Article Text

Abstract
Background and purpose The shorter the time interval between the estimation of the ischemic core by imaging and reperfusion, the more likely that core expansion is minimized. We aimed to assess the feasibility of achieving an ultrashort imaging to reperfusion time in routine clinical practice.
The study subjects were a prospective cohort of patients with acute ischemic stroke treated with endovascular therapy in a tertiary center in whom an imaging to reperfusion time of <60 min was achieved.
Results Imaging to reperfusion time of <60 min was accomplished in 11 patients. The median baseline National Institutes of Health Stroke Scale (NIHSS) score was 11 and the median baseline Alberta Stroke Program Early CT Score (ASPECTS) was 8. The median time interval from imaging to endovascular reperfusion was 47 min. The median ASPECTS score on the 24 h CT scan was also 8 and the median 24 h NIHSS score was 1. Upon discharge, 82% of patients achieved a modified Rankin scale score of ≤1.
Conclusions An imaging to endovascular reperfusion time of <60 min is feasible and resulted in minimal core expansion on follow-up imaging in patients with acute ischemic stroke.
- Stroke
- Thrombectomy
- Brain
- CT
- Intervention
Statistics from Altmetric.com
Background
Acute ischemic stroke is a dynamic process. Following cerebral arterial occlusion, the ischemic penumbra undergoes changes leading over time to the establishment of an ischemic core (infarct). Unless reperfusion is achieved, the core continues to expand until the entire area of penumbra is incorporated into the core. While the rate of core expansion remains largely unknown, animal studies have shown that about half of the final core volume is reached within the first 3 h of stroke onset and by 6–8 h almost the entire penumbra evolves into core.1 ,2
The urgency in the treatment of patients with acute ischemic stroke cannot be overemphasized. Experimental studies have shown complete neurological recovery when the occlusion time was <2 h.3 The degree of functional impairment and final infarct size were proportional to the time in occlusion beyond 2 h.4 Others have demonstrated a significant drop in tissue perfusion in the penumbra beyond 4 h from occlusion onset which minimized the area of salvageable brain tissue.5
These observations of the rapid rate of evolution of the ischemic penumbra motivated the testing and then approval of intravenous tissue plasminogen activator (tPA) within 3 h of onset of stroke symptoms. However, the exact time course of action of intravenous tPA from the time its loading dose is administered to the end of the 60 min infusion is not clear. In one study which used transcranial Doppler to continuously monitor 65 acute stroke patients receiving intravenous tPA, full reperfusion was observed in about 52% of patients within a mean time of 42 min after the tPA bolus.6 Only five patients (11%) achieved sudden reperfusion (<1 min) which resulted in dramatic recovery in all five patients. These findings highlight the strong correlation between fast reperfusion and significant recovery. It also shows the small proportion of patients achieving sudden and complete reperfusion with intravenous tPA alone.
Imaging remains a key tool in determining the extent of infarction in acute ischemic stroke. However, since imaging offers a single ‘snapshot’ in time, it provides little information about the rate of infarct growth. This led to the concept of ‘Time is Brain’—the faster reperfusion is achieved, the more penumbra tissue is saved.7 It is intuitive that the shorter the time interval between estimation of core by imaging and reperfusion, the more likely that infarct expansion is minimized. Furthermore, if reperfusion is achieved quickly, infarct estimation on baseline imaging might be an accurate estimation of final infarct size.
To explore this premise, we prospectively attempted to achieve a proposed imaging to reperfusion time of ≤60 min. We set a target of 60 min imaging to endovascular reperfusion time to allow for the time for starting intravenous tPA and for travel by the angiography team.
Methods
Design and population
This is a single-center case series from a prospectively-maintained database of patients treated with endovascular stroke therapy from October 2011 to February 2012. Informed consent was obtained prior to treatment from patients, their surrogate decision makers, or from two physicians involved in the patients’ care in accordance with institutional protocol.
Clinical characteristics and outcome measures
Patient demographics, time of onset of stroke symptoms or last seen normal and baseline stroke severity as assessed by the National Institutes of Health Stroke Scale (NIHSS) scores were documented by a stroke neurologist or fellow in training. All patients underwent an unenhanced CT scan of the head followed by CT angiography of the head and neck vessels. The Alberta stroke program early CT score (ASPECTS) was scored and a decision was then made regarding intravenous and/or intra-arterial thrombolysis.
Procedural details
Retrievable stents were used in all cases: Solitaire FR device (Covidien; Irvine, California, USA) in 10 patients and Trevo (Concentric Medical; Mountain View, California, USA) in one patient. Successful reperfusion was defined as Thrombolysis in Cerebral Ischemia (TICI) score of 2b (perfusion of half or more of the vascular distribution of the occluded artery) or 3 at the end of the procedure.8
The imaging time was defined as the time of the last image of the CT/CT angiography series obtained from the picture archiving and communication system. The time of reperfusion was defined as the time of the angiogram which documented successful reperfusion after the stent was retrieved.
