Article Text

Abstract
Many endovascular techniques have been described in recent years for the management of wide necked aneurysms. The Y stent assisted technique has been generally used for coil embolization of wide necked bifurcation aneurysms. This technique was first described for the treatment of basilar tip aneurysms in combination with several different devices, demonstrating encouraging results. We report the results of the first two cases of wide necked basilar tip aneurysms treated with Y stent assisted coil embolization using a new low profile visible intraluminal stent (LVIS Jr; MicroVention, Tustin, California, USA) delivered through a 0.017 inch microcatheter. We also reviewed the literature comparing other endovascular techniques (coiling alone, stent assisted coiling, and Y stent assisted coiling) for wide necked aneurysms. The LVIS Jr device offers a new option for the treatment of these challenging lesions, with clear advantages over currently available intracranial stents. Larger series and long term results are needed to confirm the applicability and durability of this technique/technology.
- Aneurysm
- Stent
Statistics from Altmetric.com
Introduction
Approximately 5–10% of all intracranial aneurysms are located in the posterior circulation, and aneurysms at the tip of the basilar artery (basilar artery aneurysms (BTA)) represent the most frequent location.1 Despite current refinements in microsurgical approaches and techniques, the morbidity and mortality associated with the surgical treatment of BTA remains considerably high.2 ,3 Aneurysm coil embolization was described over 20 years ago, but endovascular techniques have clearly evolved most in the past decade regarding treatment of wide necked aneurysms. This includes the evolution of single or dual balloon remodeling, aneurysm neck bridging with single intracranial, Y configuration, and cross court stent assisted embolization.4–7 Despite all of these advances, wide necked BTA represent a subset of lesions that remain challenging to either treatment modality.8
Stent assisted coiling for basilar aneurysms was first described in 1997 by Higashida et al,4 and Y stenting assisted coiling was described in 2004 by Chow et al8 with somewhat encouraging results. The use of stent assisted coiling has been adopted as a promising alternative due to its potential mechanical, hemodynamic, and biological advantages over coil embolization alone. The stent provides mechanical support that prevents coil prolapse. It may also serve as a conduit to divert blood flow while providing a scaffold for endothelial growth and vessel healing.4–12
Since the first description of stent assisted coil embolization,4 many different stents have been developed (Neuroform, Enterprise, Solitaire). However, there are no previous studies comparing the safety and efficacy of different endovascular techniques/devices for the management of BTA.
The major drawback of Y stenting configuration is the increased risk of thromboembolic complications. This can occur due to less than ideal stent to wall apposition and the amount of metal exposed to the vessel lumen.
We report the short term results and technique for Y stent assisted coil embolization of unruptured wide necked BTA, using a low profile visible intraluminal stent (LVIS Jr; MicroVention, Tustin, California, USA). Both cases were performed under compassionate use of the device approved by the Mayo Clinic institutional review board and by the USA Food and Drug Administration. The LVIS Jr is a novel neurovascular self-expanding retrievable stent system which is composed of a single round wire braided nitinol and double helix tantalum strands in addition to radiopaque tantalum proximal and distal markers to assist full length visualization. It is a compliant closed cell system that is retrievable up to 80% deployment and provides 12–21% surface area coverage. In the USA, the LVIS Jr is currently available only in study protocols and it is 0.017 inch microcatheter compatible, allowing it to be delivered through such microcatheters and also via the Scepter C balloon catheter system (MicroVention, Tustin, California, USA).
