Article Text

Abstract
Background The Penumbra system uses a coaxial separator and continuous extracorporeal suction to remove a clot from a cerebral artery. Forced-suction thrombectomy (FST) involves aspirating clots through the same reperfusion catheter using only a syringe, decreasing the procedure time and supplies needed.
Objective To evaluate multiple combinations of catheters and syringes to determine the optimal pairing for use in FST.
Methods Tests were performed using both the Penumbra system and syringes to aspirate water through Penumbra 0.041 inch (041), 4Max, 0.054 inch (054) and 5Max reperfusion catheters and a shuttle sheath. Dynamic pressure and flow at the catheter tip were calculated from the fill times for each system. Static pressure and force for each aspiration source were determined with a vacuum gauge.
Results All syringes provided significantly higher dynamic pressure at the catheter tip than the Penumbra system (p<0.001). Increasing syringe volume significantly increased static pressure (p<0.001). Both flow and aspiration force significantly increased with catheter size (p<0.001). Cases are presented to demonstrate the clinical value of the laboratory principles.
Conclusions Maximizing static and dynamic pressure when performing FST is achieved by aspirating with a syringe possessing both the largest volume and the largest inlet diameter available. Maximizing aspiration force and flow rate is achieved by using the largest catheter possible.
- Catheter
- Thrombectomy
- Intervention
- Stroke
- Technique
Statistics from Altmetric.com
Introduction
Forced-suction thrombectomy (FST) is a modification to the Penumbra system and, like the Penumbra system, is used as a mechanical recanalization method for ischemic stroke and as a rescue therapy in embolization procedures.1 ,2 In FST, a syringe is directly connected to the proximal hub of a reperfusion catheter with its distal end either on or near a vessel occlusion.1 The syringe plunger is forcibly pulled to generate a negative pressure with the goal of restoring vessel patency by either sucking the occluding element into the catheter or by maintaining a sufficient vacuum to wedge the occluding element onto the distal catheter tip which can then be manually removed from the vessel.
While several recent studies have shown that both the Penumbra aspiration system and FST are safe and efficacious in the treatment of ischemic stroke, they have also alluded to the fact that FST represents a quicker and more flexible treatment option.1 ,3 ,4 Because of its minimalistic design, FST provides advantages in preparation time and time to revascularization. Additionally, if FST fails, it can be quickly and easily converted to the Penumbra system.1 ,3
The current logic in syringe selection for FST is that larger syringes are preferred over smaller ones because of their elevated ‘suction power’1; however, no mechanical analysis of the aspiration pressures developed with different syringes exists. Furthermore, the listed aspiration pressure of the Penumbra system (>20 inHg) does not fully represent the actual aspiration pressure developed at the catheter tip (see Results section).
This study was designed to analyze current aspiration techniques for the treatment of ischemic stroke with the goal of determining working pressures at the catheter tip in order to optimize syringe and catheter selection in FST. Using our ex vivo model, we analyzed different aspiration sources paired with different reperfusion catheters and a shuttle sheath (SS), determining fluid flow and then calculating maximum dynamic pressure or pressure due to fluid velocity achieved in each scenario. In contrast to dynamic pressure developed in full-flow scenarios, we also analyzed the static pressure or pressure in zero velocity (no-flow) situations developed with each aspiration source. From the static pressure data we determined the actual aspiration force applied to the occlusion. While the factors involved in the successful recanalization of occluded vasculature extend beyond applied aspiration pressure, a more informed approach to suction thrombectomy is achieved by understanding the relationship between aspiration source, catheter size and the subsequent pressure and force developed at the occlusion site.
Our goal in this study was therefore to provide information about the working pressures and forces achieved through various aspiration techniques in an effort to highlight the importance of how these variables may affect treatment outcomes. This study also includes clinical examples that demonstrate the applicability and versatility of the principles in question.
Methods
Water was used as the fluid of choice because of its accessibility and similar fluid properties to blood. With a density of 1000 kg/m3, water nearly matches the density of whole blood.5 Additionally, the specific flow rates in this study are high enough to ignore non-linear hemorheological fluid properties and the vessel diameters are large enough to use the assumption of blood as a continuous fluid, further validating water as the fluid of choice.6
One experimental setup for this study involved aspirating water through commonly used catheters (041, 4Max, 054, 5Max and a SS) via different aspiration sources. The inner diameters of the distal catheter tips were experimentally measured and used as the diameter variable in the fluid velocity calculation. Inner diameter values were as follows: 041/4Max catheters: 1.04 mm, 054/5Max catheters: 1.37 mm, SS: 2.4 mm. As the experimental unknown in this study, the suction element was represented by either the Penumbra aspiration system or common syringes ranging in volume from 1 to 60 ml. Experiments were performed in the following manner.
