Article Text

Abstract
Background The Society of Neurointerventional Surgery revised its operational definition of emergent large vessel occlusion (ELVO) recently to include proximal M2 segment middle cerebral artery (MCA) occlusions. We sought to assess the benefit of endovascular thrombectomy (EVT) over best medical care for M2 segment MCA occlusion.
Methods Patient level data from trials in the HERMES Collaboration were included. The HERMES core laboratory identified patients with M2 segment MCA occlusions and further classified them as proximal versus distal, anterior versus posterior division, and dominant versus co-dominant versus non-dominant. Primary outcome was modified Rankin Scale (mRS) score 0–2 at 90 days. Secondary outcomes were modified Thrombolysis in Cerebral Infarction (mTICI) rates at end of procedure, 90-day mRS shift, 90-day mRS 0–1, 24 hours National Institute of Health Stroke Scale (NIHSS) score 0–2, symptomatic intracerebral hemorrhage (ICH), and death.
Results 130 patients with M2 MCA (proximal location n=116 vs distal n=14, anterior division n=72 vs posterior n=58, dominant n=73 vs co-dominant n=50 vs non-dominant n=7) were included. Successful reperfusion (mTICI 2b or 3) among those undergoing EVT was seen in 59.2% of patients. Treatment effect favored EVT (adjusted OR 2.39, 95% CI 1.08 to 5.28, p=0.03) for 90-day mRS 0–2 (58.2% EVT vs 39.7% control). Direction of benefit favored EVT for other outcomes. Treatment effect favoring EVT was maximal in patients with proximal M2 segment MCA occlusions (n=116, adjusted OR 2.68, 95% CI 1.13 to 6.37) and in dominant M2 segment MCA occlusions (n=73, adjusted OR 4.08, 95% CI 1.08 to 15.48). No sICH (0%) was observed in patients treated with EVT compared with five (7.9%) in the control arm.
Conclusion Patients with proximal M2 segment MCA occlusions eligible for EVT trial protocols benefited from EVT.
- stroke
- intervention
- thrombectomy
Statistics from Altmetric.com
Introduction
Endovascular thrombectomy (EVT) works by recanalizing intracranial arteries in a timely and safe manner, saving ischemic brain from irreversible injury.1 The presence of salvageable brain tissue along with a target arterial occlusion that could be recanalized in a time bound manner and the safety of the procedure during such an attempt were the primary reasons why recent clinical trials showed efficacy of EVT over standard care.2 3 In an effort to establish a beachhead of evidence for EVT during a time when prior trials had shown lack of efficacy of EVT, trials published in 2015–17 focused on the more accessible, larger vessel anterior circulation (internal carotid artery (ICA) and M1 segment middle cerebral artery (MCA)) occlusions.4 These occlusion sites also lend themselves easily to imaging selection strategies used in these trials (eg, Alberta Stroke Program Early CT Score using non-contrast CT (NCCT ASPECTS), CT perfusion (CTP) ischemic core volume, or CT angiography (CTA) collateral assessments).5 6 Patients with M2 segment MCA occlusions were either deliberately excluded (eg, in the ESCAPE, SWIFT PRIME, REVASCAT, THRACE, and PISTE trials) or were undersampled (eg, in the MR CLEAN and the EXTEND IA trials).2 Questions about efficacy of EVT in patients with M2 segment MCA occlusions remain.7–9
Many proximal M2 MCA segment occlusions are as easily accessible for EVT as M1 segment MCA occlusions.8 Some M2 segment MCA arteries are the dominant artery supplying blood to a large portion of the MCA territory.10 A recent meta-analysis of data from 12 non-randomized studies suggested that EVT for patients with M2 segment MCA occlusions that can be safely accessed is associated with high recanalization rates and good clinical outcomes.7 Using patient level data from the HERMES (Highly Effective Reperfusion evaluated in Multiple Endovascular Stroke Trials) Collaboration therefore, we sought to test the hypothesis that EVT would result in better clinical outcomes among patients with M2 segment MCA occlusions compared with standard care. In addition, we asked whether certain anatomical characteristics of M2 segment MCA occlusions such as location, size, anatomy, and number of vessels occluded lend themselves better to EVT than others.