Cases and technique
Patient No 1
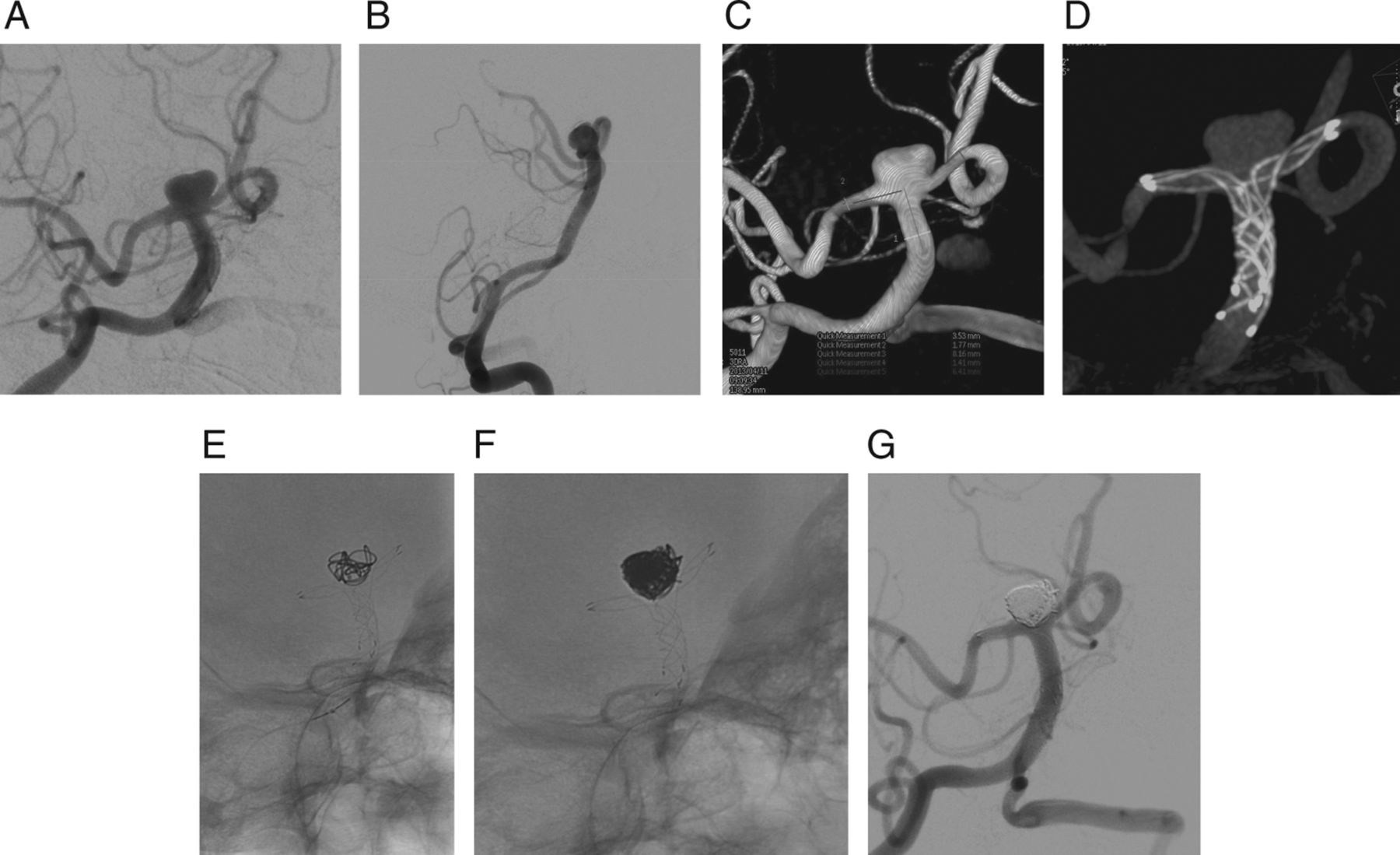
A patient in her late sixties experienced a syncope episode 10 months before being admitted to our institution. At that time, CT scans revealed an aneurysm located in the basilar artery, without indications of a subarachnoid hemorrhage. MRI/MR angiography showed an unruptured BTA. Cerebral angiogram and three-dimensional angiography demonstrated a complex wide necked aneurysm, measuring 9.0 mm×5.0 mm at the dome, with a 8.0 mm broad neck (dome to neck ratio=1.12). The neck of the aneurysm incorporated the origin of the left posterior cerebral artery (PCA) (figure 1A–D). The patient was started on aspirin and clopidogrel prior to the stent assisted coiling procedure. Aspirin and clopidogrel responses were measured with Accumetrics VerifyNow (San Diego, California, USA) and found to be therapeutic.