Dynamic pressure analysis: Penumbra aspiration system
Each catheter was connected to the Penumbra aspiration system (Penumbra, Alameda, California, USA) with the distal catheter placed in a volume of water. The Penumbra system was turned on and allowed to equilibrate to working pressure (26.5 inHg). Once equilibrium aspiration pressure was achieved (approximately 2.5 min), the time to aspirate either 100 ml (041, 4Max and 5Max catheters) or 250 ml (054 catheter and SS) was measured and recorded (n=3).
Dynamic pressure analysis: syringes
Before each test run the catheters were primed by filling the test syringe with water and dispensing it into the catheter so that no air remained in the system. 3, 5, 10, 20, 30 and 60 ml BD syringes (Becton, Dickinson and Company, Franklin Lakes, New Jersey, USA) and 3, 6, 10 and 20 ml Medallion syringes (Merit Medical Systems, South Jordan, Utah, USA) were tested by aspirating maximally (rapidly pulling the plunger to the highest volume marking) through the test catheter, the end of which was placed in a volume of water. The time to aspirate the full syringe volume was measured and recorded (n=10). Some syringes were not used because the fill time could not be accurately recorded; this occurred more frequently when aspirating with smaller syringes and larger catheters (eg, BD 3 ml syringe and SS which had a fill time of <1 s). The main difference between the BD and Medallion syringes is their respective inlet diameters (Medallion syringes have inlet diameters of 2.34 mm, BD syringes have inlet diameters of 1.78 mm).
Flow rate (ml/s) was determined by dividing the flow volume by the aspiration time. The fluid velocity at the distal catheter (m/s) was determined by dividing the flow rate by the distal catheter cross-sectional area. In this study the dynamic pressure at the distal catheter (catheter tip) represents the kinetic energy introduced to the occluding element in a full-flow environment (catheter tip close to but not pressed against the occlusion). The dynamic pressure of the system was determined by simplifying Bernoulli's principle to q=½ × рv2 where q is the dynamic pressure, р is the fluid density and v is the fluid velocity at the catheter tip. Dynamic pressure, velocity and flow results were recorded and graphed in Sigma Plot with 2×SD bars.
Static pressure analysis
The static pressure of each device was measured directly with an Equus 3620 Innova Vacuum Gauge (Equus Products, Irvine, California, USA). Both the Penumbra system and each syringe were individually attached to the pressure gauge and, after maximal aspiration, the peak pressure and the test duration was recorded. The Penumbra system was later modified to allow it to pump down before testing the pressure development characteristics. This was accomplished by placing a closed valve in between the Penumbra pump and the vacuum gauge, only opening it after the system had been turned on for over 2.5 min.
Force analysis between catheters
The force applied to the occlusion at the catheter tip is applicable in static or no-flow scenarios. This was determined by multiplying the maximum static pressure of each aspiration source by the area of the catheter exposed to the occlusion. The units for force were recorded in Newtons (N).
Statistical analysis
All statistical analysis was performed in Sigma Plot based on a one-way analysis of variance, Holm–Sidak pairwise multiple comparison procedure (α=0.05). To emphasize statistical variance, error bars are displayed as 2×SD.
