Article Text

Abstract
The pipeline embolization device has demonstrated clinical success in the management of complex intracranial aneurysms arising along the anterior intracranial circulation with a relatively low complication profile. A case report is presented which describes a novel complication of delayed intraparenchymal hemorrhage following deployment of a pipeline embolization device for the treatment of a previously ruptured partially thrombosed ophthalmic segment aneurysm.
- Angiography
- aneurysm
- arteriovenous malformation
- embolic
- artery
- spinal cord
- subarachnoid
- thrombectomy
- catheter
- navigation
- complication
- neck
- balloon
- thrombolysis
- stroke
- stenosis
- malformation
- coil
- brain
- atherosclerosis
- angioplasty
Statistics from Altmetric.com
- Angiography
- aneurysm
- arteriovenous malformation
- embolic
- artery
- spinal cord
- subarachnoid
- thrombectomy
- catheter
- navigation
- complication
- neck
- balloon
- thrombolysis
- stroke
- stenosis
- malformation
- coil
- brain
- atherosclerosis
- angioplasty
Introduction
The pipeline embolization device (PED; ev3, Plymouth, Minnesota, USA) gained FDA approval in April 2011 for the treatment of large (>10 mm) or giant (>25 mm) wide-necked aneurysms occurring between the petrous and superior hypophyseal internal carotid artery segments. Several preliminary series have demonstrated successful endovascular reconstruction of complex aneurysms using this device with acceptable morbidity and mortality rates.1–5 We present a novel complication—subacute intraparenchymal hemorrhage—following PED deployment to treat a residual giant ophthalmic aneurysm.
Clinical case
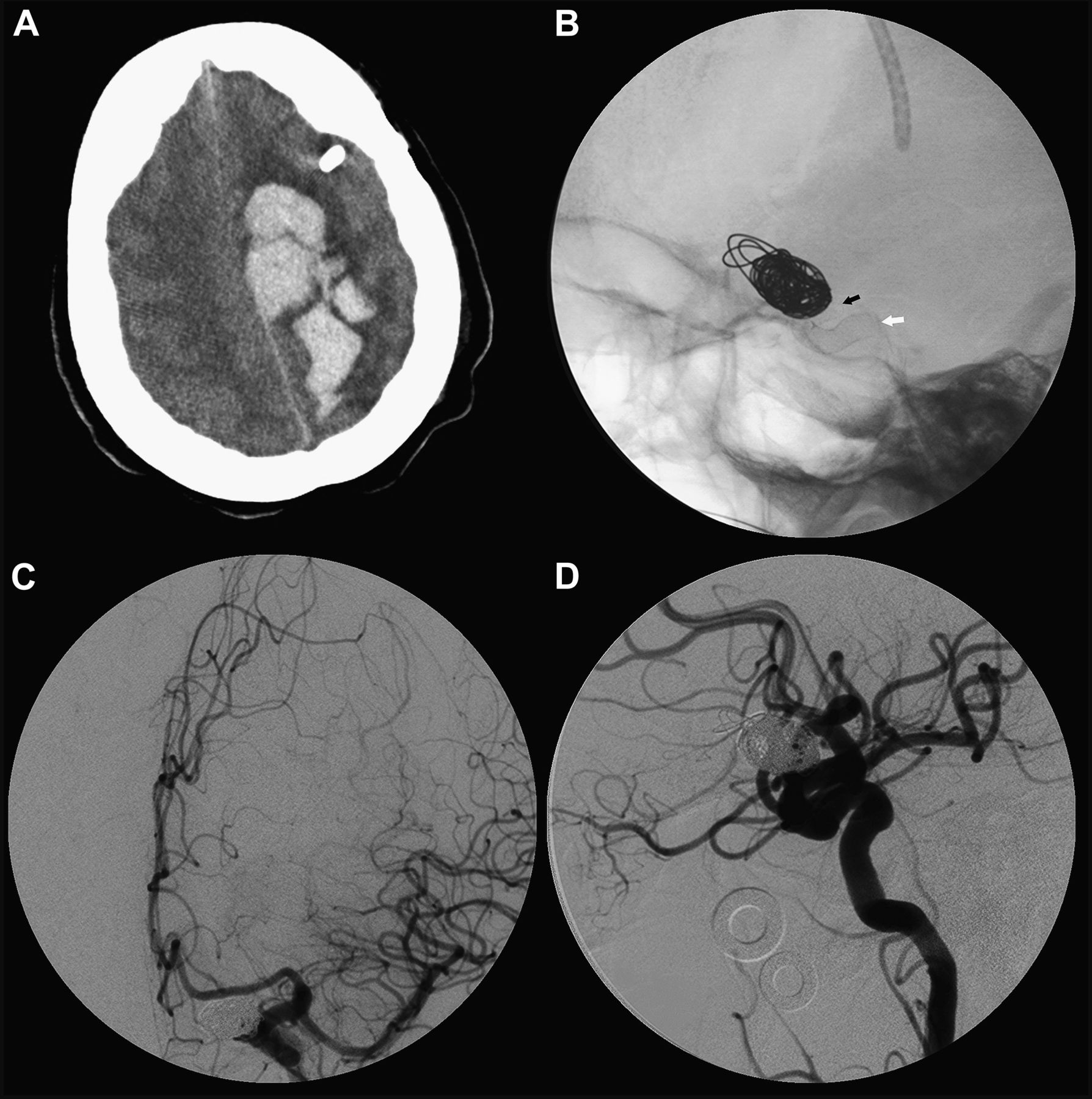
A woman in her late 50s with Hunt and Hess grade 3 subarachnoid hemorrhage presented with a ruptured giant (30 mm) partially thrombosed left ophthalmic aneurysm (figure 1A). On angiography, contrast filled an approximate volume measuring 17×12×8 mm with a large daughter aneurysm sac projecting superolaterally (figure 1B). Transcatheter coil embolization was performed. Two GDC 18 coils (Stryker Neurovascular, Fremont, California, USA) followed by two HydroSoft coils (MicroVention, Tustin, California, USA) were placed. Following placement of the fourth coil, the aneurysm thrombosed almost the entire remainder of its lumen. Despite the low packing density, Raymond grade II embolization was achieved (95% occlusion), as shown in figure 1C and D. She did well initially and was discharged home without neurological deficits.

