Article Text

Abstract
Background Antiplatelet agents are required to prevent thromboembolic complications from recently deployed intracranial stents, yet they carry a risk of bleeding complications that may be serious in patients with recent subarachnoid hemorrhage.
Method Consecutive patients at a single institution who had ruptured intracranial saccular aneurysms treated with stent assisted coiling were retrospectively reviewed. Our primary outcomes were ischemic stroke related to the stent and bleeding complications possibly related to antithrombotic therapy. Secondary outcomes included 3 month follow-up National Institute of Health Stroke Scale (NIHSS) scores and modified Rankin Scale (mRS) scores.
Results 44 aneurysms in 42 patients were treated. Seven patients experienced ischemic strokes during their hospitalization. Five ischemic strokes were secondary to vasospasm; one was definitely related to thrombus formation within the stent and one was possibly related to the stent. Two patients had asymptomatic intracranial hemorrhages and one patient had a symptomatic intracranial hemorrhage. Patients with Hunt and Hess grades I–II (n=25) experienced no stent associated ischemic strokes or symptomatic intracranial hemorrhages. The two stent associated ischemic strokes and one symptomatic intracranial hemorrhage occurred in patients with Hunt and Hess grades III–V (n=17) and patients with external ventricular drains (EVDs) (n=17). Only one patient had disability at the 3 month follow-up that was possibly related to the stent (mRS score of 3 and NIHSS score of 2).
Conclusion These data suggest that higher grade hemorrhage patients, especially those with EVDs, are at greater risk for ischemic stroke and/or bleeding complications than lower grade patients. However, the complications had a small impact on mid-term disability outcomes in this cohort.
- Subarachnoid
- Aneurysm
- Coil
- Complication
- Stent
Statistics from Altmetric.com
Wide necked cerebral aneurysms pose a challenge for endovascular treatment because of problems with stability of the coils within the aneurysm. Various endovascular techniques have been described, including combined surgical clipping and coiling,1 use of two microcatheters2 and balloon remodeling.3–7 The Neuroform stent was approved for use in the USA in November 2002 under a Humanitarian Device Exemption and has been used to treat wide necked aneurysms.8–19
Use of the intracranial stents to treat acutely ruptured aneurysms is controversial. There is likely a higher risk of thrombus forming within the stent and resulting in thromboembolic ischemic strokes because these patients are generally not pretreated with antiplatelet agents.8 9 11 19 There is also likely a higher risk of bleeding complications from the use of double antiplatelet agents and glycoprotein (GP) IIb/IIIa inhibitors. The bleedings risks may be augmented further by the presence of vasospasm infarcts the presence or placement of ventriculostromy catheters and may the need for other invasive procedures such as ventriculoperitoneal shunts.20 We reviewed our institution's experience with Neuroform stent assisted coiling of acutely ruptured intracranial aneurysms to evaluate these risks and assess outcomes.
Methods
We have been using the Neuroform stent to treat unruptured intracranial aneurysms since 2002 and ruptured intracranial aneurysm since November 2003 under an institutional review board (IRB) approval (IRB–01 200210057). We retrospectively reviewed a prospectively collected database of all neurointerventional radiology procedures performed at a single hospital between November 2003 and March 2008. All patients who underwent stent assisted coiling of ruptured aneurysms were identified. Patients who had ruptured pseudoaneurysms were excluded.
Patients
Patients with subarachnoid hemorrhage were screened for aneurysms initially with CT angiogram, and then a decision about best treatment modality, coiling or clipping was made jointly between the neurosurgery and neurointerventional teams. Patients in whom there was uncertainty as to whether coiling was feasible subsequently underwent diagnostic angiography. Patient information collected included age, sex, aneurysm location, aneurysm size, Hunt and Hess grade, Fisher grade, number of days after aneurysm rupture that stent placement was performed, whether a ventriculostomy catheter was placed, periprocedure heparin dose, periprocedure tirofiban dose (if given), whether clopidogrel (Plavix; Bristol-Myers Squibb/Sanofi Pharmaceuticals, New York, New York, USA) and/or aspirin was given, whether an invasive procedure that may be associated with increased bleeding risk was performed, major medical complication, National Institute of Health Stroke Scale (NIHSS) score at the 3 month follow-up, modified Rankin Scale (mRS) score at the 3 month follow-up and whether the aneurysm needed recoiling at the 6 month follow-up. Modified Fisher grade was assigned based on retrospective review of the initial head CT (RAT, RCC, MH).
