Article Text

Abstract
The artery of Percheron (AOP) is a rare anatomic variant of the paramedian thalamic–mesencephalic arterial supply, arising as a solitary arterial trunk from the P1 segment of the posterior cerebral artery. Its occlusion, commonly caused by cardioembolism, leads to distal bilateral paramedian thalamic ischemia, oftentimes affecting the midbrain and/or the anterior thalamus. AOP occlusion presents with a clinical triad of altered mental status, vertical gaze palsy, and memory impairment, along with other associated symptoms. Digital subtraction angiography is effective for detecting AOP, while diffusion weighted MRI is best for diagnosis of its occlusion. Our extensive literature search sought to determine the best forms of treatment for uncomplicated AOP occlusion, with the inclusion criterion of implementation of medical treatment or other forms of therapy in patient recovery from this condition. We conclude that intravenous heparin and thrombolysis with tissue plasminogen activator are effective firstline treatment options for emergent AOP occlusion followed by a prescription of long term anticoagulants, while non-emergent cases without midbrain involvement could be treated through rehabilitation and continual monitoring by medical staff. Clinical trials of higher power are needed for a more comprehensive analysis of the treatment options for AOP occlusion.
- Thrombolysis
- Thrombectomy
- Stroke
Statistics from Altmetric.com
Introduction
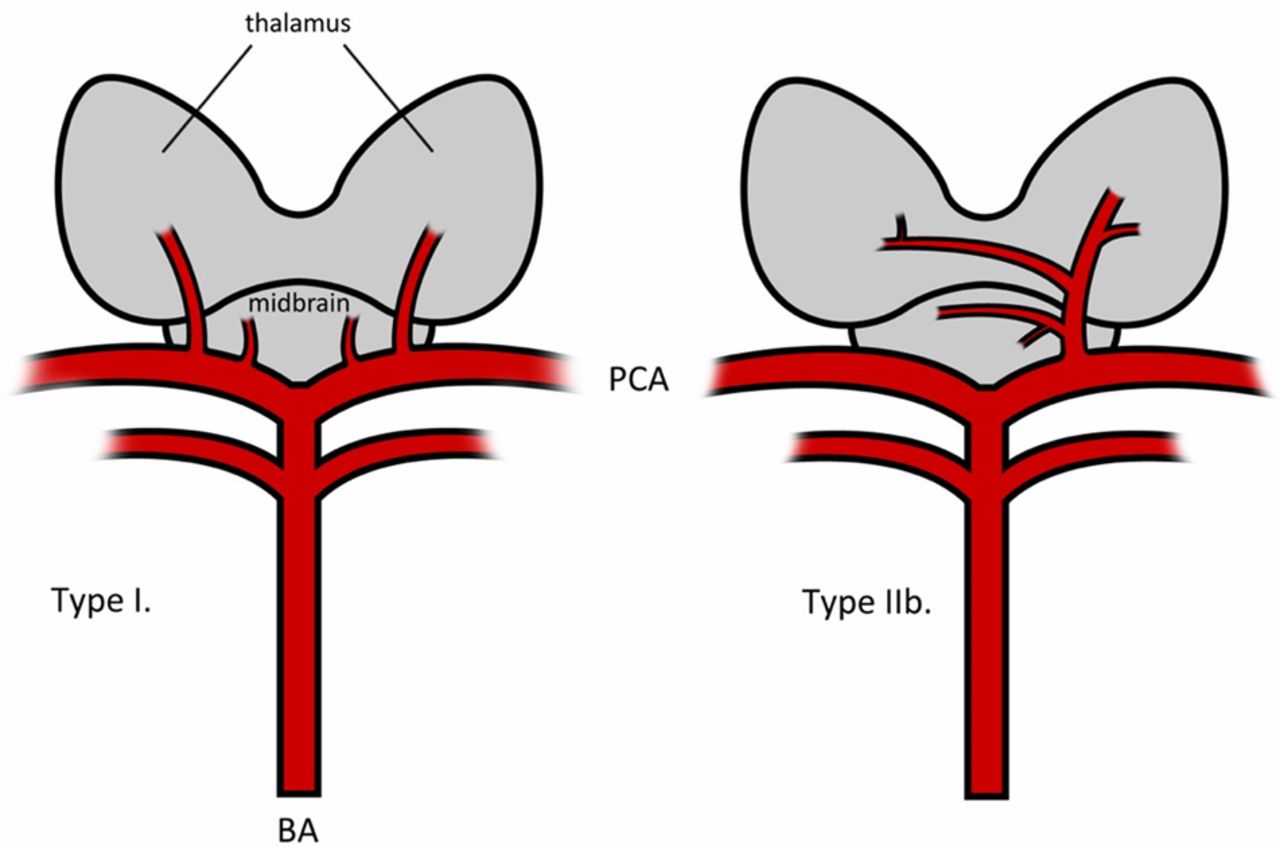
