
Abstract
This article reports on preliminary findings describing microstructural abnormalities in the white matter of cortical areas thought to be associated with bipolar disorder. In all, 14 patients with bipolar disorder and 21 nonpsychiatrically ill control subjects underwent MR imaging including a diffusion tensor imaging (DTI) pulse sequence (six directions, b=1000 mm2/s). DTI data were analyzed on a workstation using a program that allowed calculation of apparent diffusion coefficient (ADC) and fractional anisotropy (FA) within the following three white matter fiber tracts bilaterally: the orbital frontal cortex, and the superior and middle frontal gyri. These values were compared across patient groups. The left and right orbital frontal white matter exhibited significantly higher ADC values in bipolar subjects than control subjects on both the left (p=0.028) and right (p=0.011). Microstructural changes in the white matter of the orbital frontal areas as reflected by increased ADC values appear to be associated with bipolar disorder. Further research is needed to better understand the interaction of microstructural changes and bipolar symptoms and whether these changes are specific to bipolar disorder.
Similar content being viewed by others

INTRODUCTION
Mayberg (1997) proposed that three brain systems comprise the neurological substrate of mood disorders: (1) a dorsal attention-cognitive system composed of prefrontal cortex (PFC) (Brodmann areas, BA 9/46, 44), the anterior cingulate (BA 24), and inferior parietal (BA 40) areas, (2) a ventral vegetative-somatic system composed of ventral frontal (BA 47) cortex, the amygdala, hippocampus, subgenual cingulate (BA 25), and ventral insula, and (3) a rostral cingulate region (BA 24) that integrates the dorsal and ventral systems.
Mayberg (1997) hypothesized that a reciprocal relationship between the dorsal and ventral system regulates mood. We were interested in evaluating whether the connectivity between these regions may be impaired in mood disorders. We used diffusion tensor imaging (DTI) to evaluate this connectivity. DTI imaging provides sensitivity to the microscopic motions of water in tissue in a selected direction and, consequently, the microcellular environment in the tissue through the application of diffusion-sensitizing gradients in the selected direction. DTI allows measurement of rate of microscopic water diffusion (as reflected in the apparent diffusion coefficient, or ADC) and directionality of water diffusion (as reflected in anisotropy values, or tendency for water to diffuse in one direction as opposed to all other directions). Anisotropy is standardly measured using indices such as fractional anisotropy (FA) values and relative anisotropy values.
Using such images, the tissue ADC can be calculated. The term ‘ADC’ is used to indicate that the result is an average over the various tissue compartments in an image voxel. This imaging method is well established to be exquisitely sensitive to ischemic damage in tissue (Gray and MacFall, 1998; Taylor et al, 2004a) and thus is likely to provide similar information in tissue affected by lesions.
In general, microscopic water diffusion can be characterized as a tensor (rather than scalar or vector) quantity. The minimal number of diffusion encoding directions needed to describe such a tensor quality is six directions (Basser and Pierpaoli, 1996). The degree to which these coefficients differ in a voxel (the degree of anisotropy) is a measure of the tissue structure. Normal white matter tracts exhibit strong anisotropy, while normal gray matter is isotropic. There is some early evidence that anisotropy is decreased in white matter pathways in Alzheimer's disease (Hanyu et al, 1998), depression (Taylor et al, 2004b), and schizophrenia (Buchsbaum et al, 1998), presumably due to degeneration. This study reports on preliminary findings looking at the microstructural integrity of white matter tracts in bipolar patients.
We hypothesized that bipolar subjects would exhibit greater microstructural abnormalities (represented by increased diffusivity, or higher apparent ADC values) and decreased anisotropy values in the tracts connecting critical regions thought to be involved in mood regulation of bipolar disorder. Based on Mayberg's hypothesis, the regions on which we selected to focus were the orbital frontal and prefrontal areas.
