaneous transluminal angioplasty (PTA) and stenting in cases of stenosis achieve much less dilation than expected or intended [36]. Training on vascular models bears undoubtedly the inherent danger that the trainees develop a “wrong security” due to the evident absence of in vivo conditions like fragility of the vessels and lesions, spastic reaction of arteries, and occurrence of thromboembolic phenomena. It is therefore mandatory that the trainees are being continuously reminded by the supervisor about this central limitation during their training on models. Furthermore, it is essential that this training for the beginner in the field takes place in parallel with the observation of in vivo procedures.
In addition, the models include the major vessels of the brain but lack the distal cortical vasculature. As a result, manipulation of microwires and microcatheters in such small vasculature is not learned. Moreover, modeling of perforators is lacking; this is a consideration when training microwire navigation. Furthermore, there are no good arteriovenous malformation (AVM) models, not to mention that the flow dynamics of AVMs are extremely difficult to reproduce. Additionally, although flow-directed microcatheters can be used in these models, the lack of preferential flow renders their use and the overall training much limited. Finally, the technique of glue and/or particle injection cannot be learned from the silicone models, and the testing of biocompatibility is not possible due to the absence of biological conditions [33]. It is important to keep in mind that as we test new medical devices in such models, we are actually testing only their physical characteristics.
The fluoroscopic road-mapping simulation with a combination of silicone and animal-based models seems to be a more practical approach in addressing the issues raised above. Of major significance would also be the use individualized models instead of a standard model [36]. With this in mind, many studies have been conducted in the last 2 decades. The main objectives of this research are presented in the following section.
Research topics
The aforementioned advantages have drawn the attention of researchers to the application of silicone models in a great variety of research areas. Table 1 presents several studies conducted in the last years using silicone models with special interest in coils [3, 4, 12, 17, 19, 22, 25, 27–32, 34, 39, 41] and stents [2, 3, 8, 10, 19, 37, 38, 40].
Liquid embolic agents have also been tested. Imbesi et al. [15] evaluated the efficacy of such agents while studying the changes in the aneurysm flow dynamics after placing a nondetachable balloon in the parent vessel. Piotin et al. [29] determined the effectiveness of filling the cavity of aneurysms with detachable platinum coils and the combination of detachable platinum coils and a liquid embolic agent (tricellulose acetate polymer).
Other researchers focused on flow dynamics in aneurysms [1, 2, 4, 9, 10, 12, 15, 16, 31, 38]. For example, Acevedo et al. [1] used phase-contrast MRI computational fluid dynamics flow simulations. Barath et al. [2] evaluated hemodynamic changes induced by the implantation of a stent, and Fujimura et al. [10] quantified flow reduction in aneurysmal cavities produced by stent implants used for flow diversion. The intra-aneurysmal flow characteristics before and after the placement of self-expanding stents were assessed by Tateshima et al. [38]. In addition, Cantón et al. [4] measured the changes in the intra-aneurysmal fluid pressure and parent vessel flow characteristics resulting from packing the aneurysmal sac with hydrogel-coated platinum coils, and the influence of flow dynamics in the parent vessel and of intra-aneurysmal coil embolization on flow pattern and pressure was investigated by Gobin et al. [12]. Furthermore, Sorteberg et al. [31] determined whether changes in pressure and flow observed after coiling are the result of the presence of coils plus thrombus (hemodynamic effect) or the result of the presence of the coils themselves (hydrodynamic effect). The complicated flow dynamics of internal carotid artery was studied by Kerber et al. [16]. Finally, the impact of the geometric configuration of parent artery in relation to the aneurysm on the 3D rotational angiography has also been assessed [9].
Moreover, new materials and devices have been tested in silicone models [20, 24, 26]. Oechtering et al. [26] tested intra-arterially administered magnetic microparticles for embolization of aneurysms with assistance from an external magnetic field. Matsubara et al. [20] developed a new sensor device to measure the coil insertion pressure via an optical system, and Müller-Hülsbeck et al. [24] evaluated the efficacy of filtration devices designed for cerebral protection during carotid angioplasty.