Statistical analysis
Measured variables are reported as medians and compared using the Mann–Whitney U test. Categorical variables were reported as proportions. Analyses were performed using Stata 10 software (Stata Corp, College Station, Texas, USA).
Results
Of 29 patients treated since October 2011, 11 (38%) achieved an imaging to reperfusion time of <60 min. The results of these 11 patients are presented here. The patient characteristics are shown in table 1. The median age was 62 years, median NIHSS score at presentation was 11 and the median ASPECTS score was 8. The most common occlusion site was the proximal (M1) middle cerebral artery (46%). In all 11 patients the procedure was performed under local anesthesia.
Characteristics of the patient cohort
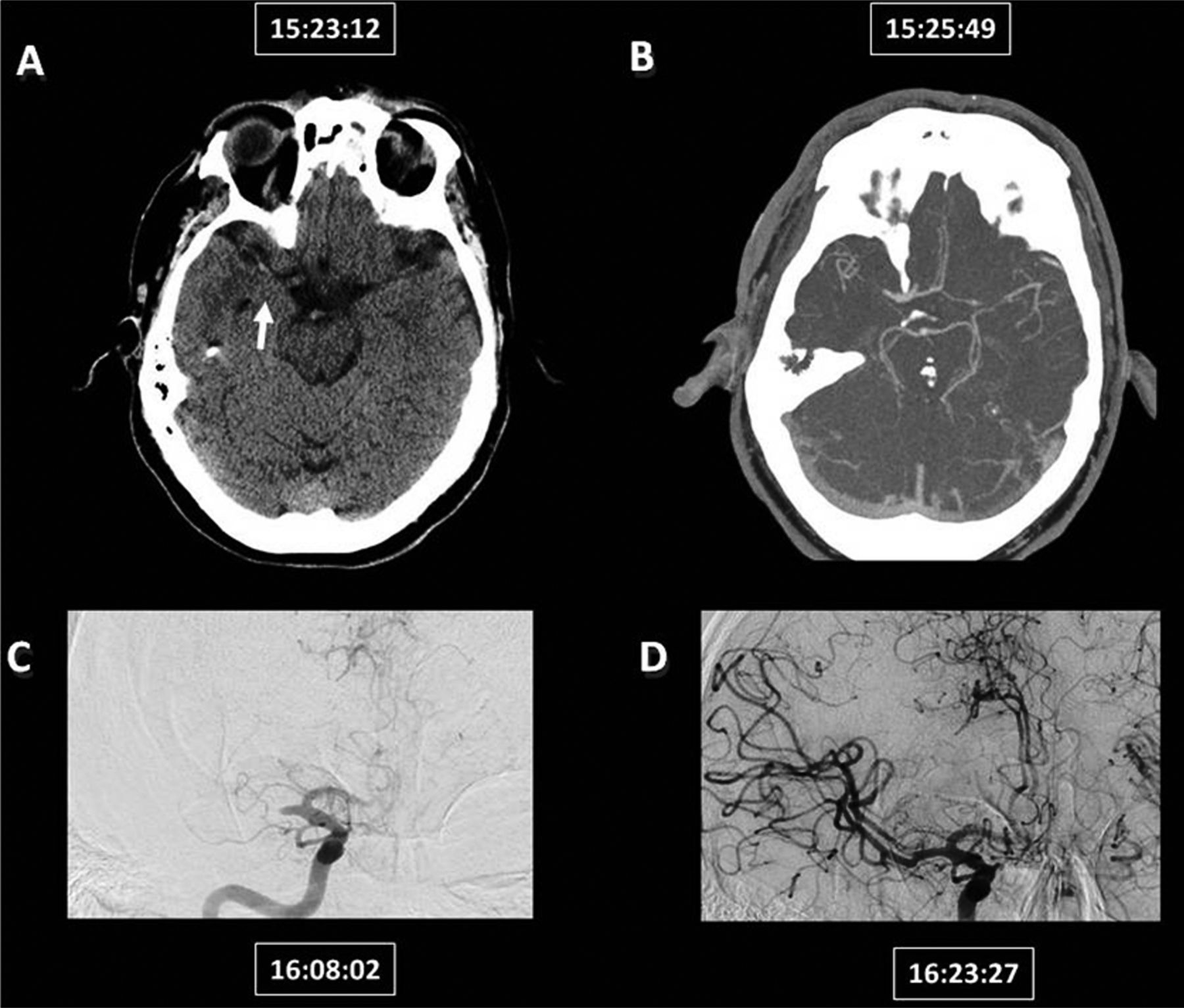
Intravenous tPA was given in 27% of patients. The reasons for not giving intravenous tPA included presentation outside the intravenous tPA treatment window and high INR. All cases had a baseline TICI score of 0. Successful reperfusion (TICI 2b/3) was achieved in all cases; half had complete reperfusion (TICI 3). Only one patient was treated with intra-arterial tPA in addition to the retrievable stent. None of the patients had thromboembolic events to the same or new vascular territories. The median time interval from imaging to reperfusion was 47 min and the median time interval from onset to reperfusion was 131 min. There were no immediate procedural complications. Images from an illustrative case are shown in figure 1.