Results
Dynamic pressure
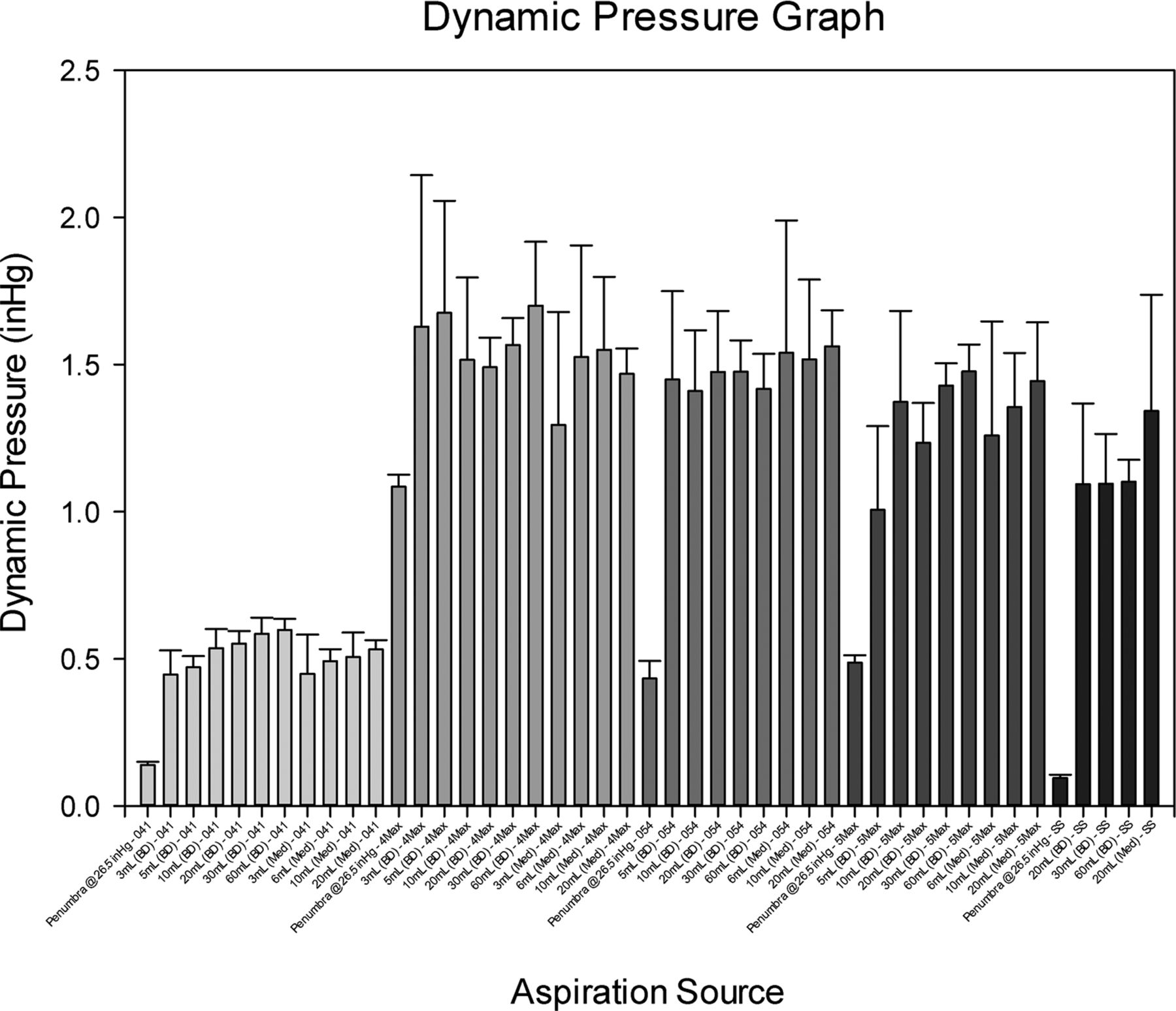
For all test catheters, flow testing revealed that all syringes provided significantly higher mean dynamic pressures at the tip of the catheter compared with the canister (figure 1). The mean dynamic pressures achieved in this study were: 041+syringe (0.52 inHg) versus 041+canister (0.14 inHg) (p<0.001); 4Max+syringe (1.54 inHg) versus 4Max+canister (1.09 inHg) (p<0.001); 054+syringe (1.48 inHg) versus 054+canister (0.43 inHg) (p<0.001); 5Max+syringe (1.32 inHg) versus 5Max+canister (0.49 inHg) (p<0.001); and SS+syringe (1.16 inHg) versus SS+canister (0.10) (p<0.001) (table 1). When using the SS, the 20 ml Medallion syringe provided a significantly higher dynamic pressure (1.3425 inHg) than all of the BD syringes (max 1.1027 inHg) (p<0.001).