Patient No 1. Digital subtraction angiogram, anteroposterior (A) and lateral (B) views, show a wide necked distal basilar trunk aneurysm. Three-dimensional reconstruction (C) and digital subtraction angiogram (D), anteroposterior views, demonstrate landing zone measurements in anticipation for Y stent assisted coiling of the aneurysm. Native fluoroscopy, anteroposterior view, shows the first low profile visible intraluminal stent (LVIS Jr) deployed from the left posterior cerebral artery to the basilar trunk (E). Native fluoroscopy, anteroposterior view, shows a second LVIS Jr stent in place with a microcatheter into the aneurysm (F). XPert CT reconstruction (G) shows the final Y configuration stent construct with very good wall apposition. Unsubtracted (H) and digitally subtracted angiogram (I), anteroposterior views, after dense coil embolization showing patent posterior cerebral arteries and near complete occlusion of the aneurysm.
The patient was brought to the neurointerventional suite and placed supine on the angiography table under general anesthesia. A 5 F sheath was placed into the right common femoral artery. Then a 5 F DAV catheter was introduces over a 35 Glidewire and advanced selectively into the left vertebral artery. At this point, 5000 units of intravenous heparin were administered to obtain an activated coagulation time >200 s. A 6 F Neuron 0.70 guide catheter (Penumbra, Alameda, California, USA) was advanced into the distal segment of the left vertebral artery under roadmap guidance. A Headway 17 microcatheter (MicroVention, Tustin, California, USA) was navigated over a 0.014 inch Traxcess guidewire (MicroVention) into the left PCA across the aneurysm neck. The wire was removed and a 2.5×22 mm LVIS Jr stent was deployed, centered across the aneurysm neck, extending from the left PCA into the mid-basilar trunk, covering a portion of the aneurysm neck (figure 1E). After the first stent was deployed, a coil embolization attempt was made, with significant coil prolapse into the right-sided PCA, precluding coil detachment. For this reason, a second Headway microcatheter was navigated across the first stent into the right PCA with a second 2.5×22 mm LVIS Jr stent deployed into the right PCA, creating a Y stent configuration (figure 1F). Xpert CT was obtained, demonstrating good stent positioning with very good wall apposition (figure 1G). Lastly, the aneurysm was coiled, obtaining near complete occlusion on post-procedure angiography (figure 1H–I).
On the initial 30 day follow-up visit, the patient described an episode of vision blurriness and dizziness which resolved spontaneously. At the 3 month follow-up, there was no significant change on clinical examination. The patient was neurologically intact and we continued her on a dual antiplatelet regimen. Follow-up imaging will be obtained at 6 months.
Patient No 2
A patient in her late sixties was referred to our institution after a BTA was incidentally found on an MRI during a workup for multiple sclerosis. MR angiography and angiography demonstrated a bilobed lesion incorporating both posterior cerebral arteries. Given the morphological characteristics of the aneurysm, the decision was made to proceed with stent assisted coiling. The patient was treated with clopidogrel and aspirin for 7 days before the procedure, with therapeutic levels obtained.
Under general anesthesia, a 7 F introducer sheath was placed into the right femoral artery and a Neuron 6 F 0.070 was placed into the left vertebral artery. Heparin 50 U/kg were given, and a therapeutic activated clotting time was obtained. Periprocedure angiography showed a BTA measuring approximately 8.3 mm×4.5 mm, with a 7.2 mm neck (dome to neck ratio=1.15) (figure 2A–C). A Headway 17 microcatheter was advanced over a 0.014 inch Traxcess guidewire to the left PCA. The wire was then removed and a 2.5×24 mm LVIS Jr stent was advanced and successfully deployed, covering the left portion of the aneurysm, and centered across the aneurysm neck with the distal markers in the left P1 and the proximal markers in the basilar trunk. Using the same Headway microcatheter, a second 2.5×16 mm LVIS Jr stent was placed across the right portion of the aneurysm into the right P1, creating a Y shaped configuration that protected both posterior cerebral arteries (figure 2D). Then, the microcatheter was manipulated cautiously into the aneurysm and the aneurysm was subsequently coiled (figure 2E). Post-embolization angiography showed near complete occlusion of the aneurysm (figure 2F–G). The patient was extubated with no periprocedural complications and was neurologically intact with no symptoms at the 30 day follow-up.