METHOD
Subjects
All subjects were participants in the NIMH-sponsored cross-sectional study for Late-life Bipolar Disorder. Participants were recruited from the psychiatric units at Duke University Medical Center and John Umstead Hospital, as well as community-dwelling subjects with a history of bipolar disorder. All subjects completed a SCID interview and met diagnostic criteria for Bipolar Disorder as defined by the DSM IV diagnostic criteria. Patients were excluded if they had evidence of dementia (as suggested by seven or more errors on the Mini-Mental Status Examination (MMSE)), other primary psychiatric diagnosis, neurological or medical illnesses that contributed to the diagnosis, or a recent history of substance abuse. Control subjects were recruited by advertisement and had no active psychiatric illness. The study was approved by the Institutional Review Boards of both institutions.
The sample included 14 subjects and 21 controls. Demographic information of the samples is listed in Table 1. There were no significant differences in age, gender, marital status, or education between the controls and bipolar subjects. There was a significant difference in race, with controls having more non-Caucasians (p=0.02). Of the 14 bipolar subjects, six were currently in a depressive state, five were in a manic/hypomanic state, and three were euthymic at the time of the study. The mean length of illness (measured from the first affective episode) was 13.6 years (±12.1 years) with a range of 1–34 years. There was a wide variability in the number of recurrences with 12 (85%) reporting a history of more than three manic episodes in the past (range 1 → 100).
It should be noted that the orbital frontal cortex (OFC) was able to be viewed in only 12 bipolar subjects and 18 controls because of susceptibility artifact. This artifact usually occurs when the MRI signal is poorly transmitted due to soft tissue structures being located close to the air–brain interfaces, such as that seen in the frontal sinus.
Neuroimaging
Subjects were screened for implanted metal in their body or other contraindications to MRI. Axial images were acquired with a Signa 1.5 MR system (GE Healthcare, Milwaukee, WI) using the standard head (volumetric) radiofrequency coil. The scanner alignment light was used to adjust the head tilt and rotation so that the axial plane lights passed across the cantomeatal line and then sagittal lights were aligned with the center of the nose. A rapid sagittal localizer scan confirmed the alignment. The head position was adjusted and padded to minimized head rotation about the S–I axis. The subject's rotation around the L–R axis was allowed to vary slightly according to the subject's habitus in order to minimize discomfort and the resultant motion artifacts. After localization of slices to be imaged, the automated manufacturer algorithm adjusted the shim currents to obtain good magnetic field uniformity.
The diffusion images were acquired using a 2D echo-planar pulse sequence (TE=109 ms and TR=12 000 ms), acquiring an image in each of six diffusion weighting directions with a b value of 1000s/mm2 as well as one additional image with b=0. The direction scheme followed that of Basser and Pierpaoli (1998). The other parameters for the sequence were as follows: field of view=24 cm × 24 cm; 90 kHz bandwidth, 1 excitation; 128 × 128 matrix; 5 mm slice thickness; and slice gap=2.5 mm. Image processing was performed in the Neuropsychiatric Imaging Research Laboratory at Duke University Medical Center. Diffusion-weighted images were processed using custom MATLAB (Mathworks, Natick, MA) scripts, which calculated (Basser and Pierpaoli, 1996; Conturo et al, 1996) the diffusion tensor eigenvalues in each voxel. ADC maps and diffusion FA maps (Basser and Pierpaoli, 1996) were then calculated.
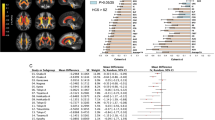
ADC and FA images were processed on SUN workstations using Analyze 4.0 (Mayo Clinic, Rochester, MN). Scans were examined in a random order by a reader (JLB) blinded to bipolar status. The reader placed regions of interest (ROIs) with defined shapes and volumes to avoid gray matter bilaterally in the white matter of the superior and middle frontal gyri, and the medial orbital frontal gyri (see Figure 1). By protocol, all ROIs were placed irrespective of white matter lesions; however, no white matter lesions were located in the ROIs on the interpreted scans.

