
Abstract
Introduction
While tight glucose control has been widely adopted in the critical care setting, the optimal target glucose level following acute traumatic brain injury (TBI) remains debatable. This observational study was conducted to delineate the relationship between glucose levels and clinical outcomes during acute phase (first 5 days) of TBI.
Methods
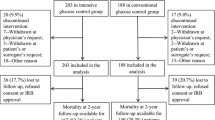
We retrospectively identified 429 TBI patients admitted to the intensive care unit (ICU) from January 2005 to December 2006. Of those, 380 patients were retained for final analysis. Collected data included demographics, admission Glasgow Coma Scale (GCS), and APACHE II, glucose on admission and during the first 5 days of admission, and insulin use. Clinical outcomes included mortality, ICU, and hospital length of stay.
Results
The overall hospital mortality was 13.2% (n = 50). Demographics were similar between survivor and nonsurvivor groups; however, nonsurvivors were older and had worse disease severity on admission. Nonsurvivors also had significantly higher glucose levels at admission and during the first 24 h of admission (P < 0.001). Based on the receiver operating characteristic (ROC) curve, admission and day-1 peak glucose were better predictors for mortality compared to hospital days 2–5 glucose levels, with day-1 peak glucose being the best predictor of mortality (AUC = 0.820). A Kaplan–Meier survival analysis also showed that patients with glucose <160 mg/dl during the first day of ICU admission had a significantly better survival rate compared to those with glucose ≥160 mg/dl (P < 0.001). Two glucose bands, <60 and ≥160 mg/dl, were identified to be associated with increased mortality irrespective of injury severity (OR = 1.130; 95% CI 1.034–1.235; P = 0.007; OR = 1.034; 95% CI 1.021–1.047, P < 0.001; respectively).
Conclusions
Findings from our study suggest a glucose level ≥160 mg/dl within the first 24 h of admission following TBI is associated with poor outcomes irrespective of severity of injury, and this presents a timeframe for which active therapeutic interventions may improve clinical outcomes. Prospective efficacy trials are needed to corroborate these findings.



Similar content being viewed by others

References
Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32(10):2426–32. doi:10.1161/hs1001.096194.
Young B, Ott L, Dempsey R, Haack D, Tibbs P. Relationship between admission hyperglycemia and neurologic outcome of severely brain-injured patients. Ann Surg. 1989;210(4):466–72. doi:10.1097/00000658-198910000-00007. discussion 472–3.
Lam AM, Winn HR, Cullen BF, Sundling N. Hyperglycemia and neurological outcome in patients with head injury. J Neurosurg. 1991;75(4):545–51.
Jeremitsky E, Omert L, Dunham CM, Protetch J, Rodriguez A. Harbingers of poor outcome the day after severe brain injury: hypothermia, hypoxia, and hypoperfusion. J Trauma. 2003;54(2):312–9. doi:10.1097/01.TA.0000037876.37236.D6.
Poungvarin N, Viriyavejakul A. Spontaneous supratentorial intracerebral haemorrhage: a prognostic study. J Med Assoc Thai. 1990;73(4):206–11.
Levetan CS. Effect of hyperglycemia on stroke outcomes. Endocr Pract. 2004;10(Suppl 2):34–9.
Lee TH, Ryu SJ, Chen ST. The prognostic value of blood glucose in patients with acute stroke. J Formos Med Assoc. 1991;90(5):465–70.
Jeremitsky E, Omert LA, Dunham CM, Wilberger J, Rodriguez A. The impact of hyperglycemia on patients with severe brain injury. J Trauma. 2005;58(1):47–50. doi:10.1097/01.TA.0000135158.42242.B1.
Margulies DR, Hiatt JR, Vinson D Jr, Shabot MM. Relationship of hyperglycemia and severity of illness to neurologic outcome in head injury patients. Am Surg. 1994;60(6):387–90.
Rovlias A, Kotsou S. The influence of hyperglycemia on neurological outcome in patients with severe head injury. Neurosurgery. 2000;46(2):335–42. doi:10.1097/00006123-200002000-00015. discussion 342–3.
Vespa P, Boonyaputthikul R, McArthur DL, et al. Intensive insulin therapy reduces microdialysis glucose values without altering glucose utilization or improving the lactate/pyruvate ratio after traumatic brain injury. Crit Care Med. 2006;34(3):850–6. doi:10.1097/01.CCM.0000201875.12245.6F.
