Article Text

Abstract
Background and purpose Combined analysis of the Interventional Management of Stroke I and II trials demonstrated a significant association between microcatheter contrast injections and both intracranial hemorrhage (ICH) and contrast extravasation following combined intravenous (IV) and intra-arterial (IA) thrombolysis. The reliability of these observations was tested in our local registry of IA cases.
Design/methods Treatment angiograms and post-procedure CTs of patients treated with combined IV/IA or IA only recombinant tissue plasminogen activator for ICA-T, M1 or M2 occlusions (n=77) were reviewed. The number of microcatheter injections (MCIs) within/distal to the target occlusion was assigned for every case. The association of MCIs to total ICH, total parenchymal hematoma (PH1+PH2) and PH2 after adjusting for significant covariates was tested.
Results MCIs were used in 21 (27%) cases (range MCI 0–6). Any ICH occurred in 38 (49%) cases, including eight (10%) PH1s and eight (10%) PH2s. The use of MCIs was associated with increased PH (p=0.04), PH2 (p=0.07) and total ICH (p=0.03). MCIs were associated with increased contrast extravasation (CEx) (p=0.02). ICH was observed in all CEx cases (n=5, 100% vs 46% non-CEx; p=0.03), and four (80%) CEx cases developed PH2s (p<0.01). MCIs remained associated with total ICH after adjustment for significant covariates of Thromolysis in Cerebral Infarction score, glucose level and presence of atrial fibrillation (OR 3.60; 95% CI 1.12 to 11.49, p=0.03). MCI use was the only significantly associated covariate for total PHs.
Conclusions MCI use was associated with ICH and with clinically significant PHs in this cohort, providing further evidence that MCIs be reduced during IA thrombolysis.
Statistics from Altmetric.com
Introduction
According to the American Heart Association/American Stroke Association guidelines in 2007, intra-arterial (IA) thrombolysis is an option for treatment of selected patients who have major strokes of <6 h duration due to occlusions of the middle cerebral artery and who are not otherwise candidates for intravenous recombinant tissue plasminogen activator (rt-PA).1 Suzuki et al reported that 99% of the US population had access to neurointerventional treatment within 6 h2 and in a recent analysis, US estimates of rt-PA use for ischemic stroke patients was estimated to be 1.8–2.1%.3
One of the major complications of IA thrombolysis is hemorrhagic transformation with neurological deterioration, observed in 10–15.4% of cases.4 There are several studies in the literature examining factors for prediction of hemorrhagic transformation during revascularization therapy. However, not many have systematically evaluated the technical aspects of the procedure. Microcatheters are used during thrombolysis for drug delivery. Contrast agent is usually given by guide catheter to monitor the results of the procedure but it can also be given by microcatheter to identify proximal thrombus, confirm catheter placement within the thrombus or visualize the vasculature distal to the occlusive thrombus. Many, if not most, procedures do not require microcatheter injections (MCIs) for IA thrombolysis. Procedures may have several MCIs performed due to inadequacy of guide catheter injections or because of the preference of neurointerventionalist. For mechanical thrombectomy with the MERCI device, a selective angiogram via an MCI is recommended to confirm device placement distal to the clot prior to its attempted retrieval using the same microcatheter.5
In the European Cooperative Acute Stroke Study (ECASS) trial analyses, among all the intracranial hemorrhage (ICH) subtypes, parenchymal hematoma types 1 and 2 (PH1 and PH2) were associated with an increased risk for neurological deterioration at 24 h after stroke onset.6 Khatri et al, in a retrospective analysis of the Interventional Management of Stroke (IMS) I and II trials suggested that MCI use is associated with a greater odds of ICH, and also identified a potential link between MCIs and contrast extravasation (CEx).7 We not only sought to test the reproducibility of these relationships but also to look specifically for a relationship between MCI and clinically significant PH. Our hypothesis was that use of MCI is associated with ICH, including PH in particular, and CEx.