Endovascular technique
The Neuroform stent was used when it was felt that the coils would not be stable within a wide necked aneurysm at the discretion of the primary operator (JC). The decision to use a Neuroform stent was sometimes not made until after an attempt to primarily coil the aneurysm was performed first. Partial coiling of the aneurysm dome or suspected rupture site was performed first if feasible, followed by stent deployment and finishing of aneurysm coiling (figure 1). This was done to protect the rupture site in case there was acute stent thrombosis and a GP IIb/IIIa inhibitor needed to be emergently administered.

Endovascular technique (patient No 34). Cerebral angiogram anteroposterior view of the brain from a right vertebral artery injection shows partial coiling of the suspected aneurysm rupture site (A), performed to help protect the aneurysm from intraprocedural rupture. The patient was then fully anticoagulated and the Neuroform stent was positioned from the right P1 segment to the mid-basilar artery (B) and then deployed. The rest of the aneurysm was then coiled with the final result shown and distal stent marker bands shown with arrows (C). The distal arrow denotes the distal end of the Neuroform stent in the right P1 segment and the proximal arrow denotes the proximal end of the stent.
A Neuroform2 or Neuroform3 stent system (Boston Scientific, Natick, Massachusetts, USA was loaded over a 200 cm Transcend EX 14 0.014 inch microwire (Boston Scientific). Stents were sized about 0.5 to 1.0 mm greater than the parent vessel. The stent system was then advanced through 5 or 6 French MPD guiding catheters (Cordis Neurovascular, Miami Lakes, Florida, USA) or 6 French shuttle sheath (Cook Corp, Bloomington, Indiana, USA). The stent catheter system was advanced over the 200 cm Transcend EX 14 0.014 inch microwire across the neck of the aneurysm. The stent was deployed using the 200 cm Transcend EX 14 0.014 inch microwire, coil pusher (Boston Scientific/Cordis Endovascular) or hypotube stabilizer. The SL-10 microcatheter (Boston Scientific) was advanced over a Transcend EX 14 or Synchro 0.014 inch microwire (Boston Scientific) to select the aneurysm.
Periprocedure ischemic stroke prevention
Periprocedure ischemic stroke prevention included empiric intravenous unfractionated intravenous heparin dosed by weight (50 units/kg bolus), followed by 1000 units/h. Clopidogrel 375 mg loading dose was given immediately after the procedure via nasogastric tube or by mouth immediately after extubation followed by clopidogrel 75 mg daily in all patients. This dose was chosen based on evidence that a clopidogrel loading dose between 300 mg and 600 mg can achieve maximal platelet inhibition within 6 h.21 Aspirin 325 mg was given immediately after the procedure followed by 325 mg daily if bleeding risk was felt not to be high. If the patient required a surgical procedure, such as ventriculoperitoneal shunt, clopidogrel was usually stopped but aspirin continued periprocedure.
Tirofiban (Aggrastat: Merck, West Point, Pennsylvania, USA) was given during the procedure if filling defects thought to be platelet aggregates were seen within the stent (figure 2) or as a prophylactic antithrombotic agent. The cardiac bolus dose of 0.4 μg/kg/min was given over 15 min with or without a maintenance infusion at 0.1 μg/kg/min if there was no significant early improvement with the bolus dose. Tirofiban was started after the aneurysm was secured with coils.

Platelet aggregates (patient No 13). Cerebral angiogram lateral view from a right internal carotid artery injection (A) shows a filling defect at the distal margin of the aneurysm neck within the stent (arrow) which improved after administration of intravenous tirofiban bolus dose (B). A continuous infusion of tirofiban was given for 80 min in this case.
Outcome measures
Our primary outcome measures included ischemic strokes and bleeding complications potentially related to the use of the Neuroform stent. Ischemic strokes were judged to be definitely related to the stent if the stroke occurred in the vascular territory of the stent and the thrombus was seen within the stent on angiography. Ischemic strokes were judged to be possibly related to the stent if the stroke occurred in the vascular territory of the stent and no other clear source of stroke was found, such as vasospasm or thrombus within the stent. Ischemic strokes were considered secondary to vasospasm if they occurred in a vascular distribution other than the stented vessel or occurred in vascular territory of the stented vessel but severe vasospasm on angiogram was found in the distribution of the infarct and no filling defects were seen on the stent. All bleeding complications were recorded and classified into four categories: symptomatic intracranial hemorrhage, asymptomatic intracranial hemorrhage, serious (if life-threatening or requiring surgical intervention) or minor (if self-limiting and without long term sequelae). Secondary outcomes included mRS score and NIHSS score at the 3 month clinic follow-up. NIHSS and mRS scores were performed routinely at the clinic follow-up or assigned after retrospective chart review (RAT, RCC).