Placement of ROIs: (a) Orbital frontal tracts and (b) medial and superior prefrontal gyri.
The prefrontal and orbitofrontal sites were selected based on evidence from Mayberg (1997) and others suggesting anatomical connections involved in a ‘mood regulation circuit’. The OFC ROIs were placed on the most superior slice in which the CSF of the olfactory sulcus was at least half of the anterior to posterior length of the OFC. Each ROI was placed medial to the olfactory sulcus bilaterally. Locations of the ROI placements for the dorsolateral PFC were standardized using criteria reported in Taylor et al (2004b). The prefrontal gyri ROIs were placed on the superior and middle frontal gyri bilaterally on the most caudad slice in which both gyri were visible as separate structures and halfway between the anterior boundary (frontal pole of the brain) and the posterior boundary (the precentral sulcus).
The size of ROIs for the OFC and the middle and superior frontal gyri was 49.59 mm2.
Reliability was established by repeated measurements on multiple resonance DTI scans. Intraclass correlational coefficients (ICCs) attained were as follows: left superior frontal gyrus, ICC=0.96; right superior frontal gyrus, ICC=0.92; left middle frontal gyrus, ICC=0.97; right middle frontal gyrus, ICC=0.77; left orbital frontal gyrus, ICC=0.72; and right orbital frontal gyrus, ICC=0.76.
Statistical Analysis
Descriptive statistics, means, SDs, and percentages were used for continuous variables and categorical variables, respectively. Nonparametric, Wilcoxon's tests were used to determine differences between the subject and control groups on values of ADC, FA, and RA values for each region. Generalized linear model (GLM) was used to examine the age-adjusted groups differences.
RESULTS
Bipolar subjects exhibited higher ADC values in all ROI; however, this was only statistically significant in both OFCs (left OFC, p=0.028; right OFC, p=0.011) (Table 2).
In the FA analyses, bipolar subjects had lower FA values than controls in all ROIs (except in the FA measurement for the left OFC), although these differences did not reach statistical significance (Tables 3).
Using GLM to control for age, the difference in diffusivity of the OFC in bipolar subjects compared with controls continued to demonstrate significance (left OFC, p=0.0092; right OFC, p=0.0204).
DISCUSSION
This study reports on preliminary findings that individuals with bipolar disorder exhibit higher ADC values in the white matter of the left and right orbital frontal gyri than nonpsychiatrically ill controls. This finding did not extend to measures of FA in the same regions. ADC values represent an indication of diffusivity of water molecules without providing an indication of water diffusion directionality. FA values provide both a measurement of both diffusivity and directionality, and are thought to represent the directionality imposed by both degree of myelination and integrity of the axons (Guo et al, 2002). Our findings may represent increases in the amount of intracellular water without changes in myelin composition or disruption of axonal pathways sufficient to produce substantial changes in FA values.
Studies have shown that the OFC is involved in modulating emotional behavior and stress response (Drevets, 2000). Orbital frontal volumetric abnormalities have been described in unipolar depressed patients (Lai et al, 2000; Bremner et al, 2002; Lee et al, 2003). Reports of volumetric analysis of the PFC are relatively limited in bipolar subjects. Drevets et al (1997) have demonstrated reduction in the gray volume of the PFC. In bipolar patients, functional neuroimaging has demonstrated decreased orbital frontal activity at rest compared with controls (Blumberg et al, 1999).
Abnormalities of function and structure in the limbic-thalamic-cortical circuits (including amygdala, medial thalamus, and orbital and medial PFC, and limbic-cortical-striatopallidal-thalamic circuits) have been implicated in mood disorders (Drevets, 2000). Our findings support the theory that microstructural changes in white matter may result in disconnection of cortical and subcortical regions. Changes in ADC are sensitive measures of white matter injury. Changes that disrupt the tracts connecting critical regions involved in mood regulation may contribute to the pathogenesis of bipolar disorder.