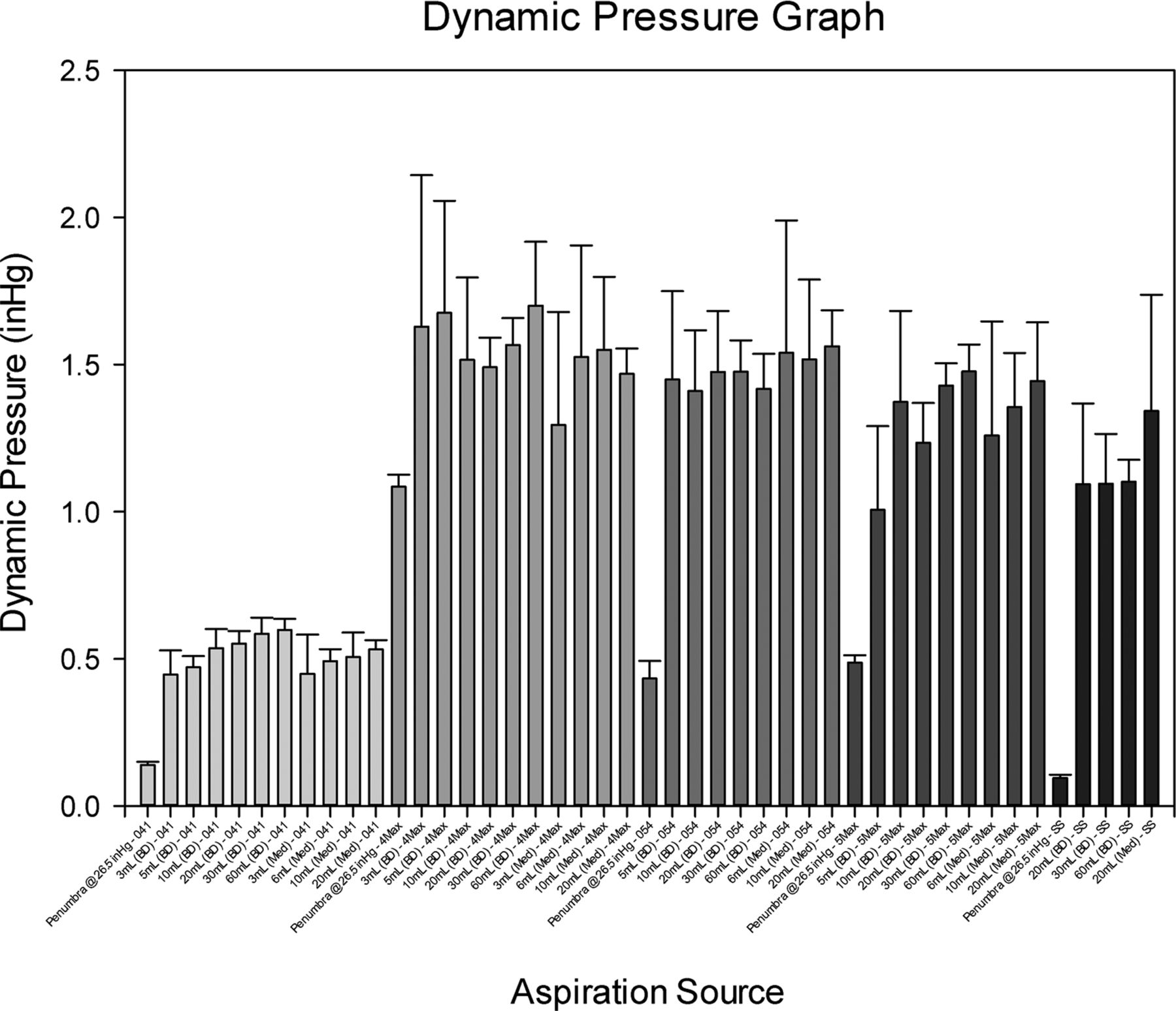
Experimental mean dynamic pressure results. Dynamic pressure, which is directly proportional to fluid velocity at the catheter tip, represents the kinetic energy applied to the occlusion in a full-flow scenario. Generally, dynamic pressure increased as the aspirating syringe volume increased.
Mean dynamic pressure comparison of aspiration sources
Flow rate
Flow rate results confirmed that larger catheters produced higher flow rates given the same aspiration source (figure 2). As an example, aspirating with a 60 ml BD syringe produced average flow rates of 1.71 ml/s (041), 2.89 ml/s (4Max), 4.58 ml/s (054), 4.67 ml/s (5Max) and 12.36 ml/s (SS). With the exception of the 054 catheter compared with the 5Max catheter, different catheter combinations produced significantly different flow rates, including comparing the 041 catheter with the newer 4Max catheter (p<0.001). In general, as the catheter outlet increased in diameter, the flow rate significantly increased (p<0.001).

Experimental flow rate results. Note the 4Max catheter produced significantly higher flows compared to the 041 catheter (p<0.001) and that flow rate increased as catheter outlet diameter increased.