Results
Patient characteristics
Patient characteristics are outlined in tables 1 and 2. Forty-four aneurysms in 42 patients were treated between 0 and 14 days of symptom onset (median 2 days, mean 3.4 (3.6) days). Ages ranged from 26 to 88 years (median 54 years, mean 57.3 (15.4) years). There were 27 women and 15 men. Twenty-five patients had initial Hunt and Hess grades I–II while 17 patients had Hunt and Hess grades III–IV. Thirteen patients had modified Fisher grades 1–2 and 31 patients had modified Fisher grades 3–4. Seventeen patients had ventriculostomy catheters placed, 15 of which were placed prior to aneurysm coiling and two after aneurysm coiling.
Clinical summary of all patients with Hunt and Hess grades I–II
Clinical summary of all patients with Hunt and Hess grades III–V
Aneurysm characteristics
The 44 saccular aneurysm locations included: nine posterior communicating artery, eight basilar summit, eight paraclinoid internal carotid artery, five anterior communicating artery, four superior cerebellar artery, three middle cerebral artery, two anterior choroidal artery, one terminal internal carotid artery, one posterior inferior cerebellar artery, one A1–A2 junction aneurysm, one A1 aneurysm and one P1 aneurysm. Aneurysm sizes (largest diameter) are listed in tables 1 and 2. Complete or near complete aneurysm occlusion (90% or greater) was achieved in all cases.
Antithrombotic treatment
Intraprocedural unfractionated intravenous heparin doses ranged between 0 units and 7000 units (median dose 4000 units). Heparin dose was given by patient weight and then adjusted for risk of bleeding, such as presence of intraparenchymal hematoma, recent ventriculostomy catheter placement or recent craniotomy. Nineteen patients were given the GP IIb/IIIa inhibitor, tirofiban, as a bolus dose during the procedure followed by an up to 3 h continuous infusion. Seven patients were given tirofiban as prophylactic treatment (patient Nos 15, 19, 24, 25, 26, 29 and 41) while the other 12 patients were given tirofiban because of the formation of platelet aggregates within the stent. Four patients who received tirofiban had ventriculostomy catheters in place and none had a bleeding complication related to the use of tirofiban (patient Nos 24, 26, 30 and 42). One patient who received tirofiban had a ventriculostomy catheter placed the following day without bleeding complications (patient No 19). All patients were loaded with clopidogrel 375 mg immediately after the procedure and treated with clopidogrel 75 mg daily for 3 months. Thirty-seven patients were also treated with aspirin immediately after the procedure followed by daily dosing for 3 months. Five patients were not treated with aspirin immediately after the procedure for the following reasons: (1) recent craniotomy with small epidural hematoma (patient No 18, aspirin was later started on post-craniotomy/coiling day 12); (2) individual staff's concern about double antiplatelets in a patient with ventriculostomy catheter (patient No 35, aspirin was started on post-procedure day 24 after the ventriculostomy catheter was removed); (3) history of cirrhotic liver (patient No 16); (4) history of chronic immunosuppression, chronic anemia, ventriculostomy catheter and need for invasive procedures such as bronchoscopy (patient No 26); and (5) ventriculostomy catheter placement and obvious need for subsequent ventriculoperitoneal shunt (patient No 37).
Intraprocedural complications
There were no technical complications related to stent deployment. There were no periprocedure aneurysm ruptures. A coil unraveled in one patient (patient No 37). This coil was successfully placed into the aneurysm but had a coil loop in the parent vessel lumen. There were no adverse sequelae to this. A coil herniated into the stent in one patient (patient No 29). This patient was treated with tirofiban prophylactically to prevent periprocedure thromboemboli and did not suffer clinical sequelae.