Methods
The HERMES Collaboration includes patient level data from the MR CLEAN, ESCAPE, REVASCAT, SWIFT PRIME, THRACE, EXTEND IA, and PISTE randomized controlled trials. Differences in patient population, sampling frame, and operational definitions of intervention (EVT) and control have been published previously.6 All baseline imaging was read by the HERMES central core laboratory blinded to clinical information. The core laboratory identified thrombus location at baseline on CTA (preferably) or MR angiography. Thrombus location was classified as either ICA, proximal and distal M1 segment MCA, or M2 segment MCA. An occlusion was considered to be in the distal M1 segment MCA and not in a M2 segment MCA if the only patent MCA arterial branch proximal to the occlusion was the anterior temporal artery.10 11 The M2 segment MCA with thrombus was subclassified based on (a) location (assessed on coronal images; proximal to the mid-sylvian point vs distal); (b) vascular territory supplied (anterior division supplying the anterior MCA region vs posterior division supplying the posterior MCA region); (c) size (dominant division supplying >50% of the MCA territory vs co-dominant supplying 50% of the MCA territory vs non-dominant supplying <50% of the MCA territory); and (d) number (1 branch involved vs >1 branch). Subject count included in analyses by trial were MR CLEAN (n=46), ESCAPE (n=18), EXTEND-IA (n=9), SWIFT PRIME (n=24), REVASCAT (n=21), PISTE (n=4), and THRACE (n=8).
Since M2 segment MCA occlusions only cause ischemia to a part of the MCA territory, it is reasonable to assume that patients with such occlusions are less likely to have large infarcts that are more commonly associated with a bedridden state or death even when not treated with EVT. Maximal benefit with EVT versus standard care is therefore likely to be seen on the lower end of the modified Rankin Scale (mRS) with minimal gains across higher levels of this scale.12 We therefore chose functional independence (mRS 0–2) as the primary outcome for this analysis. Secondary outcomes included excellent functional outcome (mRS 0–1) at 90 days, shift in mRS distribution at 90 days, and dramatic neurological improvement (defined as National Institute of Health Stroke Scale (NIHSS) score of 0–2 24 hours after stroke onset). Technical efficacy was assessed by revascularization at the end of the endovascular procedure, defined using modified Thrombolysis in Cerebral Infarction (mTICI) scale score of 2b or 3 corresponding to reperfusion of at least 50% of the affected vascular territory. Safety outcomes included symptomatic intracranial hemorrhage (sICH; defined by each trial) and death within 90 days.
Statistical analysis
All analyses were by intention to treat. Mixed effects modeling was used for all analyses, with fixed effects for parameters of interest and ‘trial’ and the interaction term ‘trial*treatment’ as random effects variables in all models. All adjusted regression models (binary logistic and ordinal) included fixed effects (age, sex, NIHSS score at admission, intravenous alteplase use, and time from onset to randomization). Heterogeneity of treatment effect by pre-specified clinical subgroups (age ≤70 vs >70 years, sex, NIHSS score at admission (≤10, 11–15, >15), baseline NCCT ASPECTS (≤8 vs 9–10), intravenous alteplase use, and time from stroke onset to randomization (≤300 min vs >300 min)) was assessed. Treatment effect in M2 segment MCA subtypes with sufficient sample size were also reported. All statistical analyses were performed using SAS v.9.2 (SAS Institute, Cary, North Carolina, USA).
Role of the funding source
The funders of the study had no role in study design, data analysis, data interpretation, or writing of the report.
Results
Baseline characteristics and workflow processes of patients with M2 segment MCA occlusions in the EVT and control groups are described in table 1. After excluding one patient with missing 90-day outcome, 130 patients with M2 segment MCA occlusions (proximal location (n=116) vs distal (n=14), anterior division (n=72) vs posterior division (n=58), dominant (n=73) vs co-dominant (n=50) vs non-dominant (n=7), single vessel (n=123) vs multi-vessel (n=7)) were included for further analysis. Sixty-seven patients were randomised to the EVT arm and 63 patients to the control arm. Successful reperfusion (mTICI 2b or 3) was observed in 59.2% of patients. Infarct core volumes at baseline were assessed on 64 patients (51 subjects using baseline CTP vs 13 baseline MRI). Median core volume was 12.6 mL (IQR 2.9, 28.6) by central assessment.