Static pressure
All static pressures are displayed in figure 3. The maximum static pressures of the syringes ranged from 1.5 inHg for 1 ml BD syringes to 23 inHg for 60 ml BD syringes and were achieved almost immediately. The Penumbra system developed a maximum static pressure of 24.5 inHg after 125 s of aspiration. When allowed to pump down for 2.5 min, the Penumbra system developed a maximum static pressure of 24.75 inHg nearly immediately. All maximum static pressures are significantly different from each other (p<0.001).
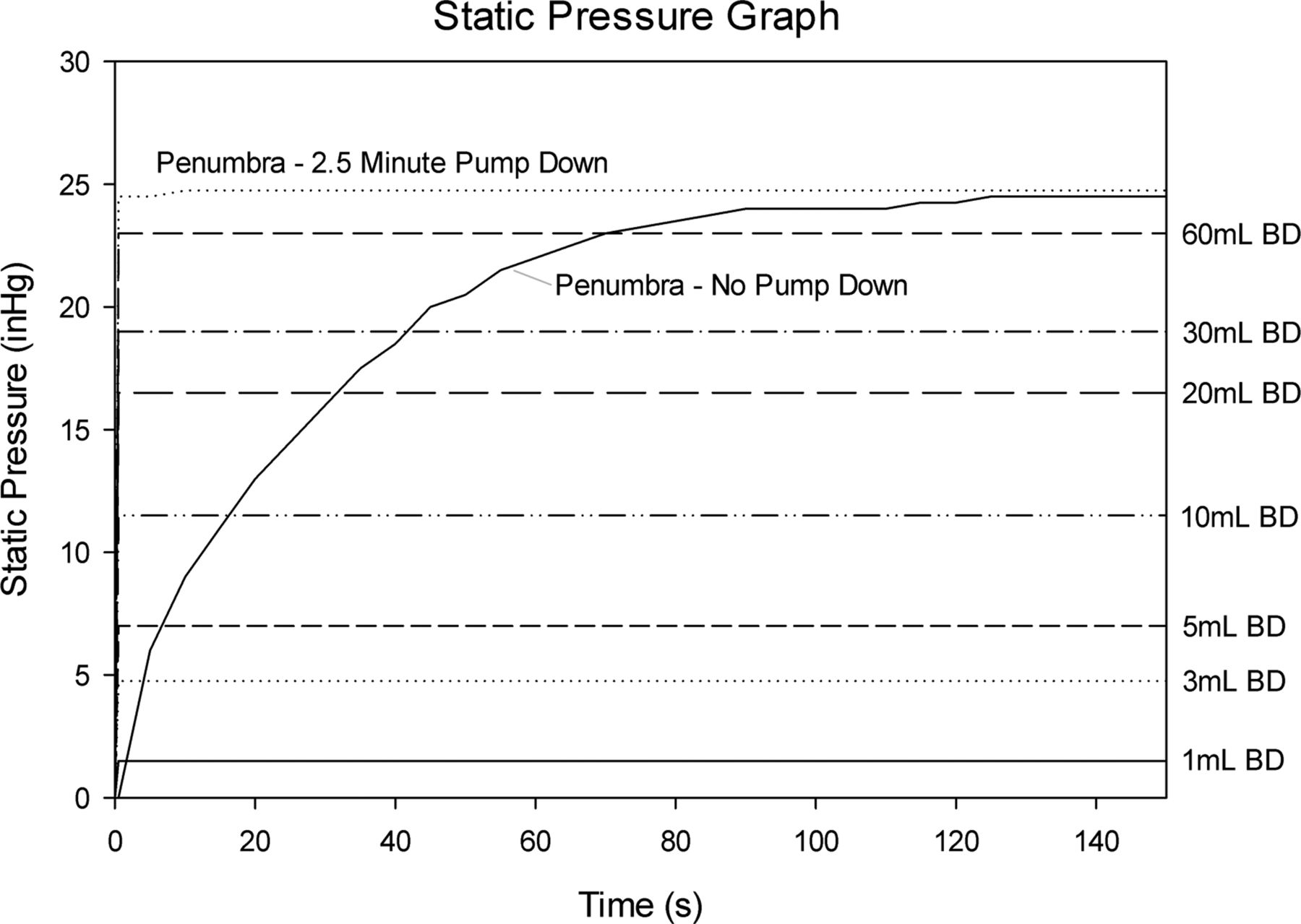
Dynamics of static pressure development for aspiration sources. All maximum static pressures recorded were significantly different (p<0.001). All syringes developed maximum static pressure almost instantly. As used clinically, the Penumbra system required >2 min to develop its maximum static pressure. When given a 2.5 min pump down, the dynamics of static pressure development for the Penumbra system were nearly identical to that of syringes.