Methods
Patient selection and intervention
We retrospectively reviewed a total of 77 non-randomized, non-study patients with acute ischemic stroke with ICA-T, M1 or M2 occlusions treated with a combined intravenous (IV)/IA or IA only approach between May 1999 and November 2005 at the University Hospital and Good Samaritan Hospital, Cincinnati, Ohio, USA. This retrospective analysis was approved by each institution's institutional review board. Inclusion criteria for IV/IA therapy were the same as used in the National Institute of Neurological Disorders and Stroke rt-PA Stroke Trial8 plus an National Institutes of Health Stroke Scale (NIHSS) score of ≥10. Combined treatment consisted of IV rt-PA (0.6 mg/kg, 60 mg maximum,10–15% bolus over 1 min with the remainder over 30 min) followed by immediate cerebral angiography and up to 22 mg of additional IA rt-PA delivered locally or regionally over 2 h. Cerebral angiogram was performed, and thrombolysis by the IA route was used only if thrombus was seen; otherwise, the procedure was terminated. IA rt-PA therapy alone was considered if IV tPA was contraindicated (eg, presentation between 3 and 6 h of symptom onset) or if systemic thrombolysis was considered unsafe by the treating stroke physician (eg, recent surgery).
Data analysis
All angiograms and post-procedure CT scans were reviewed (TT, RK). The number of MCIs documented at or distal to the occlusion was recorded for each case. All post-procedure CT scans were reviewed for CEx and ICH. CEx was defined as hyperdensity suggestive of contrast (Hounsfield unit >90) seen within 24 h, and persisting with, or replaced by, ICH at 24 h. CEx was differentiated from contrast enhancement where the hyperdensity (irrespective of CT numbers) on CT scan clears within 24 h.4 Angiographic reperfusion for IV/IA patients was documented using a modified Thrombolysis in Cerebral Infarction (TICI) Scale (0=no perfusion; 1 and 2=partial perfusion without and with any distal branch perfusing with cortical staining, respectively; 3=full reperfusion with all distal branches filling, including M3, 4). Recanalization was measured using Arterial Occlusive Lesion (AOL) score (0=no recanalization; 1 and 2=partial recanalization without or with distal flow, respectively; 3=complete recanalization with any distal flow).9 We categorized ICHs radiologically by ECASS criteria as HI (hemorrhagic infarct) and PH (parenchymal hematoma). HI type 1 (HI-1)=small petechiae along the margins of the infarct; HI type 2 (HI-2)=more confluent petechiae within the infarcted area but without space occupying effect; PH type 1 (PH-1)=hematoma in ≤30% of the infarcted area with some slight space occupying effect; PH type 2 (PH-2)=dense hematoma in more than 30% of the infracted area with substantial space occupying effect or as any hemorrhagic lesion outside the infarcted area.6
Statistical analysis
Statistical analyses were performed using SAS statistical software, V.9.1. Two multivariable analyses were performed; an ICH prediction model and a PH prediction model. For each model, variables were tested bivariately for association with the outcome of interest using either a t test or Wilcoxon rank sum test for continuous variables and χ2 or Fisher's exact test for categorical variables. The variables of interest were: use of MCI, age, baseline NIHSS, race, gender (female), serum glucose at the time of presentation, history of diabetes mellitus, atrial fibrillation, hypertension, prior antiplatelet use, AOL 0–3 score (recanalization) and TICI 0–3 score (reperfusion) (see table 1).
Variables of interest
Variables significant (p<0.25) in bivariate analysis were considered as potential covariables in logistic regression analyses. A backward elimination approach was used to find the most parsimonious model, and then variables were re-entered into the model individually to assess their effects on the independent variable of interest. The associations of CEx with MCI and ICH were assessed using Fisher's exact test due to the small number of subjects with CEx. Actual p values for these particular analyses are presented, however, for statistical significance. A Bonferroni correction must be applied for the comparison of CEx with ICH, PH and PH2; those with p<0.016 are considered statistically significant.