(A) Post-contrasted axial CT scan of the head showing the giant partially thrombosed left ophthalmic artery aneurysm at the time of initial presentation. (B) Pretreatment anteroposterior angiogram illustrating the wide-necked left ophthalmic artery aneurysm. A daughter sac arising from the superolateral portion of the aneurysm was observed. Post-coiling (C) anteroposterior and (D) lateral digital subtraction angiogram showing residual aneurysm neck filling.
Because of the unusually low packing density and partial thrombosis, the patient returned for early follow-up 4 weeks after initial coiling. Repeat digital subtraction angiography (DSA) demonstrated increased interval recanalization of the residual aneurysm neck (figure 2A and B). Given the high recanalization rate of giant aneurysms and partially thrombosed aneurysms, it was decided to place a PED. The patient was initiated on daily aspirin (325 mg) and clopidogrel (75 mg) 1 week prior to the procedure. A pretreatment clopidogrel assay confirmed therapeutic (33%) platelet inhibition. A single 4.25×16 mm PED was successfully deployed into the left internal carotid artery. Balloon angioplasty using a Hyperform balloon (ev3) was employed to enhance PED apposition to the parent artery wall. Post-placement angiography demonstrated satisfactory positioning of the device (figure 2C and D). Mild internal carotid artery vasospasm developed during PED deployment just distal to the guide catheter (figure 2D). This quickly resolved following repositioning of the guide catheter and injection of intra-arterial verapamil (extrapolated from DSA runs, vasospasm was present for approximately 5 min, possible range 2–9 min). Final anteroposterior and lateral DSA confirmed good capillary filling without evidence of thromboembolism. The patient was discharged home the following day neurologically intact on dual antiplatelet therapy.

Four-week follow-up (A) anteroposterior and (B) lateral angiograms confirmed residual filling of the aneurysm neck. (C) Unsubtracted lateral x-ray following deployment of the pipeline embolization device (PED) in the left internal carotid artery. The proximal (white arrow) and distal (black arrow) ends of the flow diverter are visualized. (D) Post-PED deployment lateral angiogram showing residual but stagnant contrast filling of the aneurysm neck. Mild vasospasm around the guide catheter was observed without angiographic evidence of delayed arterial filling or thromboembolic events.