First described in 1973, the artery of Percheron (AOP) is a rare anatomic variant of the paramedian thalamic–mesencephalic arterial supply, arising as a solitary arterial trunk from the P1 segment of the posterior cerebral artery (PCA) (figure 1). It is the primary blood supply of the paramedian territory of the bilateral thalami and the rostral midbrain.1 Interruption of flow to the AOP leads to distal bilateral ischemia of the paramedian thalamic territory and oftentimes the midbrain (57%) and/or the anterior thalamus (19%).2 Because this one artery, in essence, serves the function of the thalamic and midbrain perforators that arise directly from the PCA in the majority of the population, its occlusion would cause more severe functional impairment than occlusion of any one of the perforators alone in a patient with the more common variant. These impairments include cognitive and motor deficits, and could lead to coma if left untreated. AOP infarction accounts for only 0.1–0.3% of all ischemic strokes and 4–18% of thalamic infarctions, but its overall incidence has not been described in the literature.3 ,4 Thorough analyses of treatment options for other arterial occlusions have been performed, but never for this condition. Here we present an evidence-based treatment algorithm for optimal management of AOP occlusion.
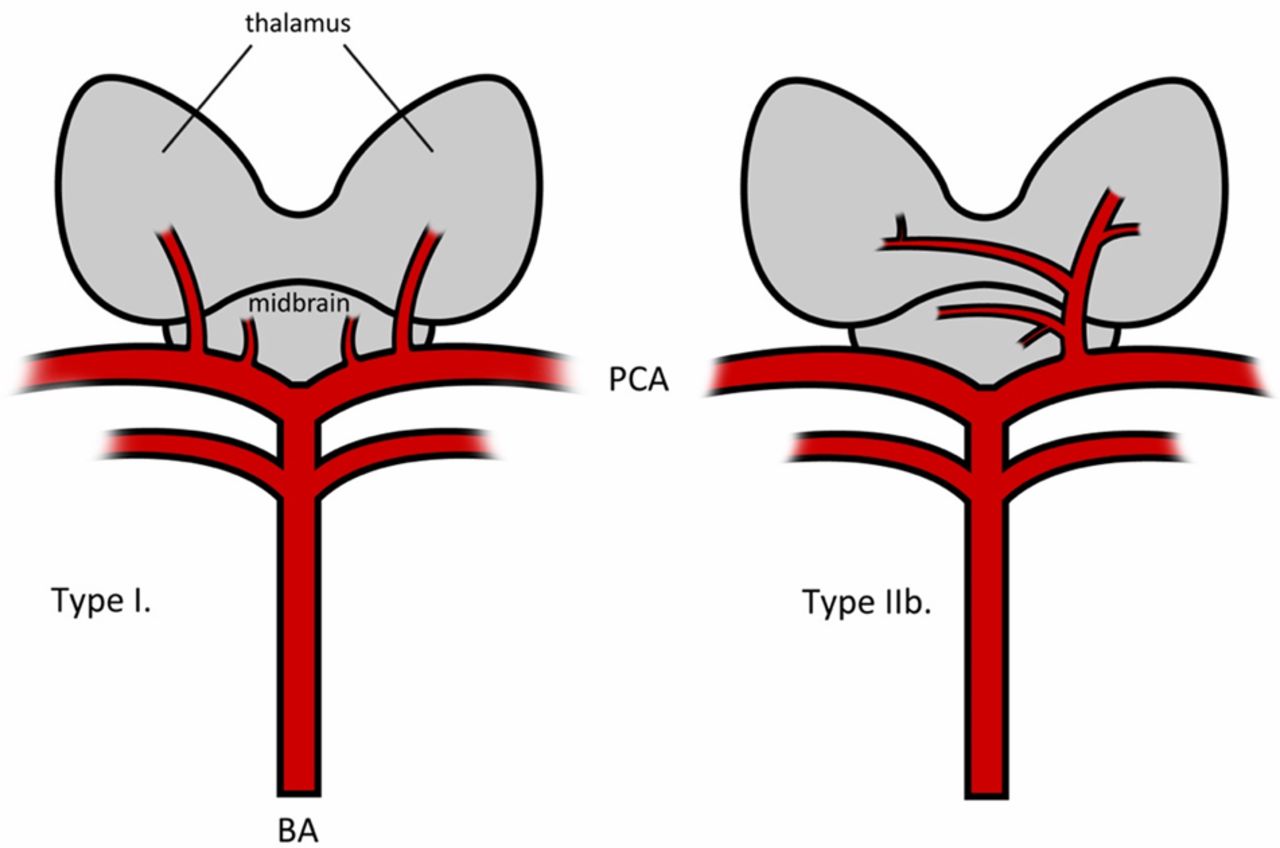
Thalamic arterial supply. Type I: Most common vascular anatomy, with perforating arteries branching directly from the PCA to supply the thalamus and midbrain. Type IIb: Artery of Percheron (AOP) variant, with the AOP arising from the PCA as a single trunk before branching to supply the bilateral paramedian thalami and the rostral midbrain. BA, basilar artery; PCA, posterior communicating artery.