Results
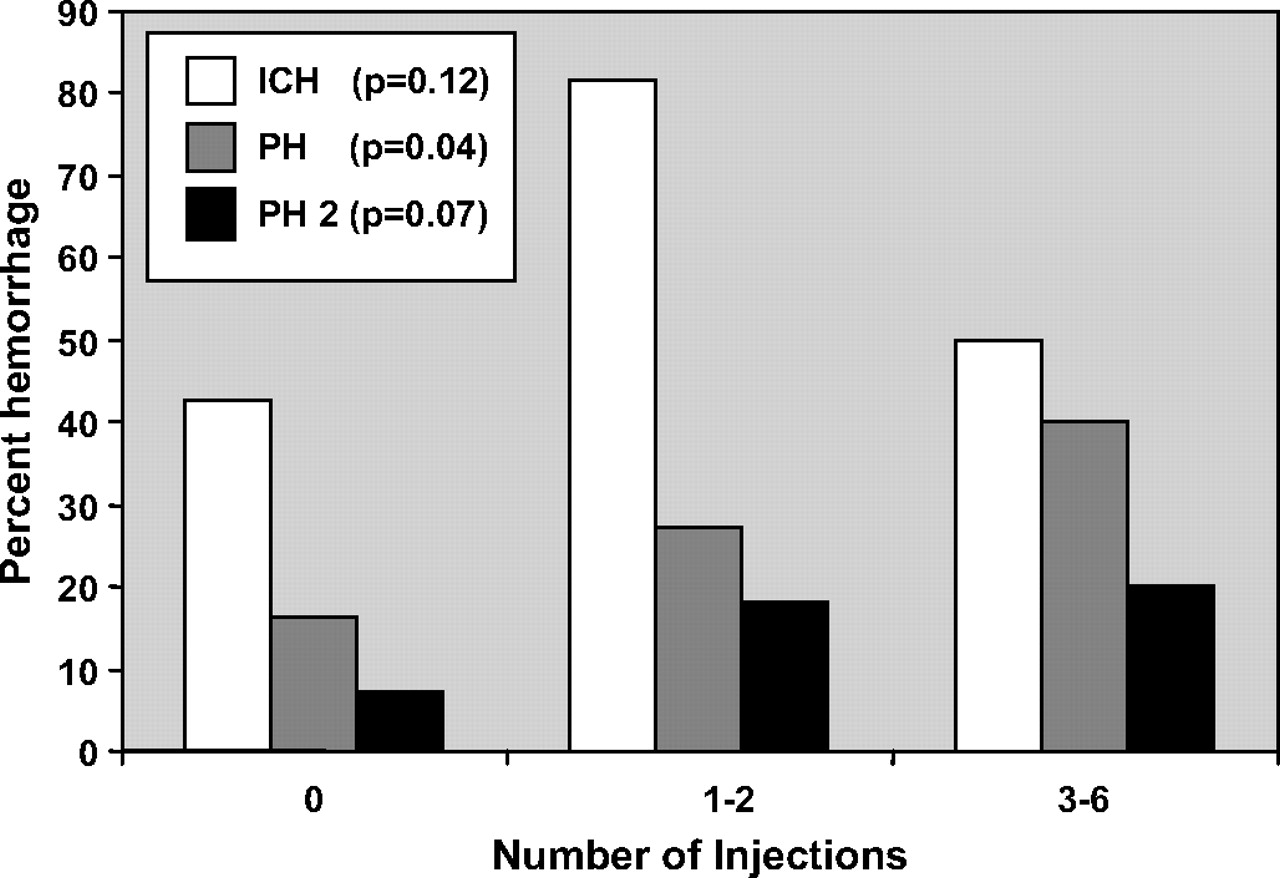
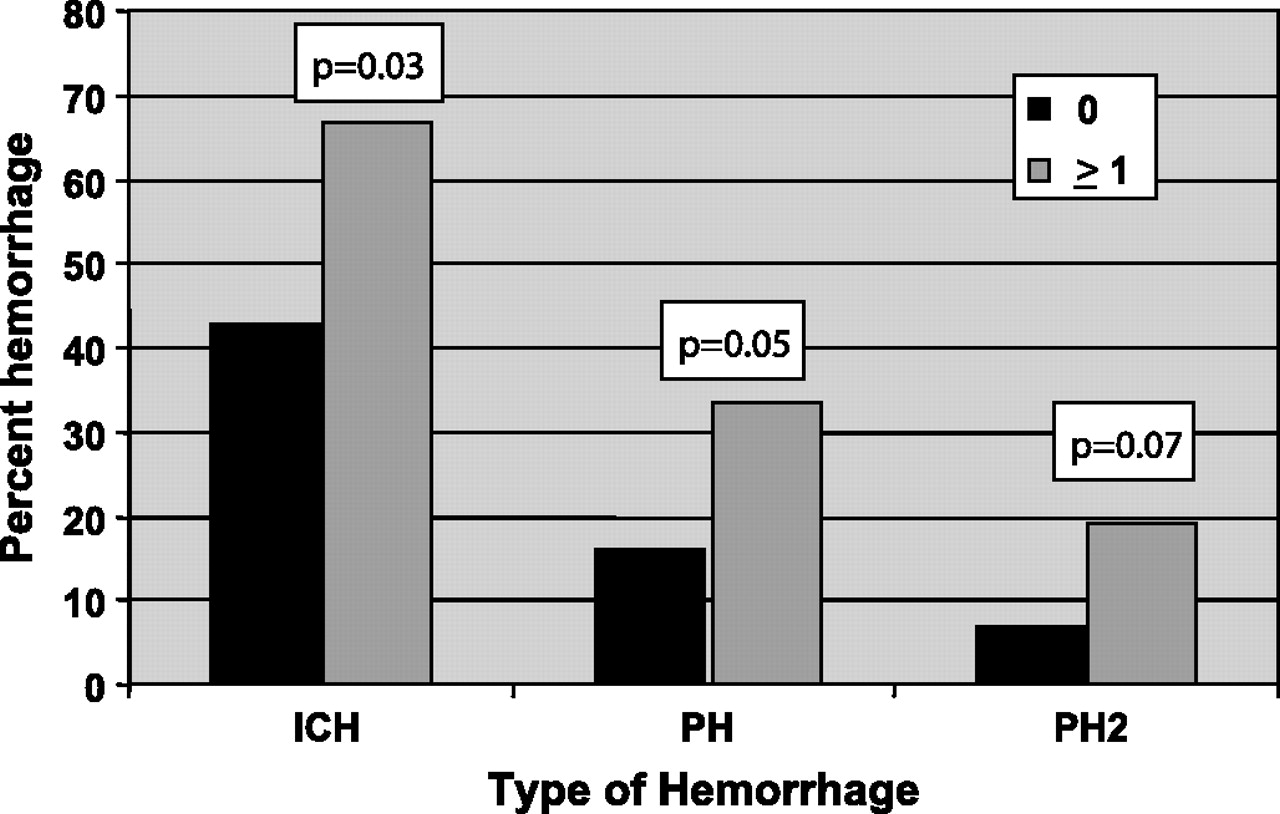
The descriptive statistics for the population are shown in table 1. Outcomes for the cohort are given in table 2. MCIs were used in 21 (27%) cases (range 0–6, 1–2 in 11 patients, 3–6 in 10 patients). ICH occurred in 38 (49%) cases, including eight (10%) PH1s and eight (10%) PH2s. In univariate analysis the use of any MCI was associated with increased total ICH (p=0.03), PH (p=0.04) and PH2 (p=0.07) (figure 1). This association was confirmed by increased overall PH and PH2 with increasing number of MCIs; however this was not seen for total ICH (figure 2). Using multiple logistic regression (table 3), the independent variables associated with an increased odds of ICH were use of MCIs, serum glucose and TICI reperfusion (0–3), and atrial fibrillation was of borderline significance. Use of MCIs remained associated with total ICH after adjustment for these significant covariables. MCI was also the only factor significantly associated with PH.
