Article Text

Abstract
Background Patients with M2 middle cerebral artery (MCA) occlusions are not always considered for endovascular treatment.
Objective To study outcomes in patients with M2 occlusion treated with endovascular procedures in the era of stentrievers.
Methods We studied patients prospectively included in the SONIIA registry (years 2011–2012)—a mandatory, externally audited registry that monitors the quality of reperfusion therapies in Catalonia in routine practice. Good recanalization was defined as postprocedure Thrombolysis in Cerebral Infarction (TICI) score 2b–3; dramatic recovery as drop in National Institutes of Health Stroke Scale (NIHSS) score >10 points or NIHSS score <2 at 24–36 h; and good outcome as modified Rankin score (mRS) 0–2 at 3 months. A 24 h CT scan determined symptomatic intracranial hemorrhage (SICH) and infarct volume.
Results Of 571 patients who received endovascular treatment, 65 (11.4%) presented an M2 occlusion on initial angiogram, preprocedure NIHSS 16 (IQR 6). Mean time from symptom onset to groin puncture was 289±195 min. According to interventionalist preferences 86.2% (n=56) were treated with stentrievers (n=7 in combination with intra-arterial tissue plasminogen activator (tPA), 4.6% (n=3) received intra-arterial tPA only, and 9.2% (n=6) diagnostic angiography only. Good recanalization (78.5%) was associated with dramatic improvement (48% vs 14.8%; p=0.02), smaller infarct volumes (8 vs 82 cc; p=0.01) and better outcome (mRS 0–2: 66.3% vs 30%; p=0.03). SICH (9%) was not associated with treatment modality or device used. After adjusting for age and preprocedure NIHSS, good recanalization emerged as an independent predictor of dramatic improvement (OR=5.9 (95% CI 1.2 to 29.2), p=0.03). Independent predictors of good outcome at 3 months were age ( OR=1.067 (95% CI 1.005 to 1132), p=0.03) and baseline NIHSS ( OR=1.162 (95% CI 1.041 to 1.297), p<0.01).
Conclusions Endovascular treatment of M2 MCA occlusion with stentrievers seems safe. Induced recanalization may double the chances of achieving a favorable outcome, especially for patients with moderate or severe deficit.
- Stroke
- Thrombectomy
- Angiography
Statistics from Altmetric.com
Background
Despite their ability to achieve high rates of recanalization in acute ischemic stroke, endovascular procedures with last-generation devices such as stentrievers are under investigation in multiple randomized trials to demonstrate their benefits.1–3 The still uncertain benefits of endovascular procedures in proximal intracranial vessel occlusions are even more controversial when considering distal occlusions such as the M2 middle cerebral artery (MCA) segment. In M2 occlusions clinical outcome might be independent of recanalization given the limited amount of tissue at risk; however, strategic small infarct may also cause significant clinical and functional impairment.4
The limited number of studies focusing on patients with M2 MCA occlusion show contradictory results. On the one hand, an Interventional Management of Stroke II (IMS II) study subanalysis of patients with an M2 occlusion on initial angiogram showed a low rate of recanalization (Thrombolysis in Myocardial Infarction (TIMI) score 2–3: 43%) but high rate of good clinical outcome (90 days modified Rankin score (mRS) 0–2: 65%).4 On the other hand, data from the Multi- Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trials in a similar population showed a high rate of recanalization (TIMI 2–3: 81%) but a low rate of favorable outcome (mRS 0–2: 40.7%).2 Finally, a subgroup analysis of the PROACT-II study showed the benefits of recanalization that could double the chance of a good clinical outcome at 90 days.5 In all these studies patients were treated with procedures or devices that are surpassed by the results of new-generation stentrievers.6 ,7
We aimed to investigate the possible benefits and safety of endovascular procedures in the era of stentrievers in patients with acute stroke with an M2 MCA occlusion treated under routine clinical conditions and included in a multicentric official registry of patients.
Methods
We studied patients prospectively included in the Sistema ONline d'Informació de l'Ictus Agut (SONIIA) registry from January 2011 to December 2012, a mandatory and externally audited registry that monitors quality of all reperfusion therapies performed in Catalonia under routine practice conditions.8 Stentrievers were widely used in routine practice before the registry was set up and all interventionalists had considerable experience in the use of the devices.