Force analysis between catheters
The force analysis between catheters is described using the 60 ml BD syringe as this was the syringe with the highest maximum static pressure, although the comparison is valid for all aspiration sources as it is dependent only on catheter outlet areas. With the 60 ml BD syringe, forces attained in static scenarios are as follows: 60 ml BD+041/4Max catheter (0.066 N), 60 ml BD+054/5Max catheter (0.115 N) and 60 ml BD+SS (0.352 N) (figure 4). All forces in figure 4 are significantly different (p<0.001).

Force comparison between catheters using a 60 ml BD syringe as the aspiration source. Because each aspiration source develops a maximum static pressure independent of catheter size, maximizing the area over which the aspiration pressure is applied maximizes the aspiration force on the occlusion. This is accomplished by aspirating with the largest catheter available.
Case reports
Case 1
A patient presented with acute onset left-sided weakness 3 h after symptom onset. A non-contrast head CT scan revealed a hyperdense middle cerebral artery (MCA) sign on the right and a CT angiogram revealed an abrupt truncation of the right MCA. A CT perfusion suggested a likely infarction in the basal ganglia and likely penumbra, defined as low-flow high-volume prolonged time to drain in the surrounding tissue (figure 5). The patient was taken for cerebral angiography which revealed that the occlusion had progressed to the internal carotid artery (TIMI 0). Taking into consideration the results described above, a SS was placed at the proximal border of the occlusion and FST was performed using a 20 ml Medallion syringe. This opened the artery to the petrous internal carotid artery. Next, a 054 Penumbra reperfusion catheter was placed at the proximal border of the occlusion and FST was performed with the same syringe. This cleared the clot up to the M1, so the 054 was advanced into the M1 and a final suction thrombectomy was performed, completely clearing the clot (TIMI 3). The total time of the procedure from access to closure was 30 min and total time from first aspiration to last was 9 min. The patient awoke from surgery with a hemiparesis. MRI revealed an isolated right basal ganglia stroke. At 9 month follow-up, the patient could ambulate without assistance but experienced persistent left upper extremity weakness.

Case 1. (A) Non-contrast CT scan of the head showing hyperdense middle cerebral artery (MCA). (B) CT angiogram in the axial plane. Black arrow shows filling of the petrous carotid. (C) Digital subtraction angiogram (DSA) of right common carotid artery. White arrow shows no filling of the right internal carotid artery (ICA). (D) DSA of right ICA. White arrow shows that artery has been recanalized to the clinoidal segment. (E) DSA of right ICA. Clot removed up until origin of MCA. White arrow shows tip of 054 reperfusion catheter. (F) DSA of right ICA after all clot removed.
Case 2
Another patient presented with a Hunt–Hess grade 4 Fisher grade 4 subarachnoid hemorrhage from a ruptured anterior communicating artery aneurysm. During coil embolization of the aneurysm via the right internal carotid artery, the right middle MCA became occluded. A Penumbra 054 reperfusion catheter was advanced to the proximal border of the clot. FST was first attempted with a 30 ml BD syringe and then, when this was unsuccessful, a 60 ml BD syringe was used which was also unsuccessful. The 054 catheter was then attached to the Penumbra system (with a separator wire) and the clot was successfully removed (figure 6). Follow-up imaging revealed a small stroke in the MCA territory. At the 6 month follow-up the patient was able to ambulate and to look after his own affairs with minimal help.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 2. (A) Digital subtraction angiogram (DSA) of right internal carotid artery (ICA) showing partially coiled anterior communicating artery aneurysm and mild vasospasm. (B) Abrupt filling defect of the right middle cerebral artery (MCA) consistent with intraprocedural clot. (C) Unsubracted angiogram immediately after forced-suction thrombectomy. White arrow shows opened anterior temporal branch; black arrow shows tip of 054 reperfusion catheter. (D) Post-thrombectomy performed with 054 and 041 reperfusion catheters as well as separators and suction canister demonstrates recanalized vessel.
Discussion
Dynamic conditions (full-flow)
The differences in dynamic pressure between the test groups can be explained by analyzing the limitation to flow in each system. The 041 catheter has a distal cross-sectional area that is 34.2% as large as the inlet cross-section of BD syringes and 19.8% as large as the inlet cross-section of Medallion syringes. In the 041 system the limitation to flow is the relatively small cross-sectional area of the catheter tip compared with the syringe inlet (ie, fluid velocity saturation: maximum fluid velocity is observed at the catheter tip).