Adler et al (2004) conducted a DTI study in bipolar patients focusing on prefrontal regions. They evaluated samplings of the white matter tracts extending above the anterior commissure, of which the most superior were located near our sampling for the SFGs. They found a reduction of FA in the prefrontal area, more prominently noted in the most superior slices, suggesting a loss of coherence in the white matter tracts in this area. Although their study cannot be directly compared with ours due to differences in technique, ROI placement, and subject samples, we did not find FA changes in similar regions between our bipolar subjects and control group for this region. However, both studies do support the possibility that a loss of mood circuit connectivity may be a mechanism involved in bipolar symptomatology.
It should be noted that although the findings were significant for the ADC measurement, FA measurements were not significantly different between the two subject groups. We believe that this is due to the small sample size. ADC measurement assesses rate of microscopic water diffusion, while FA values assess anisotropy, or directionality diffusion. A larger sample size may better elucidate the relationship of white matter changes in the OFC.
There are several potential limitations in our study. The main limitation is the lack of specificity of our findings. Not all fibers within the white matter tracts of the orbital frontal region are involved in mood regulation circuits, nor are they all following parallel lines in a plane. This limitation would be true for the other sites that we sampled as well. The exact determination of the fraction of white matter that comprises mood regulation circuits must await more specific forms of analysis, such as fiber tractography, which was not available to us at the time of this study. In future studies, we will attempt to use tractography to better define pathways relevant to our hypothesis.
As noted in the Results section, in five of the 31 scans, the OFC could not be measured due to the susceptibility artifact. This factor may also have biased our results, although the incidence of the artifact was spread evenly between subjects and controls. In future studies, this factor could be minimized by the use of parallel imaging techniques that were not available to us at the time of this study and which diminish susceptibility effects. Further, the relatively large slice thickness may allow measurement of diffusivity to be confounded by variability of individual brain shape and size. While we attempted to minimize this in our selection of ROI size and shape, future research efforts will need to use thinner slices, which would more effectively minimize this potential confound.
Although age was controlled in our analyses, the broad range of the subject ages must be controlled in future studies. Findings of potential significance in this preliminary study are an encouragement to look at a sample with a more narrow range of ages. The difference in the racial make up of the control and subject groups is not believed to be significant since other demographic factors are similar. However, potentially more important are factors that many affect neural connectivity that may vary among the bipolar subject group. These may include length of illness, age of onset, number of recurrences, phase of episode at time of the study, medication exposure, family psychiatric history, and medical illnesses. Our analyses were not powered to measure the effect of these, but future studies with larger numbers of subjects may control for these factors. Similarly, because our data are presented as preliminary findings, statistical corrections for multiple measurements were not made, which could effect the significance of the findings.
Further research is needed to continue to define the neuroanatomy of bipolar disorder, improved DTI-based fiber tractography, and the relationship of changes in severity of illness, treatment response, and relapse. The results of future studies along these lines may provide information that will elucidate disruption of pathways important in mood that will help in the assessment of prognosis and focus more specific treatments for bipolar disorder.
References
Adler CM, Holland SK, Schmithorst V, Wilke M, Weiss KL, Pan H et al (2004). Abnormal frontal white matter tracts in bipolar disorder: a diffusion tensor imaging study. Bipolar Disorders 6: 197–203.
Basser PJ, Pierpaoli C (1996). Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. J Magn Reson B 111: 209–219.
Basser PJ, Pierpaoli C (1998). A simplified method to measure the diffusion tensor from seven MR images. Magn Reson Med 39: 928–934.
Blumberg HP, Stern E, Ricketts S, Martinez D, de Asis J, White T et al (1999). Rostral and orbital prefrontal cortex dysfunction in the manic state of bipolar disorder. Am J Psychiatry 156: 1986–1988.