Outcomes of cohort

ICH and PH were associated with use of MCI (≥1, light bar) compared to no MCI (0, black bar). A strong trend toward correlation with (p=0.07) also existed.
{kind=link}
{kind=link}
PH was associated with the number of microcatheter injections. A strong trend toward correlation with (p=0.07) also existed.
Independent risk factors for intracranial hemorrhage in multivariable analysis
MCIs were also associated with increased CEx (p=0.02). ICH was observed in all CEx cases (n=5, 100% vs 46% non-CEx; p=0.03), and four (80%) CEx cases developed PH2s (p=0.01). Of five cases with CEx, four had MCI (p=0.02) (table 4).
Relationship of contrast extravasation and intracranial hemorrhage
There were no differences between IV/IA and IA only treatment with respect to MCIs, ICH or PH.
Discussion
We retrospectively analyzed the association between MCIs and both ICH and CEx. To our knowledge, this is the second detailed analysis of this kind. Use of MCIs was significantly associated with both total ICH and PH risk in bivariate analyses. Moreover, this relationship remained significant in logistic regression analysis. Increasing numbers of MCIs were also related to higher risk of PH, the most clinically significant subtype of ICH. Hyperdensity seen on head CT after cerebral angiogram may be blood, contrast extravasation or contrast enhancement. In the literature, the terms contrast ‘enhancement’ and ‘extravasation’ have been used interchangeably. It may be mechanistically important to distinguish between these two entities, as CEx may have a stronger association with ICH. In a grading scale proposed to predict the long term outcome after IA thrombolysis for stroke complicated by contrast extravasation it has been suggested that hyperdensity >150 Hounsfield units and prolonged angiographic blush are markers for poor prognosis.10 In several other reviews, CEx has been proposed as a negative prognostic sign.4 11
Intracerebral hemorrhagic transformation is likely a multifactorial phenomenon involving mainly blood vessel leakage, extravasation and reperfusion injury. Yoon et al comprehensively reviews several mechanisms postulated for CEx and hemorrhage related to contrast agents.4 The most convincing of them implicates potential contrast toxicity on basal lamina, a structural barrier where loss of integrity is associated with disruption of the blood–brain barrier. It results in cellular blood element extravasation from microvessels in association with CEx. In comparison, contrast enhancement is caused by leakage of contrast medium from vessels into the extracellular spaces as a result of increased permeability of the blood–brain barrier. Contrast agents can induce injury to the blood–brain barrier. Even though non-ionic contrast agents were deemed to be safer than ionic agents in one animal study,12 another animal study confirmed that even non-ionic agents cause blood–brain barrier disruption. Proposed mechanisms include osmolality change, increased pinocytosis and inherent chemotoxicity.13 At the molecular and biochemical level, loss of microvascular integrity and disruption of neurovascular homeostasis results from oxidative stress, leukocyte infiltration, vascular activation and dysregulated extracellular proteolysis (by matrix metaloproteinases).14 Notably, hyperglycemia and lower TICI score (decreased reperfusion) were statistically significantly associated with an increased odds of ICH in our multivariable analysis.