In contrast to the 041 catheter, the SS has a distal cross-sectional area that is 181.8% as large as the inlet cross-section of BD syringes and 105.2% as large as the inlet cross-section of Medallion syringes. Because the distal catheter cross-sectional area is larger than the syringe inlet (especially compared with BD syringes), it is no longer the location of flow velocity saturation and therefore not a major limitation to flow. The major limitation to flow when using the SS is the syringe inlet cross-sectional area and is obvious when comparing BD syringes to Medallion syringes when aspirating with the SS. Aspirating through the SS with a Medallion syringe yields a higher dynamic pressure because the flow-limiting factor is now the syringe inlet diameter, which is larger in Medallion syringes than in BD syringes (2.34 mm vs 1.78 mm).
The 054 syringe lies somewhere in between the 041 and the SS in terms of limitations to flow. In the 054 syringe the distal catheter cross-sectional area is 59.4% as large as the inlet cross-section of BD syringes and 34.4% as large as the inlet cross-section of Medallion syringes. While this syringe/catheter combination produces the highest dynamic pressures recorded in this study, there is still a noticeable (if not statistical) difference between the BD and Medallion syringes, suggesting that the syringe inlet is becoming more of a factor in flow limitation.
The newer 4Max and 5Max catheters represent a completely different catheter design. They possess identical outlet diameters to the 041 and 054 catheters, respectively, but that diameter is only maintained at the tips of the catheter (the last 10 cm for 4Max and 20 cm for 5Max) and the remainder of both catheters increases in diameter to 0.064 inch. This increase in bulk catheter diameter reduces the fluid resistance of the catheter as a whole and allows for greater flow through the catheter, thus increasing both the velocity and dynamic pressure at the catheter tip. While both the 4Max and 5Max catheters provided higher flow rates and dynamic pressures than the 041 (for the 4Max) and 054 (for the 5Max) catheters, only the difference between the 4Max and 041 catheters was found to be significant. This is noticeable when viewing the relative increases in flow rate (figure 2) and dynamic pressure (figure 1), which are much more prominent in the 4Max catheter. These advantages are seen only in full-flow scenarios.
It is noted that, generally, the dynamic pressure increases slightly as the syringe volume increases; however, this is not likely to be a true increase in the maximum achievable dynamic pressure in the system. Realistically, in each test the pressure ramps upward and plateaus when the flow limitations of the system are reached and, towards the end of the test, as the syringe body fills with water, the pressure ramps down. Because the aspiration pressure is applied both maximally and instantly in all experiments, the ramps up to the plateau and down from the plateau should be similar for the different syringes, but the relative ramp time compared with the plateau time diminishes as the syringe volume increases (ie, larger syringes spend a larger percentage of aspiration time at the plateau compared with smaller syringes). The diminishing relative ramp time as syringe volume increases manifests itself as increased mean dynamic pressure despite the maximal pressure (the plateau) likely remaining at the same level. With this in mind, the main advantage of larger syringes is their ability to apply maximum dynamic pressure for longer periods of time in full-flow scenarios, simply because their volume is not diminished as quickly as smaller syringes.2
In the interest of removing occlusions from the vasculature, the logical assumption is to choose an aspiration source and catheter combination that provides both maximum dynamic and static pressure so as to introduce as much aspiration force as possible to the occluding element to facilitate its removal. The ideal syringe is not obvious until the physiological parameters of the vasculature of interest are determined. In the case of extremely small vasculature where only an 041 catheter can be used, any syringe will offer similar dynamic pressure. In situations where the 054 catheter is feasible, Medallion syringes seem to offer a slight dynamic pressure advantage over BD syringes (although no statistical difference was determined). In the case where a SS is used, Medallion syringes offer a significant advantage in dynamic pressure compared with BD syringes and their use would introduce the largest aspiration force to the occluding element.
Our data suggest that, in full-flow conditions, maximizing dynamic pressure and the length of time the maximum dynamic pressure is applied is best achieved by aspirating with a syringe with both the largest volume and the largest inlet diameter available. Maximizing the flow rate is achieved by aspirating with the largest catheter possible and preferentially using the newer 4Max and 5Max in lieu of the 041 and 054 catheters, respectively.