Adams HP Jr, Adams RJ, Brott T, et al. Guidelines for the early management of patients with ischemic stroke: a scientific statement from the Stroke Council of the American Stroke Association. Stroke. 2003;34(4):1056–83. doi:10.1161/01.STR.0000064841.47697.22.
Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 2007;24(Suppl 1):S1–106. doi:10.1089/neu.2006.0209.
Broderick J, Connolly S, Feldmann E, et al. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38(6):2001–23. doi:10.1161/STROKEAHA.107.183689.
van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345(19):1359–67. doi:10.1056/NEJMoa011300.
Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008;358(2):125–39. doi:10.1056/NEJMoa070716.
Bergsneider M, Hovda DA, Shalmon E, et al. Cerebral hyperglycolysis following severe traumatic brain injury in humans: a positron emission tomography study. J Neurosurg. 1997;86(2):241–51.
Diringer MN. Is aggressive treatment of hyperglycemia for everyone? Crit Care Med. 2006;34(3):930–1. doi:10.1097/01.CCM.0000202433.99341.D6.
Strong AJ, Boutelle MG, Vespa PM, Bullock MR, Bhatia R, Hashemi P. Treatment of critical care patients with substantial acute ischemic or traumatic brain injury. Crit Care Med. 2005;33(9):2147–9. doi:10.1097/01.CCM.0000179029.95415.51. author reply 2149.
Vespa PM, McArthur D, O’Phelan K, et al. Persistently low extracellular glucose correlates with poor outcome 6 months after human traumatic brain injury despite a lack of increased lactate: a microdialysis study. J Cereb Blood Flow Metab. 2003;23(7):865–77. doi:10.1097/01.WCB.0000076701.45782.EF.
Oddo M, Schmidt JM, Mayer SA, Chiolero RL. Glucose control after severe brain injury. Curr Opin Clin Nutr Metab Care. 2008;11(2):134–9. doi:10.1097/MCO.0b013e3282f37b43.
Welsh FA, Ginsberg MD, Rieder W, Budd WW. Deleterious effect of glucose pretreatment on recovery from diffuse cerebral ischemia in the cat. II. Regional metabolite levels. Stroke. 1980;11(4):355–63.
Zygun DA, Steiner LA, Johnston AJ, et al. Hyperglycemia and brain tissue pH after traumatic brain injury. Neurosurgery. 2004;55(4):877–81. doi:10.1227/01.NEU.0000137658.14906.E4. discussion 882.
Godoy DA, Pinero GR, Svampa S, Papa F, Di Napoli M. Hyperglycemia and short-term outcome in patients with spontaneous intracerebral hemorrhage. Neurocrit Care. 2008;9(2):217–29. doi:10.1007/s12028-008-9063-1.
Abi-Saab WM, Maggs DG, Jones T, et al. Striking differences in glucose and lactate levels between brain extracellular fluid and plasma in conscious human subjects: effects of hyperglycemia and hypoglycemia. J Cereb Blood Flow Metab. 2002;22(3):271–9. doi:10.1097/00004647-200203000-00004.
Hopwood SE, Parkin MC, Bezzina EL, Boutelle MG, Strong AJ. Transient changes in cortical glucose and lactate levels associated with peri-infarct depolarisations, studied with rapid-sampling microdialysis. J Cereb Blood Flow Metab. 2005;25(3):391–401. doi:10.1038/sj.jcbfm.9600050.
Parkin M, Hopwood S, Jones DA, et al. Dynamic changes in brain glucose and lactate in pericontusional areas of the human cerebral cortex, monitored with rapid sampling on-line microdialysis: relationship with depolarisation-like events. J Cereb Blood Flow Metab. 2005;25(3):402–13. doi:10.1038/sj.jcbfm.9600051.
Acknowledgments
We would like to thank Al Jephson for his help with data extraction and Dr. Andrew DeRyke for his critical review of the manuscript.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Liu-DeRyke, X., Collingridge, D.S., Orme, J. et al. Clinical Impact of Early Hyperglycemia During Acute Phase of Traumatic Brain Injury. Neurocrit Care 11, 151–157 (2009). https://doi.org/10.1007/s12028-009-9228-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-009-9228-6