Etiology
AOP occlusion is most frequently caused by microangiopathy and cardioembolism from plaque buildup or lipohyalinosis.5–8 The proximity of the AOP to the basilar apex may explain the high frequency of cardioembolism as a cause of arterial occlusion, resulting in bilateral thalamic infarcts.9 Increased occlusion risk includes systemic or internal cerebral hypertension, diabetes mellitus, and atrial fibrillation (table 1).2 ,5–7 ,10 ,11 Buildup of microatheromatous plaques near the mouth of the paramedian artery can contribute to microangiopathy and thus AOP occlusion.
Causes and triggers of artery of Percheron occlusion
Obstruction of the AOP can also have a hemodynamic etiology. Systemic hypotension, distal ischemia in the posterior circulation from non-laminar basilar artery blood flow, top of the basilar artery aneurysms, or clots within these aneurysms can block the paramedian arteries.12 In some cases, AOP occlusion arises as a postprocedural complication after coiling of a basilar tip aneurysm13 or through embolism of the heart after cardiac catheterization.14
Presentation
Clinical presentation of the bilateral paramedian thalamic ischemia resulting from AOP occlusion often consists of a triad of altered mental status, vertical gaze palsy, and memory impairment.11 ,15 Change in mental status is due to involvement of the reticular activating system and can be further classified into hypersomnia, disorientation, dysarthria, or coma. Vertical gaze palsy is frequently characteristic of mesencephalic or thalamic involvement, with the latter having a role in cortical input processing to the rostral interstitial nucleus of the medial longitudinal fasciculus.16 When the anterior thalamic region is also affected, memory impairment is typically more severe. If midbrain involvement is present, the clinical presentation will usually be characterized by hemiplegia, movement disorders, cerebellar ataxia, and other oculomotor disturbances in addition to the aforementioned triad (table 2).2 Other symptoms include akinetic mutism, dysprosody, and hypophonia.14 ,17 ,18 Rare behavioral disturbances, such as long term delusions of jealousy, can also result.19 The frequencies of clinical signs for this condition have not yet been documented.
Clinical signs and symptoms of artery of Percheron occlusion based on location of infarct
Imaging
Conventional angiography usually does not permit visualization of the Percheron arterial variant because of its small size, although digital subtraction angiography is an effective commonly used angiographic technique for detecting AOP.2 ,11 Diagnosis of AOP infarction is best made using diffusion weighted MRI. On axial diffusion weighted imaging or fluid attenuated image recovery imaging, midbrain involvement in AOP occlusion manifests as a hyperintensity along the pial surface of the interpeduncular fossa in 67% of patients, termed by Lazzaro et al as the ‘V’ sign after its characteristic shape.20
Methods
In November 2013, a literature search was performed on PubMed and the Cumulative Index to Nursing and Allied Health Literature to obtain case reports, reviews, and retrospective studies of AOP occlusion with treatments involved in its resolution. Key subject terms used AOP, infarction, occlusion, bithalamic stroke, and top of the basilar syndrome. Each of these terms was then combined with a key term related to treatment: thrombolysis, thrombolytic therapy, thrombectomy, heparin, anticoagulation, treatment, and therapy. The inclusion criterion was implementation of medical treatment or other forms of therapy in patient recovery from AOP occlusion, with exclusion of articles written in a language other than English. Additional cases and background were obtained through cross referencing. Each combination of the subject and treatment terms was utilized in our search, and all relevant articles and cases were included in the formulation of the AOP treatment algorithm in this review.