In-stent platelet aggregation was the most common intraprocedural complication, seen in 12 patients (29%) (figure 2). All of these patients were treated with intravenous tirofiban. One of these 12 patients suffered an ischemic stroke (patient No 42) and one patient suffered an asymptomatic intracerebral hemorrhage along the ventriculostomy tract (patient No 30).
Ischemic strokes
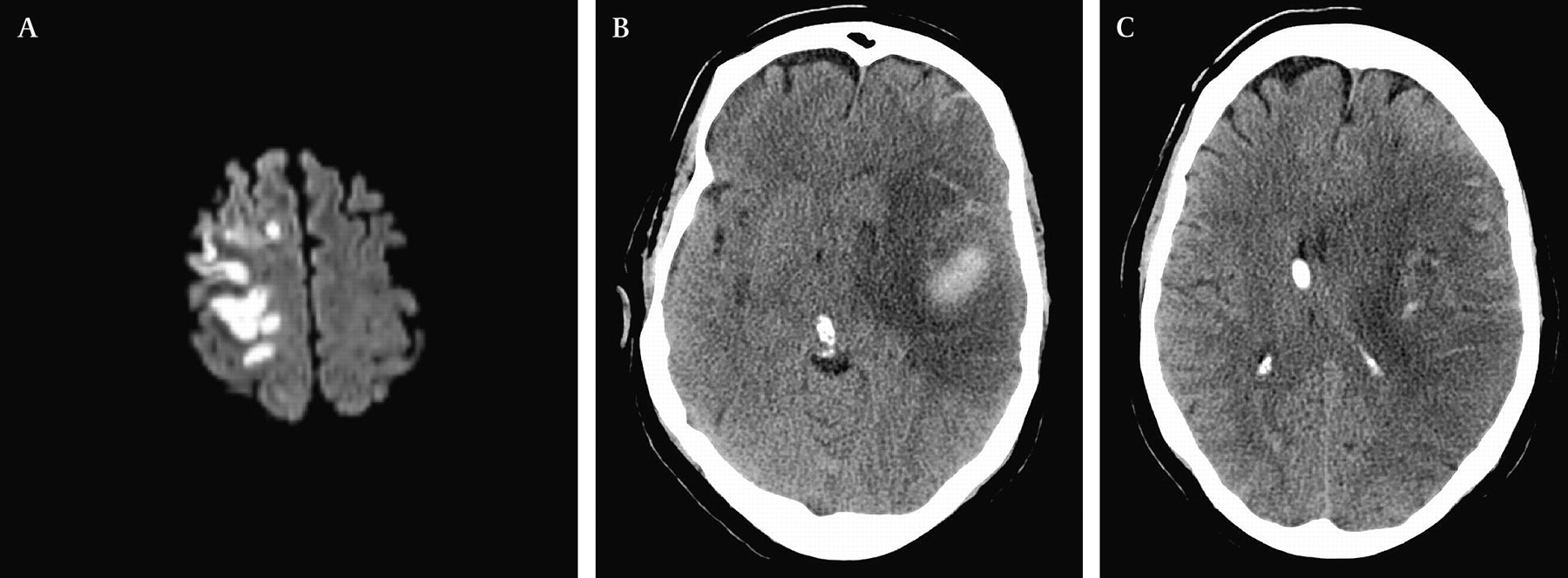
A total of seven patients experienced ischemic strokes (see table 3). One patient had an ischemic stroke definitely related to the stent (patient No 42) and one patient had an ischemic stroke possibly related to the stent (patient No 14) (see figure 3). Five patients had ischemic strokes secondary to cerebral vasospasm.
All ischemic stroke and bleeding complications

Ischemic stroke complications related to the stent. Patient No 26 experienced sudden left arm plegia (National Institute of Health Stroke Scale (NIHSS) score of 4) on hospital day 22. MRI diffusion weighted images showed a right frontal cortical ischemic stroke (A). Cerebral angiogram showed no vasospasm and no filling defects within the stent. This event occurred while the patient was on clopidogrel only and within 24 h of an episode of paroxysmal atrial fibrillation. Modified Rankin Scale score at the 3 month follow-up was 3 and NIHSS score was 2 (left arm weakness). Patient No 42 experienced in-stent thrombus during coiling of the aneurysm that was treated with intravenous tirofiban. Head CT performed several days later shows hypodensity in the left middle cerebral artery territory representing a combination of perihematoma edema and ischemic stroke (B and C). Care was withdrawn on hospital day 17 due to lack of clinical improvement from the initial Hunt and Hess grade V hemorrhage.
