
Abstract
The eye is involved in several pathologies where precise identification of the underlying condition is essential for the optimal patient care. This preliminary report presents the potential of high-resolution microscopy coil magnetic resonance imaging (HR-MRI) to undertake this task being actively used in the clinical setting. We used a commercially available MRI scanner and a microscopy surface coil. Exquisite anatomic detail of the eye and orbit with depiction of previously unobserved structures and clear demonstration of the underlying pathology was achieved. This report supports the idea that orbital imaging can be revolutionized with the introduction of HR-MRI with broad clinical implications.
Similar content being viewed by others

Introduction
High-resolution microscopy coil magnetic resonance imaging (HR-MRI) is a novel valuable tool in the field of medical imaging which has even managed to change longstanding beliefs on the pathophysiology of well-studied disorders.1 It is noninvasive and allows thinner sections with higher spatial resolution. The eye is an ideal organ for HR-MRI because of its wide variation in water content and especially because of the requirement of high spatial resolution in a small field of view with multiple tissue diversity. This preliminary report aims to provide insight on the technique and its potential as a new imaging modality.
Materials and methods
MR images were acquired using a 1.5 T Gyroscan ACS-NT scanner (Philips Medical Systems, Best, The Netherlands). Subjects with normal eyes and vision, and normal eye movements were imaged in the supine position using a Philips surface ‘microscopy coil’ of 47 mm inner diameter placed in front of the eye scanned. The examination protocol included T1- and T2-weighted spin-echo images in all three planes (axial, coronal, and sagittal). The T1- weighted images had repetition time (TR) and echo time (TE) values of 475 and 18 ms, respectively, whereas T2-weighted images were acquired with a TR value of 3500 and a TE of 100 ms. The imaging sequences employed a field of view of 80 mm and a data acquisition matrix of 256 × 224 with 512 × 512 Fourier-transformed data points. The slice thickness was 2 mm and the interslice gap was 0.2 mm. Fat suppression techniques spectral saturation inversion recovery (SPIR) and short tau inversion recovery (STIR) were also performed. Acquisition times and total scanning time were similar to those of conventional head coil orbital MRI.
Results
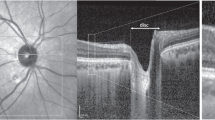
Exquisite anatomic detail previously unobserved in MRI is revealed. The tarsal plate, ciliary body, zonules of the lens, layers of anterior and posterior globe are clearly depicted (Figure 1). The extraocular muscles, optic nerve together with its sheath, as well as the retrobulbar fat and parts of its connective tissue are visualised in high detail (Figures 1, 2 and 3). The separation of superior muscle group into its components, previously unobserved with conventional head coil orbital MRI, is accomplished (Figure 3). The structure of the tarsal plate and Tenon's capsule are outlined for the first time with MRI in such a detailed manner. Furthermore, pathologies including inflammatory eye disease and its complications can be depicted with the use of this technique (Figure 4).

Axial T1-weighted HR-MR images. (a) Exquisite anatomic detail of the eye and orbital cavity. Red arrows indicate the Tenon's capsule, yellow arrowhead points at the iris and green arrowhead points at pupil (LG: lacrimal gland). (b) Tarsal plate is shown (blue arrows).

Axial T2-weighted HR-MR image. The optic nerve and its sheath are demonstrated.

Coronal T1-weighted HR-MR image. The superior rectus is clearly separated and distinguished from the levator palpebrae superioris and the outline of the other extraocular muscles is precisely defined.