Treatment options
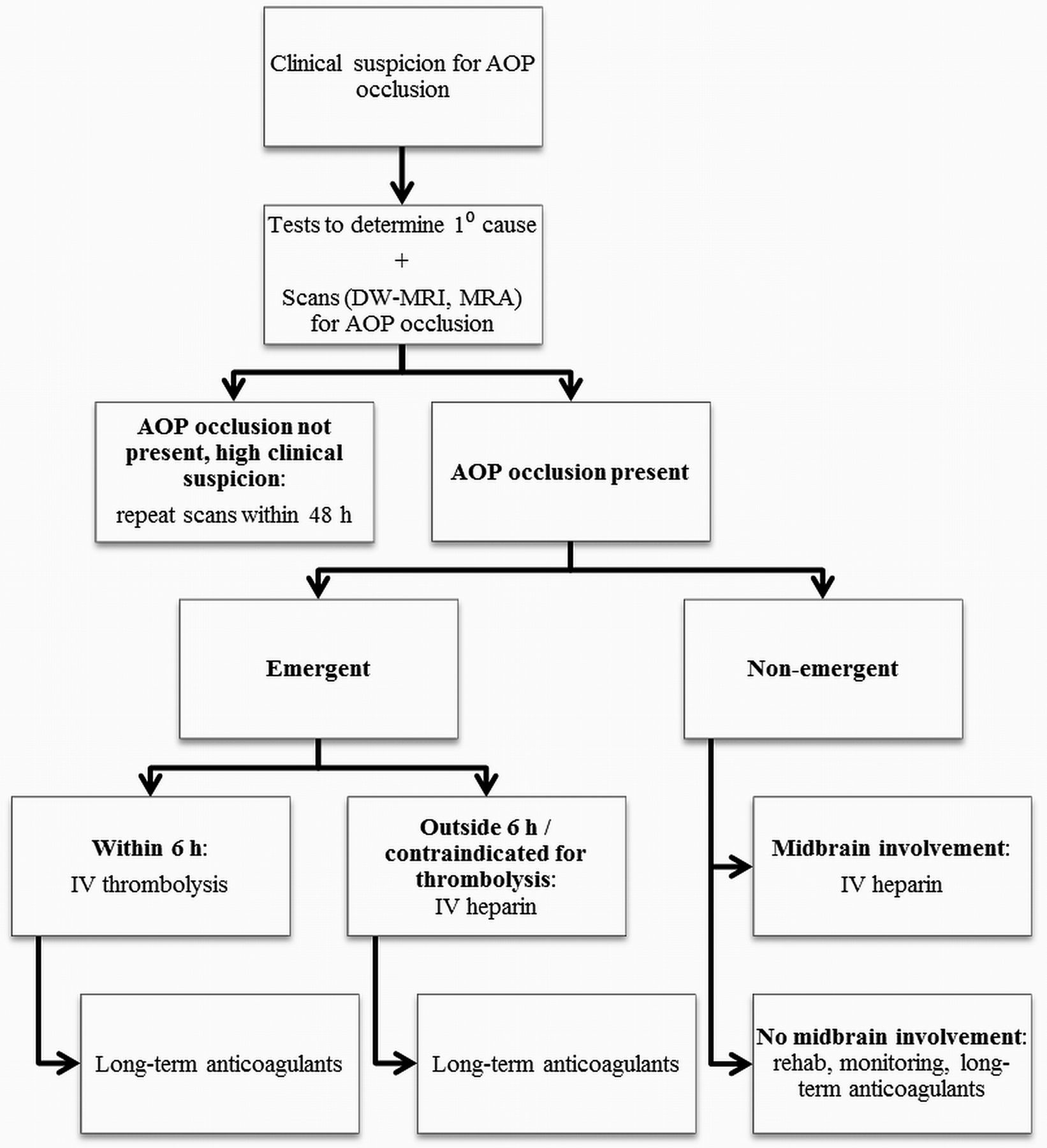
Because of the rarity of AOP occlusion and the relatively few number of documented cases (table 3) that administered medical or surgical treatment, we propose an evidence-based standardized treatment algorithm for AOP occlusion. Current objectives of a treatment regimen for AOP occlusion are to promote recanalization as soon as possible and to prevent future episodes. Thrombolysis and heparin have been used for the former and general anticoagulants for the latter. Here we present evidence for a treatment algorithm for AOP occlusion once clinical suspicion is high or has been confirmed radiographically (figure 2), one that is much in line with the 2013 guidelines from the American Heart Association/American Stroke Association on fibrinolytic and surgical management for acute ischemic strokes.21
Documented cases of treated artery of Percheron occlusion with clinical outcome. Thrombolysis and anticoagulants, especially heparin, are currently the most utilized forms of medical therapy
{kind=link}
{kind=link}
Algorithm for the treatment of artery of Percheron (AOP) occlusion. DW, diffusion weighted; MRA, MR angiography.