Bleeding complications
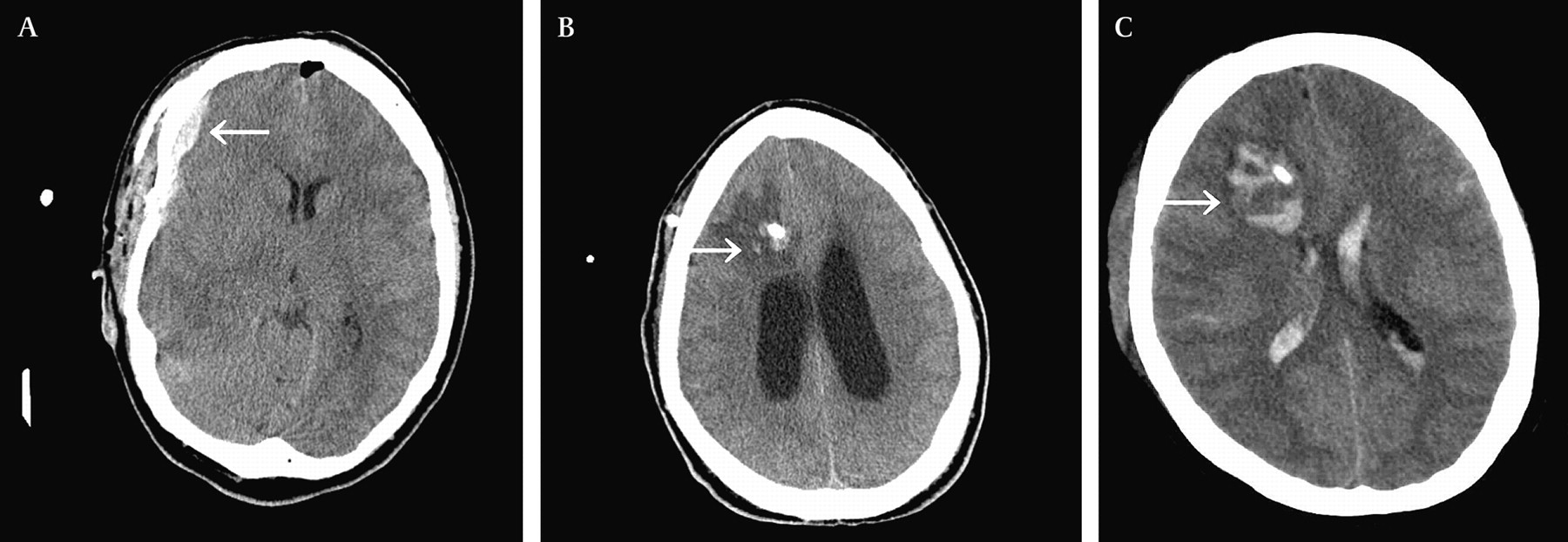
There were three intracranial hemorrhages—two asymptomatic and one symptomatic (see figure 4 and table 3). There were no aneurysm re-ruptures. There were no hemorrhagic complications in patients treated for vasospasm and no hemorrhagic transformations of ischemic strokes. All patients underwent post-procedure head CT.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Intracranial hemorrhage complications. Patient No 18 underwent clipping of a large terminus aneurysm that was compressing the optic nerve. The procedure was complicated by intraprocedure aneurysm rupture near the aneurysm neck. The patient was treated with emergent stent assisted coiling to secure the aneurysm. Post-procedure head CT showed a small asymptomatic epidural hematoma (arrow) at the craniotomy site (A) which eventually resolved. The patient had been treated with clopidogrel only for the first 12 days and then aspirin was added. Patient No 30 underwent stent assisted coiling of a ruptured right P1 aneurysm that required intravenous tirofiban for in-stent platelet aggregates. Routine head CT performed the following day showed a small amount of asymptomatic right frontal hemorrhage along the ventriculostomy track (B). The patient had been placed on both aspirin and clopidogrel post-procedure and was kept on both medications. Patient No 31 underwent uneventful stent assisted coiling of a ruptured basilar summit aneurysm and was placed on both clopidogrel and aspirin post-procedure. The evening after the coiling, the patient became more difficult to arouse. Head CT showed new right frontal hemorrhage along the ventriculostomy track (C). The intraventricular blood had been present prior to aneurysm treatment. The patient was treated with an emergent craniotomy and clot evacuation. The patient made a good recovery to National Institute of Health Stroke Scale score of 0 and modified Rankin Scale score of 1 at the 3 month follow-up.
