
Abstract
Introduction
Juvenile nasopharyngeal angiofibroma (JNA) is a rare, nonencapsulated, benign neoplasm typically diagnosed in adolescent boys. Surgery is the usual treatment modality for JNA. The optimal surgical procedure should allow maximal exposure of the tumor for complete excision with minimum morbidity. One possible surgical approach is Le Fort I maxillary osteotomy. The aim of this study was to review our experience with the Le Fort I osteotomy and to investigate the feasibility of this approach for extensive JNA invaded into pterygopalatine and infratemporal fossae.
Methods
We retrospectively studied patients who had undergone JNA resection via the Le Fort I osteotomy approach from July 2000 to September 2007, considering tumor location and size, complications, and tumor recurrence associated with the surgical approach.
Results
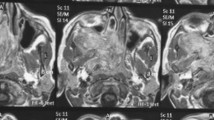
Six patients of JNA (all boys; mean age, 15.5 years) were identified through the chart review. All the angiofibromas had extended into the pterygomaxillary space and infratemporal fossa. The mean follow-up for this cohort was 50.1 months. No intraoperative and postoperative complications were noted, except for slight diplopia in one patient due to injury of the left medial rectus muscle. There were no cases of tumor recurrence that could be attributed to the procedure.
Conclusion
Our experience suggests that the Le Fort I osteotomy approach is a useful technique for the removal of extensive JNA invaded into pterygopalatine and infratemporal fossae. It has distinct advantages over traditional anterior or lateral approaches, providing a more direct vision, improved exposure, and cosmesis.
Similar content being viewed by others


References
Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM. Diagnosis and treatment of juvenile nasopharyngeal angiofibroma. Eur Arch Otorhinolaryngol. 2001;258:120–124.
Juvenile Nasopharyngeal Angiofibroma. eMedicine web site. Available at: www. emedicine.com/ent/topic470.htm. Accessed September 11, 2008.
Moloney F, Worthington P. The origin of the Le Fort I maxillary osteotomy: Cheever’s operation. J Oral Surg. 1981;39:731–734.
Yiotakis I, Eleftheriadou A, Davilis D, et al. Juvenile nasopharyngeal angiofibroma stages I and II: a comparative study of surgical approaches. Int J Pediatr Otorhinolaryngol. 2008;72:793–800.
Fisch U. The infratemporal fossa approach for nasopharyngeal tumors. Laryngoscope. 1983;93:36–44.
Lee JT, Chen P, Safa A, Juillard G, Calcaterra TC. The role of radiation in the treatment of advanced juvenile angiofibroma. Laryngoscope. 2002;112:1213–1220.
Goepfert H, Cangir A, Lee YY. Chemotherapy for aggressive juvenile nasopharyngeal angiofibroma. Arch Otolaryngol. 1985;111:285–289.
Sasaki CT, Lowlicht RA, Tokashiki R. Horizontal maxillotomy for exposure of the central skull base: the Yale experience. J Neurooncol. 2001;55:173–177.
Roger G, Tran Ba Huy P, Froehlich P, et al. Exclusively endoscopic removal of juvenile nasopharyngeal angiofibroma: trends and limits. Arch Otolaryngol Head Neck Surg. 2002;128:928–935.
Colreavy MP, Baker T, Campbell M, Murphy M, Lyons B. The safety and effectiveness of the Le Fort I approach to removing central skull base lesions. Ear Nose Throat J. 2001;80:315–318.
Lewark TM, Allen GC, Chowdhury K, Chan KH. Le Fort I osteotomy and skull base tumors: a pediatric experience. Arch Otolaryngol Head Neck Surg. 2000;126:1004–1008.
Roy S, Patel PK, Tomita T. The Le Fort I transmaxillary approach to skull base tumors. Clin Plast Surg. 2007;34.575–583.
Hoffman GR, Islam S. The difficult Le Fort I osteotomy and downfracture: a review with consideration given to an atypical maxillary morphology. J Plast Reconstr Aesthet Surg. 2008;61:1029–1033.
Lo LJ, Hung KF, Chen YR. Blindness as a complication of Le Fort I osteotomy for maxillary distraction. Plast Reconstr Surg. 2002;109:688–698.
Lanigan DT, West RA. Management of postoperative hemorrhage following the Le Fort I maxillary osteotomy. J Oral Maxillofac Surg. 1984;42:367–375.
Stringer DE, Dolwick MF, Steed DL. Subcutaneous emphysema after Le Fort I osteotomy: report of two cases. J Oral Surg. 1979;37:115–116.
Lowlicht RA, Jassin B, Kim M, Sasaki CT. Long-term effects of Le Fort I osteotomy for resection of juvenile nasopharyngeal angiofibroma on maxillary growth and dental sensation. Arch Otolaryngol Head Neck Surg. 2002;128:923–927.
Cruz AA, Atique JM, Melo-Filho FV, Elias J Jr. Orbital involvement in juvenile nasopharyngeal angiofibroma: prevalence and treatment. Ophthal Plast Reconstr Surg. 2004;20:296–300.
Okada Y. Evaluation of the process of recovery of dental pulp after Le Fort I osteotomy [in Japanese]. Kokubyo Gakkai Zasshi. 2001;68:39–50.
Watts PG. Unilateral abducent nerve palsy: a rare complication following a Le Fort I maxillary osteotomy. Br J Oral Maxillofac Surg. 1984;22:212–215.
Lanigan DT, Hey JH, West RA. Aseptic necrosis following maxillary osteotomies: report of 36 cases. J Oral Maxillofac Surg. 1990;48:142–156.
Herman P, Lot G, Chapot R, Salvan D, Huy PT. Long-term follow-up of juvenile nasopharyngeal angiofibromas: analysis of recurrences. Laryngoscope. 1999;109:140–147.
de Mello-Filho FV, De Freitas LC, Dos Santos AC, Martins Mamede RC. Resection of juvenile angiofibroma using the Le Fort I approach. Am J Otolaryngol. 2004;25: 157–161.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Lin, Y., Qiu, JH., Qiao, L. et al. Le Fort I osteotomy for extensive juvenile nasopharyngeal angiofibroma: a retrospective study. Adv Therapy 25, 1057–1064 (2008). https://doi.org/10.1007/s12325-008-0104-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12325-008-0104-0