Baseline characteristics and workflow processes in patients with M2 segment MCA occlusions in endovascular therapy (EVT) and control groups
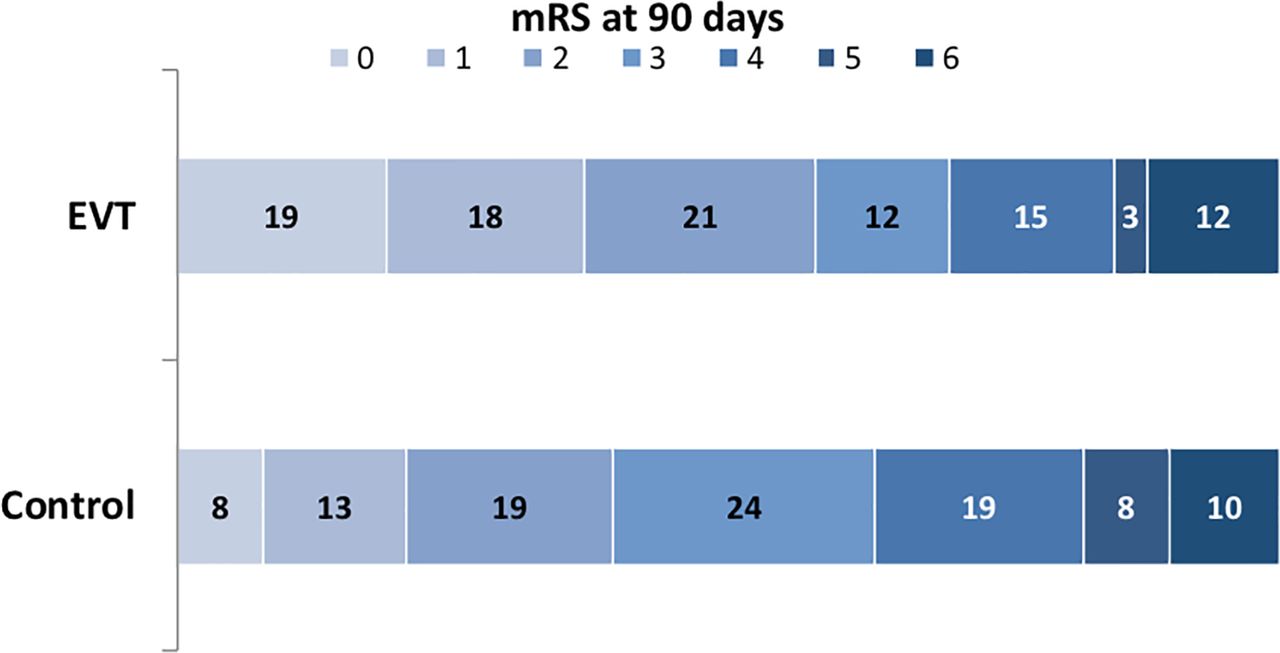
Figure 1 shows the distribution of mRS in the intervention arm versus controls in all patients included in this analysis. Treatment effect favored EVT over control (adjusted OR 2.39, 95% CI 1.08 to 5.28, p=0.03) for mRS 0–2 at 90 days. The corresponding unadjusted OR was 2.13 (95% CI 1.05 to 4.35; p=0.04; 58.2% with EVT vs 39.7% control), while the number needed to treat for one patient to have functional independence (mRS 0–2) was 5.4. The direction of benefit favored EVT over control for other outcomes but the results were not conventionally statistically significant (table 2). No sICH or major procedural complications were noted among patients treated with EVT compared with five (7.9%) in the control arm. Death at 90 days occurred in 11.9% of patients in the EVT group versus 9.5% in the control group (p=0.66). No statistically significant heterogeneity in treatment effect was noted by age, sex, NIHSS score at admission, baseline NCCT ASPECTS, intravenous alteplase use, and time from stroke onset to randomization (all p>0.05).