Stroke research has also been benefited from these models [6, 7]. For example Chung et al. studied the relationship among arterial topology, blood flow, and embolus trajectory and reported that embolus trajectory through the cerebral arteries is dependent on embolus size and strongly favors the middle cerebral artery for large emboli [7]. Chueh et al. assessed the effectiveness of mechanical endovascular thrombectomy in a model system of cerebrovascular occlusion [6]. The researchers found that the recanalization rate of the thrombectomy device was associated with the ability of the device to capture the clot during removal and the geometry of the cerebral vessels. In addition, the risk of embolic shower was influenced by the mechanism of action for the thrombectomy device [6].
Conclusion
Training with silicone models is a useful way to familiarize the younger generation of interventionists with the basic principles and techniques of interventional neuroradiology. The skills are acquired rapidly and safely in a phased manner from simple to complex tasks. In spite of certain disadvantages, the authors still feel that this training modality is good enough not only for learning the basic techniques, but also for assisting the scientific research and development.
References
Acevedo-Bolton G, Jou LD, Dispensa BP, Lawton MT, Higashida RT, Martin AJ, Young WL, Saloner D (2006) Estimating the hemodynamic impact of interventional treatments of aneurysms: numerical simulation with experimental validation: technical case report. Neurosurgery 59(2):429–430
Barath K, Cassot F, Rüfenacht DA, Fasel HD (2004) Anatomically shaped internal carotid artery aneurysm in vitro model for flow analysis to evaluate stent effect. AJNR Am J Neuroradiol 25(10):1750–1759
Bendok BR, Parkinson RJ, Hage ZA, Adel JG, Gounis MJ (2007) The effect of vascular reconstruction device-assisted coiling on packing density, effective neck coverage, and angiographic outcome: an in vitro study. Neurosurgery 61(4):835–841
Cantón G, Levy DI, Lasheras JC (2005) Changes in the intraaneurysmal pressure due to HydroCoil embolization. AJNR Am J Neuroradiol 26(4):904–907
Chueh JY, Wakhloo AK, Gounis MJ (2009) Neurovascular modelling: small batch manufacturing of silicone vascular replicas. AJNR Am J Neuroradiol 30(6):1159–1164
Chueh JY, Wakhloo AK, Gounis MJ (2012) Effectiveness of mechanical endovascular thrombectomy in a model system of cerebrovascular occlusion. AJNR Am J Neuroradiol 33(10):1998–2003
Chung EM, Hague JP, Chanrion MA, Ramnarine KV, Katsogridakis E, Evans DH (2010) Embolus trajectory through a physical replica of the major cerebral arteries. Stroke 41(4):647–652
Du Mesnil de Rochemont R, Yan B, Zanella FE, Rüfenacht DA, Berkefeld J (2006) Conformability of balloon-expandable stents to the carotid siphon: an in vitro study. AJNR Am J Neuroradiol 27(2):324–326
Ernemann UU, Grönewäller E, Duffner FB, Guervit O, Claassen J, Skalej MD (2003) Influence of geometric and hemodynamic parameters on aneurysm visualization during three-dimensional rotational angiography: an in vitro study. AJNR Am J Neuroradiol 24(4):597–603
Fujimura N, Ohta M, Abdo G, Ylmaz H, Lovblad KO, Rüfenacht DA (2006) Method to quantify flow reduction in aneurysmal cavities of lateral wall aneurysms produced by stent implants used for flow diversion. Interv Neuroradiol 12(Suppl 1):197–200
Gailloud P, Muster M, Piotin M, Mottu F, Murphy KJ, Fasel JHD, Rüfenacht DA (1999) In vitro models of intracranial arteriovenous fistulas for the evaluation of new endovascular treatment materials. AJNR Am J Neuroradiol 20(2):291–295