{kind=link}
{kind=link}
Patient No 2. Digital subtraction angiogram, anteroposterior (A) and lateral (B) views, demonstrates a bilobed wide necked distal basilar trunk aneurysm. Three-dimensional reconstruction (C) shows landing zone measurements in preparation for stents, and after the low profile visible intraluminal stents have been placed across the aneurysm neck in a Y configuration (D). Native fluoroscopy, anteroposterior view (E), shows initial coil placement against Y configuration stent. Cerebral angiogram, anteroposterior views, native (F) and subtracted (G) final runs depicting patent posterior cerebral arteries and near complete occlusion of the aneurysm.
Discussion
BTA account for approximately 5% of all intracranial aneurysms and 50% of aneurysms located in the posterior circulation. These lesions are associated with a higher probability of rupture compared with anterior circulation aneurysms.13 ,14 In addition, the prognosis after rupture of posterior circulation aneurysms is extremely poor, thereby favoring more aggressive neurosurgical intervention over observation.13 Despite the fact that catheterization of BTA is technically easy because of the straight angle of the basilar trunk, prolapse of the coils with possible thromboembolism into the perforator rich basilar apex and posterior cerebral arteries is a considerable challenge. The direction of flow also makes this anatomical location more prone to recurrence. There are various methods for parent artery reconstruction of wide necked aneurysms prior to coil embolization, such as balloon remodeling, P1 to P1 horizontal stent assisted, parallel stenting, and Y stent assisted coiling.15–19
With recent advances in stent technology, stent assisted coiling has become common practice in the treatment of wide necked BTA. Self-expanding stents, such as the Neuroform, Enterprise, Solitaire, LVIS, and LVIS Jr, have been designed specifically for intracranial deployment. Although more straightforward and safer in the case of a wide necked BTA, placement of a single stent at the top of the basilar artery may not protect the contralateral PCA from coil herniation. In these cases, utilization of a balloon or a second stent is required to protect the contralateral PCA and reconstruct the basilar apex, allowing for better packing and possible lower aneurysm recurrence rates.
In theory, placement of a stent across the neck of the aneurysm alters the blood flow pattern and disrupts the flow in the aneurysm, thus allowing for a spontaneous thrombosis of the aneurysm. Shobayashi et al20 demonstrated the intra-aneurysmal hemodynamic alterations between single stent and flow diverters in a three-dimensional realistic computational aneurysm model without coil placement. In the report, a single stent induced a reduction in mean flow velocity of 14%. However, there was only a small change in the overall intra-aneurysmal flow pattern with a reduction in the mean intra-aneurysmal pressure of 4 mm Hg. These changes in blood flow lead to progressive aneurysm thrombosis. The presence of a stent also facilitates aneurysm neck endothelization, improving durability compared with other endovascular techniques.