An illustrative case: a middle-aged patient with National Institutes of Health Stroke Scale score of 17 due to a right M1 occlusion. Images show the times for the non-contrast CT (A; arrow: hyperdense sign), CT angiogram (B) which shows the right M1-middle cerebral artery occlusion, the first angiographic run (C) and the final angiographic run after reperfusion (D) with good contrast washout of the anterior cerebral artery from the contralateral side.
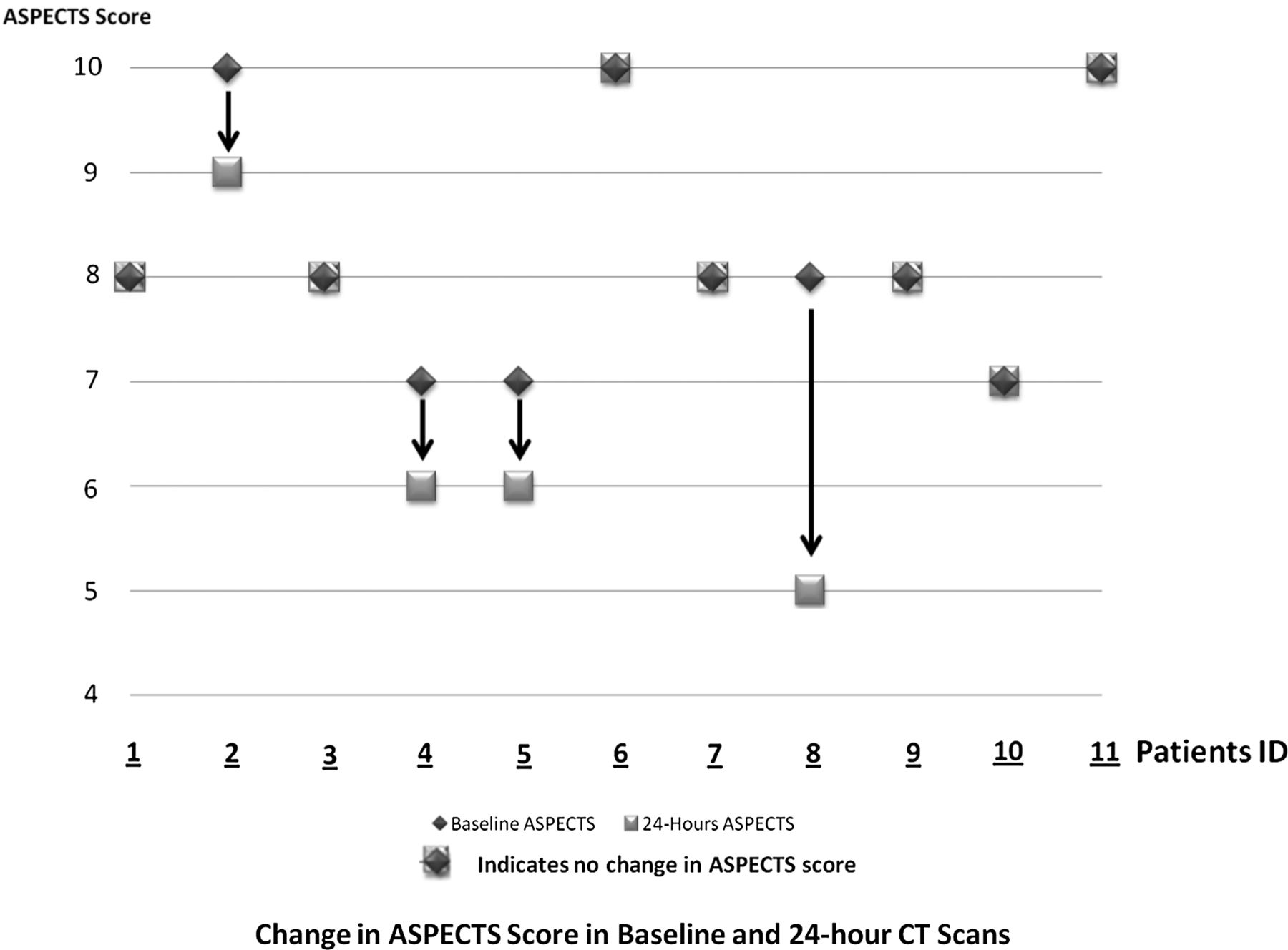
The median 24 h ASPECTS score was 8 (figure 2). There was no significant difference in the median ASPECTS scores of baseline and 24 h CT scans (p=0.49, Mann–Whitney test). The median 24 h NIHSS score was 1. Four patients (36%) had a 24 h NIHSS scale of 0. The median modified Rankin scale (mRS) score at discharge was 1. In this cohort, 82% of patients achieved an mRS score of ≤1 upon discharge.