Gobin YP, Counord JL, Flaud P, Duffaux J (1994) In vitro study of haemodynamics in a giant saccular aneurysm model: influence of flow dynamics in the parent vessel and effects of coil embolization. Neuroradiology 36(7):530–536
Gruber A, Bavinszki G, Killer M, Shameri A, Richling B (1998) In vitro training model for endovascular embolization of cerebral aneurysms. Minim Invasive Neurosurg 40(4):121–123
Guglielmi G, Vinuela F, Dion J, Duckwiler G (1991) Electrothrombosis of saccular aneurysms via endovascular approach. Part 2: preliminary clinical experience. J Neurosurg 75(1):8–14
Imbesi SG, Knox K, Kerber CW (2003) Aneurysm flow dynamics: alterations of slipstream flow for neuroendovascular treatment with liquid embolic agents. AJNR Am J Neuroradiol 24(10):2044–2049
Kerber CW, Heilman CB (1992) Flow dynamics in the human carotid artery: I. Preliminary observations using a transparent elastic model. AJNR Am J Neuroradiol 13(1):173–180
Majidi S, Khatri R, Watanabe M, Siddiq F, Chaudhry SA, Qureshi AI (2012) Aneurysm embolization using detachable coils under intravascular ultrasonography guidance: an in vitro feasibility study. Neurosurgery 70(6):1557–1564
Malisch TW, Guglielmi G, Vinuela F, Duckwiler G, Gobin YP, Martin NA, Frazee JG (1997) Intracranial aneurysms treated with the Guglielmi detachable coil: midterm clinical results in a consecutive series of 100 patients. J Neurosurg 87(2):176–183
Martin JB, Murphy KJ, Gailloud P, Sugiu K, Treggiari MM, Muster M, Guimaraens L, Théron JG, Rüfenacht DA (2001) In vitro evaluation of the effectiveness of distal protection in the prevention of cerebral thromboembolism during carotid stent placement. Acad Radiol 8(7):623–628
Matsubara N, Miyachi S, Nagano Y, Ohshima T, Hososhima O, Izumi T, Tsurumi A, Wakabayashi T, Sakaguchi M, Sano A, Fujimoto H (2009) A novel pressure sensor with an optical system for coil embolization of intracranial aneurysms. J Neurosurg 111(1):41–47
McDougall CG, Halbach VV, Dowd CF, Higashida RT, Larsen DW, Hieshima GB (1998) Causes and management of aneurismal hemorrhage occurring during embolization with Guglielmi detachable coils. J Neurosurg 89(1):87–92
Mehra M, Hurley MC, Gounis MJ, King RM, Shaibani A, Dabus G, Labdag FE, Levy EI, Bendok BR (2011) The impact of coil shape design on angiographic occlusion, packing density and coil mass uniformity in aneurysm embolization: an in vitro study. J Neurointerv Surg 3(2):131–136
Morris PP (2007) Practical neuroangiography. Lippincott Williams & Wilkins, Philadelphia
Müller-Hülsbeck S, Jahnke T, Liess C, Glass C, Paulsen F, Grimm J, Heller M (2002) In vitro comparison of four cerebral protection filters for preventing human plaque embolization during carotid interventions. J Endovasc Ther 9(6):793–802
Murphy KJ, Mandal S, Gailloud P, Clint H, Szoplnskl K, Qule H, Martin JB, Rüfenacht DA (2000) Neurovascular embolization: in vitro evaluation of a mechanical detachable platinum coil system. Radiology 217(3):904–906
Oechtering J, Kirkpatrick PJ, Ludolph AGK, Hans FJ, Sellhaus B, Spiegelberg A, Krings T (2011) Magnetic microparticles for endovascular aneurysm treatment: in vitro and in vivo experimental results. Neurosurgery 68(5):1388–1398
Piotin M, Iijima A, Wada H, Moret J (2003) Increasing the packing of small aneurysms with complex-shaped coils: an in vitro study. AJNR Am J Neuroradiol 24(7):1446–1448
Piotin M, Liebig T, Dalle Feste C, Spelle L, Mounayer C, Moret J (2004) Increasing the packing of small aneurysms with soft coils: an in vitro study. Neuroradiology 46(11):935–939
Piotin M, Mandai S, Sugiu K, Gailloud P, Rüfenacht DA (2001) Endovascular treatment of cerebral aneurysms: an in vitro study with detachable platinum coils and tricellulose acetate polymer. AJR Am J Roentgenol 176(1):235–239