Bremner JD, Vythilingam M, Vermetten E, Nazeer A, Adil J, Khan S et al (2002). Reduced volume of orbitofrontal cortex in major depression. Biol Psychiatry 51: 273–379.
Buchsbaum MS, Tang CY, Peled S, Gudbjartsson H, Lu D, Hazlett EA et al (1998). MRI white matter diffusion anisotropy and PET metabolic rate in schizophrenia. Neuroreport 9: 425–430.
Conturo TE, McKinstry RC, Akbudak E, Robinson BH (1996). Encoding of anisotropic diffusion with tetrahedral gradients: a general mathematical diffusion formalism and experimental results. Magn Reson Med 35: 399–412.
Drevets WC (2000). Neuroimaging studies of mood disorders. Biol Psychiatry 48: 813–829.
Drevets WC, Price JD, Simpson JR, Todd RD, Reich T, Vannier M et al (1997). Subgenual prefrontal cortex abnormalities in mood disorders. Nature 386: 824–827.
Gray L, MacFall J (1998). Overview of diffusion imaging. MRI Clin N Am 6: 125–138.
Guo AC, MacFall JR, Provenzale JM (2002). Diffusion tensor imaging of multiple sclerosis: evaluation of normal-appearing white matter. Radiology 222: 729–736.
Hanyu H, Sakurai H, Iwamoto T, Takasaki M, Shindo H, Abe K (1998). Diffusion-weighted MR imaging of the hippocampus and temporal white matter in Alzheimer's disease. J Neurological Sci 156: 195–200.
Lai TJ, Payne ME, Byrum CE, Steffens DC, Krishnan KRR (2000). Reduction in orbital frontal cortex in geriatric depression. Biol Psychiatry 48: 971–975.
Lee SH, Payne ME, Steffens DC, McQuoid DR, Lai TJ, Provenzale JM et al (2003). Subcortical lesion severity and orbitofrontal cortex volume in geriatric depression. Biol Psychiatry 54: 529–533.
Mayberg HS (1997). Limbic-cortical dysregulation: a proposed model of depression. J Neuropsychiatry Clin Neurosci 9: 471–481.
Taylor WD, Hsu E, Krishnan KR, MacFall JR (2004a). Diffusion tensor imaging: background, potential, and utility in psychiatric research. Biol Psychiatry 55: 201–207.
Taylor WD, MacFall JR, Payne ME, McQuoid DR, Provenzale JM, Steffens DC et al (2004b). Late-life depression and abnormalities in dorsolateral prefrontal cortex white matter microstructure. Am J Psychiatry 161: 1293–1296.
Acknowledgements
This study was supported by a NARSAD Young Investigator Award and NIMH Grant #5ROI-MH57027. We would like to acknowledge the image processing assistance of Mr Brian Boyd and Ms Cynthia Key of the Department of Psychiatry and Behavioral Sciences at Duke University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Beyer, J., Taylor, W., MacFall, J. et al. Cortical White Matter Microstructural Abnormalities in Bipolar Disorder. Neuropsychopharmacol 30, 2225–2229 (2005). https://doi.org/10.1038/sj.npp.1300802
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.npp.1300802
Keywords
This article is cited by
-
Analysis of Bipolar Disorder Using fMRI
Wireless Personal Communications (2023)
-
Differences in attentional control and white matter microstructure in adolescents with attentional, affective, and behavioral disorders
Brain Imaging and Behavior (2020)
-
A Critical Review on Structural Neuroimaging Studies in BD: a Transdiagnostic Perspective from Psychosis to Fronto-Temporal Dementia
Current Behavioral Neuroscience Reports (2020)
-
Structural dysconnectivity of key cognitive and emotional hubs in young people at high genetic risk for bipolar disorder
Molecular Psychiatry (2018)
-
Myelin vs Axon Abnormalities in White Matter in Bipolar Disorder
Neuropsychopharmacology (2015)