{kind=link}
Modified Rankin Scale (mRS; unadjusted) distribution at 90 days in patients with baseline CT or MR angiography-defined M2 segment middle cerebral artery (MCA) occlusions. Benefit with endovascular thrombectomy (EVT) is better seen on the left side of the mRS scale.
Unadjusted and adjusted clinical and safety outcomes in patients with M2 segment MCA occlusions
Treatment effect favoring EVT was maximal in patients with proximal M2 segment MCA occlusions (n=116, adjusted OR 2.68, 95% CI 1.13 to 6.37, p=0.02 for mRS 0–2 at 90 days, 57.1% EVT vs 37.7% control, respectively) when the involved M2 segment MCA was dominant (n=73, adjusted OR 4.08, 95% CI 1.08 to 15.48, p=0.04 for mRS 0–2 at 90 days, 61.5% EVT vs 44.1% control, respectively) and when a single M2 segment MCA was involved (n=123, adjusted OR 2.73, 95% CI 1.19 to 6.27, p=0.02 for mRS 0–2 at 90 days, 58.5% EVT vs 37.9% control, respectively). The direction of benefit favored EVT for these subtypes of M2 segment MCA occlusion across most secondary outcomes (table 3). Benefit with EVT was seen in patients with anterior and posterior division M2 segment MCA occlusions, although smaller sample sizes meant results did not reach statistical significance (results not shown). However, no statistically significant heterogeneity in treatment effect was noted across any M2 segment MCA occlusion type.
Unadjusted and adjusted clinical and safety outcomes in patients with proximal M2 segment MCA occlusion, single vessel M2 segment middle cerebral artery (MCA) occlusions and dominant M2 segment MCA occlusions
Discussion
Endovascular therapy is now standard care in patients with ischemic stroke due to emergent anterior circulation large vessel occlusions.13 The Society of Neurointerventional Surgery (SNIS) recently revised its operational definition of emergent large vessel occlusion (ELVO) to include proximal M2 segment MCA occlusions in addition to intracranial carotid artery and M1 segment MCA occlusions.8 The American Stroke Association guidelines assign this occlusion site a lesser degree of evidence of benefit with EVT compared with the ICA or M1 segment MCA occlusions.14 This analysis of patients with M2 segment MCA occlusions from the HERMES Collaboration of seven recent randomized controlled trials shows that EVT, especially in patients with proximal or dominant M2 segment MCA, results in improvement in functional ability at 90 days when compared with best medical care.
Mechanical embolectomy devices are designed to suit the target arterial profile and access. Devices that work well in the proximal arterial segments are less likely to suit the arterial profile and access demands of distal arterial segments. A proximal segment or dominant M2 MCA branch, however, does not necessarily pose significantly increased difficulty in access when compared with the distal M1 segment MCA. This is substantiated by the fact that our analysis showed no intracerebral hemorrhage or major procedural complications in these patients. Moreover, patients with dominant M2 MCA branch occlusions have a substantial volume of ischemic brain that could potentially be salvaged with EVT, thus increasing chances of benefit with this therapy. The successful reperfusion (mTICI 2b/3) rates noted in this analysis (59.2%) are significantly better than that obtained with intravenous alteplase in patients with M2 segment MCA occlusions.15 The reperfusion rates with EVT could improve further with the use of smaller diameter next-generation stent retrievers and aspiration devices, further improving clinical outcomes in these patients.16 17
The functional independence rates at 90 days noted in this study are comparable to the results from a recent meta-analysis of 12 non-randomized studies reporting outcomes in patients with M2 segment MCA occlusions treated with EVT (58.2% vs 59% 90-day mRS 0–2 rates).7 Interestingly, successful recanalization rates in these 12 non-randomized studies (81% overall) were higher than that noted in the current study (59.2%) while the symptomatic ICH (10% vs 0%) and death (16% vs 11.9%) rates were higher, highlighting the need for good patient selection and the use of appropriate endovascular techniques in these patients.