Five days later she was found unresponsive at home with right-sided hemiparesis. A CT scan demonstrated an 8×3 cm left-sided mesial frontoparietal intraparenchymal hemorrhage remote from the aneurysm (figure 3A). Following intubation, a left-sided ventricular catheter was placed. Although the opening pressure was within normal limits, mild cerebrospinal fluid diversion resulted in neurological improvement to Glasgow Coma Scale 8T. Repeat angiography demonstrated no evidence of PED migration (figure 3B), dissection, thrombus or stenosis (figure 3C and D). No angiographic evidence of residual aneurysm neck filling was observed. According to the family report, the patient was compliant with her aspirin and clopidogrel. Furthermore, cervical and aortic arteriography and echocardiography failed to demonstrate a potential embolic source.
{kind=link}
{kind=link}
{kind=link}
(A) Non-contrast CT scan of the head following placement of a left frontal ventricular catheter for management of a large left frontoparietal intraparenchymal hemorrhage at the time of representation. (B) Follow-up lateral unsubtracted x-ray showing stable positioning of the pipeline embolization device. Repeat (C) anteroposterior and (D) lateral digital subtraction angiogram confirming filling of all major arterial and capillary territories in time without angiographic evidence of dissection or thromboembolic phenomena. No residual aneurysm neck filling was observed.
Discussion
Flow diversion technology attempts to correct underlying hemodynamic factors important to the progression and eventual rupture of aneurysms. By reducing aneurysmal blood inflow, these devices promote stagnation, thrombosis and neointimal formation. The Pipeline for Uncoilable or Failed Aneurysms Study (PUFS), a prospective multicenter single-arm trial of 111 patients, evaluated the safety and efficacy of PED in wide-necked internal carotid artery aneurysms.5 The primary endpoint, total aneurysm occlusion with <50% parent artery stenosis, was achieved in 74% of patients at 1 year. Five patients (4.5%) suffered periprocedural intracerebral hematomas, the details of which have not yet been fully described by the investigators. More recent data from the PED for the Intracranial Treatment of Aneurysms (PITA) trial reported two periprocedural strokes (one hemorrhagic) among 30 patients.3 Szikora et al observed one death among 18 patients who underwent PED deployment following rupture of a coexisting intracranial aneruysm.4 No significant periprocedural complications were reported by Lylyk et al in the treatment of 63 wide-necked aneurysms.2
Despite these accounts, the risk of major stroke following PED deployment has been quoted to be as low as 2%.6 Hemorrhagic complications secondary to vessel perforation and puncture site hematomas have been described.2–5 To date, no published reports of delayed intraparenchymal hemorrhage exist. However, in personal communications, the authors have been anecdotally informed that other practitioners have observed this particular complication. The underlying mechanism of subacute hemorrhage is unclear. No direct iatrogenic injury was observed during the procedure. One potential explanation posits hemorrhagic transformation of an ischemic anterior cerebral artery stroke. Despite the fact that the patient was given antiplatelet therapy, a thrombus may have developed and propagated distally into the anterior cerebral artery, resulting in an infarction that secondarily hemorrhaged. However, no angiographic evidence of thrombus formation was observed during PED deployment or on repeat DSA following the intracranial hemorrhage. Hemorrhagic conversion of small micro-infarctions in the setting of dual antiplatelet therapy is another hypothesis. However, such hemorrhages are not observed with any significant frequency following carotid angioplasty and stenting, a procedure in which micro-infarctions occur at a high rate. Another possible explanation is that the PED stiffened or subtly altered the parent artery course, possibly varying hemodynamic stress. Such blood flow redirection may have effected a spontaneous intraparenchymal hemorrhage.
As with any new device, initially promising clinical results may be tempered by newly discovered complications following wide dissemination. Although flow diverter technology shows significant promise for the treatment of select complex cerebrovascular pathology, stringent reporting of all complications is imperative to avoid misperceptions. The need for timely and rigorous complication reporting has been brought to the forefront of the medical and lay communities following the recent disclosure of under-reported complications from a commonly employed agent used to supplement spinal fusion.7
Acknowledgments
The authors thank Dave Peace for preparation of the figures.
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was not obtained as our institution does not require IRB approval for a case report involving one patient.
-
Provenance and peer review Not commissioned; internally peer reviewed.
-
Data sharing statement The data have not been disseminated in any form to other institutions or journals.