Emergent: thrombolysis
The small therapeutic window (4.5–6 h) of thrombolytic therapy, currently the most effective treatment for AOP occlusion, necessitates the importance of immediate diagnosis to maximize efficacy and minimize risk.11 ,22 ,23 The first known case of treated AOP occlusion proven by angiography was treated with tissue plasminogen activator thrombolysis delivered via catheterization, resulting in full patient recovery with residual absence of upgaze and downgaze, and skew deviation.24 In another more recent case, thrombolysis with tissue plasminogen activator with an unspecified route of delivery was administered within 6 h based solely on clinical presentation of sudden loss of consciousness with no acute infarctions on CT. This treatment led to immediate improvement in the Glasgow Coma Scale score, from unspecified sudden onset of unconsciousness to 15. Upon discharge, the patient was fully conscious although with severe cognitive impairment.11
As with treatment of other arterial infarctions, thrombolytic therapy should be avoided in patients with cerebral hemorrhage found within 3 h or edema present on CT or MR.17 ,25 There have been no documented reports of patients contraindicated for thrombolytic therapy because of hemorrhagic bleeds.
Emergent: alternative treatments
In one case documented by Cassourret et al, diagnosis of ischemic stroke due to AOP occlusion was made after the therapeutic window, complicated by the finding of a normal initial MRI. Intravenous heparin on day 2 after onset of unconsciousness, dysarthria, and other neurological abnormalities proved effective, and the patient was discharged with marked cognitive and motor improvement but still with partial memory deficit.22 Heparin has also been used post-recanalization with thrombolysis.24 Mechanical thrombectomy has been utilized to effectively treat other cerebral arterial occlusions, but usage has not yet been documented for AOP occlusion.26
Non-emergent
In many non-emergent cases, patients are placed in rehabilitation centers and monitored for signs of clinical and radiographic improvement.3 If left untreated, AOP occlusion can lead to persistence of neurological deficits or recurrence, which can be a potentially fatal event.3 ,17 However, even without treatment, prognosis is significantly better if the midbrain is unaffected, which is the case in 43% of AOP occlusion cases.2 ,10 ,14 ,16 Unspecified oral anticoagulants have been prescribed to patients after full or partial recovery to prevent future episodes.10 ,22
Further clinical studies and systematic case reports on patients with AOP occlusion are needed to further elucidate factors to determine the optimal management of this condition, although large scale studies may be difficult due to its rarity. Doing so would provide insight into the therapeutic window of thrombolysis, benefits and risks of injected versus small catheter thrombolytic therapy, the efficacy of intravenous heparin in cases of non-emergent AOP occlusion or if the therapeutic window of thrombolytic therapy had passed, and the utility of long term anticoagulants in the prevention of recurrence.
Conclusion
AOP is a rare unique anatomical variant that combines the function of midbrain and thalamic perforators that branch directly off the PCA, leading to a variety of neurological deficits that could cause severe functional impairment or even coma if left untreated. The scarcity of documented treated cases of AOP occlusion is most likely attributed to the rarity of AOP in the population, and thus development of treatment options is still in progress. The authors conclude that as of this writing, thrombolysis and intravenous heparin are effective firstline treatment options for emergent uncomplicated AOP occlusion followed by prescription of long term anticoagulants, while non-emergent cases without midbrain involvement could be treated through rehabilitation and continual monitoring by medical staff. With an average diagnosis delay of 7 days, AOP occlusion requires immediate diagnosis and treatment initiation for a more favorable prognosis.4 Systematic case reports and clinical trials of higher power are needed for a more comprehensive analysis of AOP occlusion treatment options.
References
Footnotes
-
Contributors NA, CJP, and CDG were involved in the design and conception of this manuscript. XL and NA performed the literature search and compiled the primary manuscript. DRH, CJP, and CDG critically revised the manuscript. All authors have approved the manuscript as it is written.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-