Axial T1-weighted HR-MR image with fat suppression and contrast enhancement in multifocal choroiditis. Attenuation of the normal enhancement of the choroido-retinal layer at the posterior pole is observed with thickening on the lateral aspect (red arrows). These findings correlated well with choroiditis and a macular scar in the left fovea.
Discussion
This study demonstrates the great potential that HR-microscopy coil MRI has in both depicting normal anatomy and subtle pathologic changes. HR-MRI shares all the advantages of conventional MRI over CT including the absence of ionising radiation, capability of multiplanar image acquisition and the absence of dental and bony artefacts. Furthermore, it offers superior tissue contrast to both conventional MRI and CT and focuses on the tissue of interest with regard to orbital imaging. Surface coils of various configurations and sizes have been used in the past.2, 3, 4, 5, 6, 7 However, to the best of our knowledge, this is the first report on HR-MRI presenting such a detailed depiction of orbital structures with special reference to globe layers, Tenon's capsule and tarsal plates. The advantages of this technique, in particular, are that it does not require customised coils or long and elaborate acquisition procedures. Furthermore, from our experience it seems that it is well tolerated by patients. The limitation of this technique was a slight and gradual decrease of signal intensity with increasing distances from the coil. This was inevitably encountered as it is an inherent disadvantage of surface coil imaging. However, by using coil uniformity correction methods like CLEAR (constant level appearance) of the Philips systems, more uniform signal intensity can be achieved.
This study supports the idea that microscopy coils should be introduced into orbital imaging and further research is required to establish a robust imaging technique for the optimal visualisation of eye and orbital cavity. Lessons learned from other specialties on the use of HR-MRI can and should be applied in the everyday ophthalmologic practice.1
Conclusion
Obtaining HR-MR images from clinically available scanners represents a novel way of exploring the anatomy and pathological changes in the eye and orbit. Our results illustrate that the use of this microscopy surface coil improves dramatically the image resolution and consequently both the diagnostic accuracy and surgical planning.
References
Tan AL, Grainger AJ, Tanner SF, Shelley DM, Pease C, Emery P et al. High-resolution magnetic resonance imaging for the assessment of hand osteoarthritis. Arthritis Rheum 2005; 52(8): 2355–2365.
Bilaniuk LT, Schenck JF, Zimmerman RA, Hart Jr HR, Foster TH, Edelstein WA et al. Ocular and orbital lesions: surface coil MR imaging. Radiology 1985; 156(3): 669–674.
Atlas SW, Bilaniuk LT, Zimmerman RA, Hackney DB, Goldberg HI, Grossman RI . Orbit: initial experience with surface coil spin-echo MR imaging at 1.5 T. Radiology 1987; 164(2): 501–509.
Ohnishi T, Noguchi S, Murakami N, Tajiri J, Harao M, Kawamoto H et al. Extraocular muscles in Graves ophthalmopathy: usefulness of T2 relaxation time measurements. Radiology 1994; 190(3): 857–862.
Strenk SA, Semmlow JL, Strenk LM, Munoz P, Gronlund-Jacob J, DeMarco JK . Age-related changes in human ciliary muscle and lens: a magnetic resonance imaging study. Invest Ophthalmol Vis Sci 1999; 40(6): 1162–1169.
Ettl A, Zwrtek K, Daxer A, Salomonowitz E . Anatomy of the orbital apex and cavernous sinus on high-resolution magnetic resonance images. Surv Ophthalmol 2000; 44(4): 303–323.
Lemke AJ, Hosten N, Wiegel T, Prinz RD, Richter M, Bechrakis NE et al. Intraocular metastases: differential diagnosis from uveal melanomas with high-resolution MRI using a surface coil. Eur Radiol 2001; 11(12): 2593–2601.
Author information
Authors and Affiliations
Corresponding author
Additional information
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Work Attributed to: Eye Department, School of Medicine, University of Leeds
Rights and permissions
About this article
Cite this article
Georgouli, T., James, T., Tanner, S. et al. High-Resolution Microscopy Coil MR-Eye. Eye 22, 994–996 (2008). https://doi.org/10.1038/sj.eye.6702755
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702755
Keywords
This article is cited by
-
3T high-resolution magnetic resonance imaging, conventional ultrasonography and ultrasound biomicroscopy of the normal canine eye
BMC Veterinary Research (2022)
-
Uveal melanoma: evaluation of extrascleral extension using thin-section MR of the eye with surface coils
La radiologia medica (2014)
-
Retrobulbar vasculature using 7-T magnetic resonance imaging with dedicated eye surface coil
Graefe's Archive for Clinical and Experimental Ophthalmology (2013)
-
Orbita – Anatomie, Entwicklung und Fehlbildungen
Der Radiologe (2008)