There were six other bleeding complications for a rate of 14% (see table 3). One bleeding complication was classified as serious—a femoral artery pseudoaneurysm in an obese patient that required surgical repair. The other five bleeding complications were minor. The vitreal hemorrhage in patient No 41 was likely secondary to the initial hemorrhage but was discovered after the aneurysm coiling because of patient intubation and impaired level of consciousness. Antiplatelet medications were not held or discontinued in patients with bleeding complications.
Secondary outcomes
The distribution of mRS scores is shown in table 4. Only one patient was found to have a 3 month follow-up mRS score and/or NIHSS score that was possibly affected by an ischemic stroke or hemorrhagic complication (patient No 26). This patient had an NIHSS score of 2 for arm drift at follow-up and associated disability that probably led to a 1 point shift on the mRS score (from 2 to 3). Other patients with mRS scores of 3 were related to cognitive effects of the initial subarachnoid hemorrhage and advanced age (patient Nos 29, 35 and 37). The fifth patient with an mRS of 3 was a result of vasospasm infarcts and the vitreal hemorrhages. Deaths were discussed earlier.
Modified Rankin scale scores at 3 months
Deaths
There were six deaths during the 3 month clinical follow-up period. None of the deaths was directly related to stent placement, either as a result of a bleeding complication or ischemic stroke. Four deaths (patient Nos 21, 36, 40 and 42) were related to a decision to withdraw care. In three of these four patients (patient Nos 36, 40, and 42), the decision to withdraw care was related to the initial high grade hemorrhage (Hunt and Hess grade IV or V). One of these patients did suffer an ischemic stroke related to stent placement (patient No 42) but the patient's clinical examination was a result of the initial injury from the subarachnoid hemorrhage. In one of these four patients, the decision to withdraw care was related to severe acute respiratory distress syndrome (patient No 21). Two patients died of other medical complications (patient Nos 16 and 30): one patient who had chronic hepatic cirrhosis from hepatitis C died of acute liver failure on hospital day 4 (patient No 16) and another patient who developed sepsis and myocardial infarction died of cardiac arrest on hospital day 23 (patient No 30).
Aneurysm follow-up
Six month angiography was performed on 34 patients. Six patients did not have angiographic follow-up because they died during their initial hospitalization; two patients were followed-up at outside institutions; two patients refused follow-up; and one patient died from a pulmonary embolism after the 3 month follow-up but before the 6 month follow-up (patient No 35). Six patients (17.6%) required retreatment (patient Nos 1, 4, 13, 18, 27 and 34). There were no aneurysm re-ruptures in follow-up.
Discussion
The success of treating acutely ruptured intracranial saccular aneurysms with stent assisted coiling relies on several factors. Firstly, the operator needs to have sufficient experience with stent assisted coiling techniques in order to obtain high technical success (100% in our cohort). If the aneurysm cannot be selected and coiled after stent deployment, then the patient will need to be on double antiplatelet agents with an unsecured aneurysm.
Secondly, a GP IIb/IIIa inhibitor needs to be readily available, frequent runs need to be performed to check for the development of platelet aggregates and the operator needs to be able to administer the GP IIb/IIIa inhibitor as soon as platelet aggregates are seen to form within the stent. Twenty-nine per cent of patients in our cohort developed in-stent platelet aggregates. All but one case was successfully treated with a GP IIb/IIIa inhibitor without clinical evidence of ischemic stroke and one intracranial hemorrhage that was asymptomatic. This high rate of in-stent thrombus formation in the absence of pretreatment with double antiplatelet agents is similar to early reports. Fiorella and colleagues11 described a subgroup of six patients with ruptured aneurysms who underwent Neuroform stent assisted coiling in the absence of antiplatelet pretreatment and/or an intraprocedural GP IIb/IIIa inhibitor bolus dose. Three out of five of these patients who underwent post-procedure MRI had acute infarcts on diffusion weighted sequences, and one patient with an initially normal MRI later developed in-stent thrombosis. Future strategies to reduce the incidence of in-stent thrombus formation include loading the patient with clopidogrel several hours prior to a planned stent assisted coiling procedure.21 Aspirin, which has a rapid onset of action, could be given just prior to stent deployment.22 In our cohort, an attempt to primary coil the aneurysm was generally undertaken and then a decision was made to use a stent during the procedure. In this approach, pretreatment with antiplatelets was not possible unless the procedure was rescheduled for several hours later.