Despite the lack of prospective studies comparing the procedural and long term results of Y stenting techniques, the overall data to date have been improving. In the Thomas Jefferson endovascular team10 review of 235 cases of BTA, there were 16 cases treated with Y stent assisted coiling. The authors reported no significant differences in the rates of complications, recurrence, or retreatment between conventional and Y stenting techniques. However, the Y stenting group showed a trend toward lower rates of recanalization (8.3%) and retreatment (0%) compared with the single stenting group. Accordingly, Spiotta et al21 reported their experience in 19 wide necked aneurysms (18 basilar apex) using Neuroform stents in a Y configuration.21 Complete aneurysm occlusion at the last follow-up (mean of 16 months) occurred in 63% of the aneurysms. The authors argued that initial complete obliteration of the aneurysm was the highest predictor of long term occlusion. Zhao et al22 reported a complete occlusion rate at 9 months of 91% in 11 patients treated with the Enterprise and Neuroform stents in a Y configuration. These results demonstrate that Y stenting techniques may provide a durable option for lesions previously not ideal or amenable to endovascular treatment. Moreover, considering the complexity of the lesions and that Y stenting was conducted as a salvage procedure for failed conventional coiling, the overall morbidity rates in these studies compare favorably with other endovascular techniques. Procedural thromboembolic events have ranged from 0% to 16% in large case series.9 ,21 ,22 These events involve small transient cerebellar infarcts or asymptomatic punctuate lesions on MRI.21 Spiotta et al encountered two delayed occipital infarcts 2 months after the procedures, both of which recovered completely. Contrary to these studies, Hwang et al23 have suggested that stent assisted coil embolization of unruptured aneurysms, which are unfavorable for simple coiling, does not significantly improve the long term angiographic outcome at 2 years. Our experience shows improved overall results of endovascular aneurysm treatment when using intracranial stents. (Hanel RA, personal communication)
The capacity of the cell expanding structure in the stent is frequently associated with difficulties during the passage of a second stent.15 ,19 ,24–29 In the current study, the new low profile visualized intraluminal stent proved advantageous because it is a self-expanding braided stent device. In addition, it is well visualized throughout its course due to three radio-opaque helical strands. The three distal device markers are evenly spaced around the circumference of the device while the three proximal markers are paired together. The smaller cell structure (w 0.9 mm) provides greater protection across the aneurysm neck and improves flow diversion compared with other currently available stents. The braided wire structure enables the strands of wires to slide on each other, allowing catheterization through the interstices. The device is the first stent for aneurysm to be delivered through a 0.017 inch microcatheter, making it considerably easier to navigate, especially when difficult anatomy is found. There is a short lead coil attached to the delivery wire system. The device is initially unsheathed and then is pushed out. It may be reconstrained up to 80% of its deployment. Once deployed, the delivery wire is removed and the microcatheter can access the true lumen of the device using a traditional microwire. The proximal and distal markers splay apart, demonstrating that the proximal and distal ends of the device are open. The three helical strands also spread into a double helix configuration, with alternating wall opposition visible on angiograms.
In cases of Y stenting configuration, the fact that the LVIS Jr stent is delivered through a 0.017 inch microcatheter makes crossing the first stent easier, due to the low profile of microcatheter. Also, the braided nature of the device allows for better wall apposition, with a theoretically lower risk for thromboembolic complications.
Conclusion
The technique of stent assisted coiling of aneurysms has been adopted as a promising adjunct with potential advantageous mechanical, hemodynamic, and biological properties; theoretically imparting an advantage over coil embolization alone, with lower rates of recanalization and retreatment.
The LVIS Jr stent provides a safe and technically straightforward option for Y stent assisted coiling of wide necked BTA. The steps to achieve satisfactory deployment are improved compared with other available devices due to the device's profile, its cell structure, and excellent visualization throughout the procedure.
Acknowledgments
The authors would like to thank Alison Dowdell and Victoria Jackson for the careful review of this manuscript.
References
Footnotes
-
Contributors MDC and ANR made significant contributions to the conception, design/analysis, and interpretation of the data. MDC and LBCB made significant contributions to drafting/revising the article. RAH made significant contributions to all aspects of this work.
-
Funding The Mayo Clinic has received an unrestricted educational grant (grant No 92693) from MicroVention.
-
Competing interests All authors declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics approval Both cases were performed under compassionate use of the device approved by the Mayo Clinic institutional review board and by the USA Food and Drug Administration.
-
Provenance and peer review Not commissioned; externally peer reviewed.