{kind=link}
{kind=link}
Changes in baseline and 24 h Alberta Stroke Program Early CT Score (ASPECTS).
Among the 18 patients who did not meet the 60 min cut-off, one patient (5.6%) died during hospitalization, only one patient (5.6%) had a 24 h NIHSS score of zero and 12 patients (66.7%) achieved an mRS score of 0–1 at discharge.
Discussion
In this prospective study we show the feasibility of achieving an imaging to reperfusion time of <60 min in patients undergoing endovascular stroke therapy. This resulted in minimal core expansion on follow-up imaging. A discharge mRS score of ≤1 was achieved in 82% of cases. This surpasses the outcomes previously reported in patients who did not meet this target time. In a cohort of 27 patients treated with the Penumbra system9 and in 14 patients treated with Solitaire retrievable stents10 the median puncture to reperfusion times were 80 and 84 min, respectively, indicating an imaging to reperfusion time interval of >60 min. A good clinical outcome at discharge (mRS ≤2) was achieved in 48% of patients treated with the Penumbra system and in 57% of those in whom Solitaire stents were used, compared with 82% of patients achieving mRS ≤1 in the present study.
Despite evidence from experimental studies, the rate of ischemic core expansion in humans remains unknown. Nevertheless, the efficacy of reperfusion is time-dependent: the faster reperfusion is achieved, the more brain tissue is preserved. These assumptions are supported by evidence from a meta-analysis of 2066 patients with spontaneous or therapeutically-induced reperfusion.11 In that report, studies with a documented reperfusion time within 6 h of onset of symptoms showed a stronger effect of successful reperfusion on outcomes than studies reporting later reperfusion. The effect of time from symptom onset to intervention on stroke outcome was also shown in intravenous thrombolysis studies. In a meta-analysis of 3670 patients receiving intravenous tPA, the adjusted odds of a favorable outcome at 3 months progressively increased as the time from onset to intravenous tPA treatment decreased.12
Short onset to reperfusion time may not entirely account for the favorable effects of reperfusion. A pooled analysis of the MERCI/Multi MERCI trials showed that 40% of the patients who achieved a final Thrombolysis in Myocardial Infarction score of 2 or 3 at or beyond 6.9 h still achieved independent functional outcomes. 13 Based on this report, such patients can achieve excellent recovery if the imaging to reperfusion time is accomplished rapidly, even outside the standard treatment window, as we move towards a paradigm of imaging-based patient selection. While the imaging to reperfusion time is only one of several important time intervals that start at the stroke onset time, a number of other factors could potentially modify the core expansion rate such as blood glucose level,14 collateral status15 and peri-infarct depolarization.16 The effects of these factors need to be considered in addition to the time of achieving full reperfusion.
Our report has limitations. This is a single-center report in which the treatment approach was tailored on a case-by-case basis. Our approach to imaging-based patient selection involves the use of unenhanced CT and CT angiography of the head and neck vessels without perfusion imaging. Our small sample size also makes it hard to draw definitive conclusions about the effect of a short imaging to reperfusion time. However, we demonstrate the feasibility of achieving an ultrashort imaging to endovascular reperfusion time in routine clinical practice.
Conclusion
Targeting ultrashort (<60 min) imaging to endovascular reperfusion time in ischemic stroke therapy is feasible and resulted in minimal expansion of the core based on ASPECTS scoring.
Acknowledgments
We would like to thank all members of the Calgary Stroke Program who participated in the care of these patients.
References
Footnotes
-
Contributors Conceptual design: MG. Data collection: MA, ME, BM. Analysis: MA, ME, BM, AD, MG. Drafting: MA, ME. Critical review: MG, AD, BM.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Conjoint Health Research Ethics Board at the University of Calgary prior to patient enrollment.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement These data are part of an ongoing prospectively-collected endovascular database at the University of Calgary Stroke Program. Data are maintained and updated continuously. The data are only accessible to the Calgary Stroke Program investigators.