Schloesser PE, Pakbaz RS, Levy DI, Imbesi SG, Wong WH, Kerber CW (2007) Analysis of complex framing coil stability in a wide-necked aneurysm model. AJNR Am J Neuroradiol 28(2):387–389
Sorteberg A, Sorteberg W, Aagaard BDL, Rappe A, Strother CM (2004) Hemodynamic versus hydrodynamic effects of Guglielmi detachable coils on intra-aneurysmal pressure and flow at varying pulse rate and systemic pressure. AJNR Am J Neuroradiol 25(6):1049–1057
Standard S, Chavis T, Wakhloo AK, Ahuja A, Guterman LR, Hopkins LN (1994) Retrieval of a Guglielmi detachable coil after unraveling and fracture: case report and experimental results. Neurosurgery 35(5):994–999
Sugiu K, Martin JB, Jean B, Gailloud P, Mandai S, Rüfenacht DA (2003) Artificial cerebral aneurysm model for medical testing, training and research. Neurol Med Chir (Tokyo) 43(2):69–73
Sugiu K, Tokunaga K, Mandai S, Martin JB, Jean B, Rüfenacht DA (2003) Spiral versus J-shaped coils for neurovascular embolization-an in-vitro study. Neuroradiology 45(7):417–422
Sugiu K, Tokunaga K, Sasahara W, Watanabe K, Nishida A, Katsumata A, Kusaka N, Date I, Ohmoto T, Rüfenacht DA (2004) Training in neurovascular intervention. Usefulness of in-vitro model and clinical practice. Interv Neuroradiol 10(Suppl 1):107–112
Suzuki Y, Fujitsuka M, Chaloupka JC (2005) Simulation of endovascular neurointervention using silicone models: imaging and manipulation. Neurol Med Chir (Tokyo) 45(11):567–573
Tanaka N, Martin JB, Tokunaga K, Abe T, Uchiyama Y, Hayabuchi N, Berkefeld J, Rüfenacht DA (2004) Conformity of carotid stents with vascular anatomy: evaluation in carotid models. AJNR Am J Neuroradiol 25(4):604–607
Tateshima S, Tanishita K, Hakata Y, Tanoue SY, Viñuela F (2009) Alteration of intraaneurysmal hemodynamics by placement of a self-expandable stent. J Neurosurg 111(1):22–27
Tokunaga K, Tanaka N, Sugiu K, Levrier O, Martin JB, Rüfenacht DA (2002) Performance of long J-shaped coils in large and giant intracranial aneurysms: an in vitro study. Neuroradiology 44(3):261–267
Wakhloo AK, Gounis MJ (2008) Retrievable closed cell intracranial stent for foreign body and clot removal. Neurosurgery 62(5 Suppl 2):ONS390–ONS394
Watanabe K, Sugiu K, Tokunaga K, Sasahara W, Ono S, Date I (2007) Packing efficacy of hydrocoil embolic system: in vitro study using ruptured aneurysm model. Neurosurg Rev 30(2):127–130
Conflict of interest
The authors have no personal financial interest in any of the materials or devices described in this article.
Author information
Authors and Affiliations
Corresponding author
Additional information
Comments
Matthew Gounis, Worcester, USA
The article entitled “Silicone models as basic training and research aid in endovascular neurointervention—a single-center experience and review of the literature” by Srinivasan Paramasivam and colleagues describes the utility of silicone cerebrovascular replicas for training in endovascular techniques. Over the past decade, advances in 3D modeling and rapid prototyping have enabled a generation of anatomically accurate cerebrovascular models. This review is timely, as it emphasizes the need to develop solutions for comprehensive training as the dramatic increase in the availability of specialized interventional programs has subsequently decreased the volume available for endovascular training at academic medical centers [1]. The authors have trained an impressive 178 fellows in basic neurointerventional techniques using these silicone models. Moreover, the paper describes the necessity for advanced training of experienced interventionalists with new technology, namely, imaging systems and medical devices.