Although this analysis represents high-quality randomized trial data, caution in interpretation is warranted. Differences in baseline characteristics (eg, median baseline ASPECTS 9 in the EVT group vs 8 in the control group, difference not statistically significant) may potentially explain better outcomes in the EVT group. The seven recent RCTs testing EVT efficacy included in the HERMES Collaboration did not include all patients with M2 segment MCA occlusions (by design or otherwise).6 We cannot therefore rule out the possibility of selection bias influencing these results. Only 130 patients were available for analysis, potentially resulting in analysis of effect modification by M2 segment MCA occlusion type being underpowered to show efficacy of EVT. Nonetheless, point estimates of all reported clinical outcomes favouring EVT provide confidence that EVT benefits these patients. Finally, the choice of the primary outcome (mRS 0–2 proportion at 90 days) was based on a careful assessment of the outcome distribution on the mRS scale and may therefore be considered post hoc.12
In conclusion, this analysis from recent randomized controlled trials provides additional evidentiary support for the efficacy of EVT versus current non-endovascular acute stroke therapy in patients with M2 segment MCA occlusions.
References
Footnotes
Contributors BKM and MG had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: BKM, MDH, DWJD, JLS, TJ, AvdL, MG. Acquisition, analysis, or interpretation of data: AD, YBWEMR, BCVC, FG, AMD, KM, PM, PW, SB. Drafting of the manuscript: BKM, SB, MDH, DWJD, MG. Critical revision of the manuscript for important intellectual content: All authors. Statistical analysis: SB. Obtained funding: MG. Administrative, technical, or material support: MDH, SB. Study supervision: BKM, MG.
Funding This work was supported by an unrestricted grant provided to the University of Calgary by Medtronic Inc.
Competing interests MDH owns stock in Calgary Scientific Inc, a company that focuses on medical imaging software, is a director of the Canadian Federation of Neurological Sciences, a not-for-profit group and has received grant support from Alberta Innovates Health Solutions, CIHR, Heart & Stroke Foundation of Canada, National Institutes of Neurological Disorders and Stroke. YBWEMR reports Stock ownership of Nico-Lab, outside the submitted work. BCVC reports grants from National Health and Medical Research Council, Royal Australasian College of Physicians, Royal Melbourne Hospital Foundation, National Heart Foundation, National Stroke Foundation of Australia, Covidien (Medtronic) during the conduct of the study. KM reports grants from Medtronic and from Codman outside the submitted work. AMD reports personal fees from Medtronic during the conduct of the study. TJ has consulted for Codman Neurovascular and Neuravi; holds stock in Silk Road, Anaconda, Route 92, and Blockade; received travel expenses from Stryker as primary investigator of the DAWN trial and from Fundacio Ictus related to the REVASCAT and RACECAT trials. PM reports receiving consulting fees from Medtronic and Stryker, personal fees from Stryker and Microvention outside the submitted work. PW reports grants from National Institutes for Health Research, the Stroke Association, Medtronic (Covidien), and Codman and has consulted for Microvention Terumo and Codman. AvdL reports grants from Dutch Heart Foundation, and consulting fees from AngioCare BV, from Covidien/EV3, from MEDAC Gmbh/LAMEPRO, from Stryker, from Penumbra Inc, during the conduct of the study; grants from Stryker, grants from Penumbra Inc, grants from Medtronic outside the submitted work. JLS has acted as a scientific consultant regarding trial design and conduct for Medtronic. SB reports personal fees from University of Calgary during the conduct of the study; personal fees from Medtronic outside the submitted work. MG reports grants from Medtronic and personal fees from Stryker, Medtronic, Microvention, and Cerenovus during the conduct of the study; grants from Stryker outside the submitted work. In addition, MG has a patent Systems of Acute Stroke Diagnosis issued to GE Healthcare.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are available within the article. Any additional data will be made available, upon reasonable request, by the corresponding author after getting approval from the HERMES executive.
Patient consent for publication Not required.