Thirdly, patients need continuous management of antiplatelets during their hospitalization. In our cohort, several patients had systemic bleeding complications, thrombotic complications (eg, pulmonary embolism or deep venous thrombosis) and/or invasive procedures that could require alterations in the antiplatelets regimen. In our cohort, there were several patients who were managed with a single antiplatelet because of clinical concern for increased bleeding risk. In the event of a need for anticoagulation (eg, pulmonary embolism), we stopped one antiplatelet agent. Additionally, we would not hold the antiplatelets for non-CNS invasive procedures such as gastrostomy tubes and tracheostomies but did hold one antiplatelet agent prior to ventriculoperitoneal shunts. In the future, platelet function assays may serve to help manage the antiplatelet regimen and balance the bleeding risks versus ischemic stroke risks post-procedure.22 23 Since the prevalence of aspirin or clopidogrel resistance may be between 5% and 30%,24 the platelet function assay may help determine which antiplatelets should or should not be held.
Neuroform stent assisted coiling of ruptured intracranial aneurysms has been described within a few other cohorts.9 11 15–17 Benitez and colleagues9 described 48 patients treated with Neuroform stent assisted coiling, 16 of which were ruptured aneurysms. The clinically significant ischemic stroke rate was 12.5% (two out of 16 patients) for ruptured aneurysms and 6.25% (two out of 32 patients) for unruptured aneurysms, consistent with a higher risk of ischemic stroke for ruptured aneurysms.
Katsaridis and colleagues16 described a subgroup of 33 patients with acutely ruptured aneurysms treated with Neuroform stent assisted coiling, none of whom had ischemic stroke or serious bleeding complications. There was also only one in-stent thrombus successfully treated with tissue plasminogen activator. Their strategy included 5000 IU of intravenous heparin with 1500 IU every 1.5 h for an activated clotting time of 200, 2500 IU heparin at completion of the procedure, nadroparin at completion of the procedure and for 3 days, and clopidogrel 75 mg and aspirin 100 mg at the end of the procedure or the following morning. This differs from our approach which included less aggressive heparinization, use of tirofiban to treat platelet aggregates when present and earlier administration of antiplatelets with a loading dose of clopidogrel.
Tumialan and colleagues20 reported a high rate of symptomatic intracranial hemorrhage complications in patients (six out of seven patients) who had undergone stent assisted coiling of ruptured intracranial aneurysms and also had external ventricular drains (EVDs) and/or ventriculoperitoneal shunts placed. This differs from our rate (one out of 17 patients). This may in part be explained by their inclusion of two patients who experienced aneurysm re-rupture due to incomplete aneurysm coiling whereas all patients in our cohort had 90% or greater aneurysm treatment. Additionally, they included an elective aneurysm stent assisted coiling case associated with periprocedure rupture.
An alternative strategy to reduce the risk of intracranial hemorrhage and/or ischemic stroke complications may be to first primary coil the aneurysm rupture site and then stage the stent assisted coiling of the aneurysm remnant after the patient is clear of needing an EVD or ventriculoperitoneal shunt. This strategy may be preferable if it is clear where the aneurysm rupture site is and if it can be adequately secured; however, it may not always be clear where the aneurysm rupture site is. Our cohort included only one such patient where staging the stent assisted coiling was performed. More outcome data on this strategy are warranted to ensure that there is not a high aneurysm re-rupture rate.
Conclusions
Our data suggest that Neuroform stent assisted coiling of acutely ruptured intracranial aneurysms and use of double antiplatelet agents carries a higher risk in patients with Hunt and Hess grades III–V and in patients with EVDs than in those with Hunt and Hess grades I–II. However, our cohort showed that these complications did not have a major impact on long term outcome. Better ways to reduce these risks warrant further study.
References
Footnotes
Competing interests JCC is a consultant for Boston Scientific and has received honoraria for proctoring Neuroform stent cases.
Ethics approval This study was conducted with the approval of the the institution's internal review board.
Provenance and peer review Not commissioned; not externally peer reviewed.