Hyperglycemia has also been previously described as a risk factor for symptomatic ICH. In exploratory analysis of the Prolyse in Acute Cerebral Thromboembolism II (PROACT II) trial, blood glucose >200 mg/dl was the only significantly associated factor with symptomatic ICH in r-proUK treated patients in a univariate analyses.15 Two large registry experiences with IV thrombolytics also substantiate association of serum glucose or diabetes mellitus as an independent predictor for ICH.16 17 It has been proposed that glucose may accelerate blood–brain barrier disruption by increasing matrix mettaloproteinase-9 expressions (protelolytic enzyme degrading basal lamina) Moreover, it induces a pro-oxidative and proinflammatory state that can cause direct neuronal toxicity, and a procoagulant state, further compromising blood supply to the penumbral areas in acute ischemic stroke.18 Others have suggested that late reperfusion may be associated with a higher risk of total ICH.7 19 We have insufficient late post-procedure perfusion data to prove the hypothesis. Even though TICI reperfusion and AOL recanalization scores seem to be in modest agreement, AOL scores were not associated with ICH risk. The reason for this relationship is not clear but it may be related to an increase in ischemia due to limited distal perfusion despite modest proximal recanalization and thus predisposing it for hemorrhage and reperfusion injury when the vessel recanalizes later. In another analysis by Molina et al, thrombolysis related hemorrhagic infarct represented a marker of early successful recanalization and improved clinical outcome compared with parenchymal hematoma which is related to delayed recanalization and poor clinical outcome. This again emphasizes the importance of recognizing the association of MCI and PH observed in our analysis.20
Additional factors that may contribute to hemorrhage are mechanical traumatic injury to the vasculature by the microcatheter or microguidewire itself, or possibly pressure transmission during the actual injection phase. Microcatheters and microguidewires have been used to mechanically disrupt thrombi in the literature. A case series of 23 such cases reported two cases with vessel perforations and two cases with CEx.21
Another notable finding in our registry analysis is the high rate of total ICH (49%) and PH (21%) which we believe may be due to a higher baseline mean NIHSS of 20, the extended therapeutic window or the lack of standardization of IV heparin during thrombolysis. If hyperdensity is seen on head CT after IA reperfusion therapy, Nakano et al reported an overall hemorrhage rate of 55.6% and a symptomatic hemorrhage rate of 29.7% which is comparable with our rates.22 High rates of any ICH have been observed with other interventional trials of acute ischemic stroke such as the Mechanical Embolus Removal in Cerebral Ischemia (MERCI) phase I trial (43%), IMS I (42.5%) and PROACT II (26% at 24 h and 58% at 10 days).23
Contrast material is known to be deposited in the brain during prolonged IA interventions.24 25 It has been identified following thrombolysis, with no significance ascribed.26 27 It has been reported in over 90% of thrombolytic procedures immediately post-procedure, with contrast and/or hemorrhage persisting at 24 h in approximately 50%.28 As noted, others have ascribed significance to its presence.4 7 10 11 This range of observations indicate there is much to learn regarding contrast appearance and significance in the setting of stroke treatment and the injured blood–brain barrier.
Our analysis has several limitations. It is a retrospective analysis of a registry of cases which inevitably introduces patient selection bias. We had only 21 subjects with MCIs which is a relatively small sample size. There were 16 PH, a relatively low event rate. The number of MCIs and CEx for some cases may have been underestimated if all the angiographic runs were not recorded via image or report, thereby being unavailable to the central readers for identification. CEx was determined by visual inspection (instead of strict Hounsfield units) in several obvious cases where only hard copies of head CTs were available. Technical factors such as injection pressure, syringe size, contrast bolus volume and contrast type were not standardized or measured. We also could not measure all of the clinical and imaging variables that have shown association with ICH in prior observations; however, our main aim was to elaborate primarily on this technical aspect of the procedure.
Finally, it should be acknowledged that while complex cases with larger clot burden may have received an increased number of MCIs to delineate the clot or to see the distal vasculature beyond the occlusion site, that was not the general practice of all operators. We considered baseline NIHSS in an attempt to address this issue but did not have access to IA procedure duration or total rt-PA dose to consider this issue further.
Conclusion
Our registry experience suggests that use of MCIs in patients treated with combined IV/IA or IA therapy is significantly associated with ICH and PH risk. We also showed a relationship between MCI and CEx, as well as a relationship between CEx and PH. These observations provide a second set of compelling data to suggest that MCIs should be minimized during IV/IA revascularization procedures whenever possible. This relationship and other technical factors need to be prospectively tested in acute revascularization trials.
References
Footnotes
Competing interests None.
Ethics approval This study was approved by each institution's institutional review board.
Provenance and peer review Not commissioned; not externally peer reviewed.