Numerous research studies that have advanced technology in neuroendovascular treatments using silicone vascular replicas are surveyed in this paper. The advantages of these models include reproducible engineering studies on hemodynamics and device characterization. Due to costs and societal sensitivities associated with animal experimentation, these models provide a viable alternative to address certain important questions in research of interventional neuroradiology. Researchers have seeded 3D vascular silicone models with endothelial cells [2], making a new generation of replicas that can serve as bioreactors. Yet other groups are working on new materials to generate vascular replicas that offer nearly identical tactile feedback with respect to the human cerebrovasculature. Advances in vascular replicas will continue to advance the discovery of improved technology for the treatment of cerebrovascular disease and offer enriching training programs for the foreseeable future.
Shahram Majidi, Washington, USA
This is an important study stressing the role of silicone models as a training aid in endovascular neurointerventional fellowship training. Paramasivam et al provided their experience in using silicone models as training tools in their endovascular neurointerventional fellowship program. The authors have more than 15 years of experience in training fellows in the field of endovascular surgical neurology and have trained more than 170 fellows. According to their experience, using silicone models has had significant impact on expanding fellows’ skills in handling and manipulating and navigating microcatheter and guidewire and also performing procedures such as coil embolization with or without stent assistance. As the authors nicely outlined, silicone models can be also used as valuable research tools. For instance, we can design and execute complex experiments investigating the hemodynamic changes within the aneurysm following stent deployment or compare different clot-retrieving devices in a safe in vitro setting without risk of harming the patient. These sorts of experiments are essential components of the field considering the fact that not all the hemodynamic and biophysical aspects of the devices are fully understood.
Current guidelines recommend minimum procedural volume requirements in order to reach acceptable operator experience and proficiency in performing endovascular procedures [3, 4]. For example, this number is 30 procedures for aneurysm coil embolization. There are very few teaching institutions in the USA which meet minimum requirements for all the procedures needed to reach adequate operator experience [5]. Therefore, it is essential to use adjunct training modalities such as silicone models or computer simulators in order to help the trainees obtain and maintain adequate procedural skills. Computer simulators have been used as a valuable adjunct training modality for endovascular procedure training with proven impact on trainees’ skill improvement [6]. Similarly, Dr. Paramasivam’s study is a successful example of necessity and value of using silicone models in neurointerventional fellowship training.
References
1. Cloft HJ. The neurointerventional bubble. AJNR Am J Neuroradiol. 2010;31:1162–1164.
2. Farcas MA, Rouleau L, Fraser R, Leask RL. The development of 3-D, in vitro, endothelial culture models for the study of coronary artery disease. Biomed Eng Online. 2009;8:30
3. Qureshi AI, Abou-Chebl A, Jovin TG. Qualification requirements for performing neurointerventional procedures: a Report of the Practice Guidelines Committee of the American Society of Neuroimaging and the Society of Vascular and Interventional Neurology. Journal of neuroimaging : official journal of the American Society of Neuroimaging. Oct 2008;18(4):433–447.
4. Connors JJ, 3rd, Sacks D, Furlan AJ, et al. Training, competency, and credentialing standards for diagnostic cervicocerebral angiography, carotid stenting, and cerebrovascular intervention: a joint statement from the American Academy of Neurology, the American Association of Neurological Surgeons, the American Society of Interventional and Therapeutic Neuroradiology, the American Society of Neuroradiology, the Congress of Neurological Surgeons, the AANS/CNS Cerebrovascular Section, and the Society of Interventional Radiology. Journal of vascular and interventional radiology : JVIR. Jul 2009;20(7 Suppl):S292–301.
5. Grigoryan M, Chaudhry SA, Hassan AE, Suri FK, Qureshi AI. Neurointerventional procedural volume per hospital in United States: implications for comprehensive stroke center designation. Stroke; a journal of cerebral circulation. May 2012;43(5):1309–1314.
6. Spiotta AM, Rasmussen PA, Masaryk TJ, Benzel EC, Schlenk R. Simulated diagnostic cerebral angiography in neurosurgical training: a pilot program. Journal of neurointerventional surgery. Jul 2013;5(4):376–381.
Rights and permissions
About this article
Cite this article
Paramasivam, S., Baltsavias, G., Psatha, E. et al. Silicone models as basic training and research aid in endovascular neurointervention—a single-center experience and review of the literature. Neurosurg Rev 37, 331–337 (2014). https://doi.org/10.1007/s10143-014-0518-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-014-0518-x