Static conditions (no-flow)
Static pressure data are applicable only in no-flow situations and represent the force applied in the worst case scenario during an aspiration thrombectomy procedure (eg, the catheter is engaged directly with the occlusion and no flow occurs after maximal aspiration). Devices capable of producing higher static pressure have the ability to exert more force on an occlusive element. In context, this means that a 60 ml BD syringe, capable of producing 23 inHg static pressure, might be more successful in removing occlusions than a 10 ml BD syringe which produces only 11.5 inHg static pressure. The data confirmed that larger syringes are capable of producing higher static pressures than smaller syringes (back to the original argument; larger syringes have more ‘suction power’); however, no syringe tested matched the static pressure produced with the Penumbra system. Additionally, larger catheters will apply more force to the occlusion simply through an increase in the area in which pressure is applied, so using the largest catheter possible increases the aspiration force applied to the occlusion which should facilitate its removal (figure 4).
It is also important to consider the dynamics of how that pressure develops (figure 3). The syringes, while they achieve lower static pressures, reach their maximum values almost immediately (<0.5 s) whereas the Penumbra system as used clinically (ie, no pump down) took 125 s to reach its maximum static pressure. The dynamics of loading in these two situations are completely different, with the syringes approximating a step-jump in force and the Penumbra system producing a plateauing exponential ramp in force. Modifying the Penumbra system with the addition of a valve so that it could pump down produced a pressure curve with nearly instantaneous loading characteristics, virtually identical to syringes. With regard to no-flow scenarios, using the largest syringe available will provide the highest static pressure and using the largest catheter possible will provide the largest aspiration force onto the occlusion.
Case studies
The experiments and analyses above describe the mechanical characteristics of the aspiration techniques and how to maximize the effectiveness of FST. The cases presented demonstrate the benefits of employing FST as the initial treatment method for ischemic stroke. Case 1 shows that, when successful, FST quickly recanalizes occluded vasculature. Case 2 illustrates a scenario where FST is unsuccessful and demonstrates that transitioning to alternative treatment methods can be done quickly and easily. In this case, the 054 reperfusion catheter was perfectly placed to begin a traditional Penumbra system thrombectomy with a separator wire and the suction canister. It is also possible to perform stent retrieval through the 054 reperfusion catheter using the suction canister in place of a balloon guide catheter for flow arrest. FST can be performed unsuccessfully but not delay the transition to another therapy for any longer than it takes to aspirate with a large syringe and perform a follow-up run.7 In this way, FST does not compete with the latest generation of stent retrievers, but complements them.
It might be reasonably asked if Case 2 demonstrates that the traditional Penumbra set-up is the superior system because it removed the clot and FST did not. On the contrary, we believe that the rationale for using FST is that the length of the procedure is only as long as access and the time needed to aspirate on a syringe, which is especially attractive given the fact that time is a key component in the treatment of acute stroke. Case 2 shows that, if FST is unsuccessful, transition to a slower method does not require removal and replacement of guiding or microcatheters and requires only the amount of time necessary to thread a separator wire or stent retriever through the FST catheter already immediately adjacent to the lesion.8
The issue of patient safety is not addressed by the experiments and analysis presented here. While the published series as well as our own experience have yet to yield a complication from aspiration, this by no means is proof that it is impossible. One could imagine that a powerful enough aspiration against a vessel wall could cause endothelial damage. That being said, the literature would seem to support the idea that the pressures generated by the range of syringes available today are safe. Furthermore, the surgeon must be vigilant to ensure that the catheter is engaged with the thrombus. If a thrombus is at a vessel bifurcation such as the M1–M2 junction and it is difficult to determine whether the catheter has engaged the thrombus or the endothelium, it would be prudent to choose another thrombectomy method.
Conclusion
This biomechanical examination suggests that, when aspirating through the 041, 4Max, 054 or 5Max reperfusion catheters, FST is best performed with the largest available BD or Medallion syringe and, when aspirating through a SS, it is best performed with the largest available Medallion syringe. In general, maximizing the static pressure, dynamic pressure and flow developed in FST is achieved by aspirating with a syringe possessing both the largest volume and the largest inlet diameter available. Maximizing the force applied to the occlusion is achieved by aspirating through the largest catheter possible.
Footnotes
-
Contributors Both SDS and CPG contributed equally to all aspects of this study. As the topic expert, SDS is and should be represented as the first author of this study.
-
Funding This research was funded by an unrestricted educational grant by Covidien (Mansfield, Massachusetts, USA) to the Virginia Commonwealth University Department of Neurosurgery.
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Virginia Commonwealth University Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All data discussed in this study are presented; no unpublished data were used.