Baseline characteristics, including preprocedure National Institutes of Health Stroke Scale (NIHSS) score and occlusion location on initial angiogram, were collected for all patients. Only patients with an initial occlusion in the M2 segment of the MCA were included. The decision to perform endovascular procedures was made according to the stroke neurologist and interventionalist criteria.
We defined good recanalization as Thrombolysis in Cerebral Infarction (TICI) score 2b–3 on the last angiogram, and dramatic recovery as an NIHSS score drop ≥10 points or NIHSS <2 at 24–36 h. Favorable clinical outcome was considered when mRS at 3 months was 0–2. We determined the presence of hemorrhagic transformation9 on the 24–36 h CT scan. This scan was also used to calculate infarct volume10 in all patients treated in one of the centers. The registry also requires prospective recording of all procedural related complications.
Statistical analysis
Descriptive and frequency statistical analyses were obtained using SPSS 17.0 software. Categorical variables are presented as absolute values and percentages, and continuous variables as median±SD if normally distributed or median (interquartile intervals) if not normally distributed. Statistical significance for intergroup differences was assessed by Pearson χ2 or Fisher exact test for categorical variables and by Student t or Mann–Whitney U test for continuous variables.
Multivariable logistic regression analyses were performed for each group to determine factors that could be considered as independent predictors of favorable outcome.
Variables showing p<0.1 in univariate analysis were included in the multivariate model. A probability value of <0.05 was considered significant for all tests.
Results
Of the 571 registered patients who received endovascular treatment in the study period, 65 (11.4%) presented a single M2 occlusion on the initial angiogram. They had the following characteristics: mean age 66±15 years, female 47.7%, median preprocedure NIHSS 16 (IQR 6), and 45 cases (69.2%) were left MCA M2 occlusions. Thirty-five patients (53.8%) received intravenous (IV) tissue plasminogen activator (tPA) before the procedure. Ten patients (15.4%) received general anesthesia before the procedure. Mean time from symptom onset to groin puncture was 289±195 min. Baseline characteristics are shown in table 1.
Baseline characteristics of patients and main outcomes according to early recanalization or not
According to interventionalist preferences, of the 65 patients, 86.2%, (n=56) were treated with stentrievers; of these 10.8% (n=7) in combination with intra-arterial (IA) tPA, 4.6% (n=3) received IA tPA only (n=3), and the rest 9.2% (n=6) received diagnostic angiography only. The following stentrievers were used, Solitaire FR Covidien, Mindframe Capture, Trevo Pro Retrieval System by Concentric Medical, Preset stent retriever. Detailed information on the specific device or devices used in each case was not recorded.
To obtain a better profile of the stentrievers we could have performed the analysis after excluding the few patients in whom a stentriever was not finally used (13.8%). However, to obtain a better report of the expected results in routine clinical practice, we decided to include all patients with an M2 MCA occlusion treated during the studied period. Of the six patients who received diagnostic angiography only (preprocedure NIHSS 11.5 (IQR 6)), four (67%) had a favorable clinical outcome at 3 months.
Patients who achieved good recanalization (TICI score 2b–3: 78.5%, n=46) had more often dramatic improvement (48% vs 14.8%, p=0.02), smaller infarct volumes (8 vs 82 cc, p=0.01) and better outcome (mRS 0–2: 66.3% vs 30%; p=0.03) than those who did not recanalize (table 1). After adjusting for age and baseline NIHSS, good recanalization emerged as an independent predictor of dramatic improvement (OR=5.9 (95% CI 1.2 to 29.2), p=0.03). Previous IV tPA treatment was not associated with higher recanalization rates (28% vs 22% p=0.69).
At 3 months 60% of patients had a good outcome and the death rate was 16.4%. Age, no history of hypertension, preprocedure NIHSS, and good recanalization were associated with good outcome. Independent baseline predictors of good outcome at 3 months were age (OR=1.067 (95% CI 1.005 to 1132), p=0.03) and preprocedure NIHSS (OR=1.162 (95% CI 1.041 to 1.297), p<0.01).
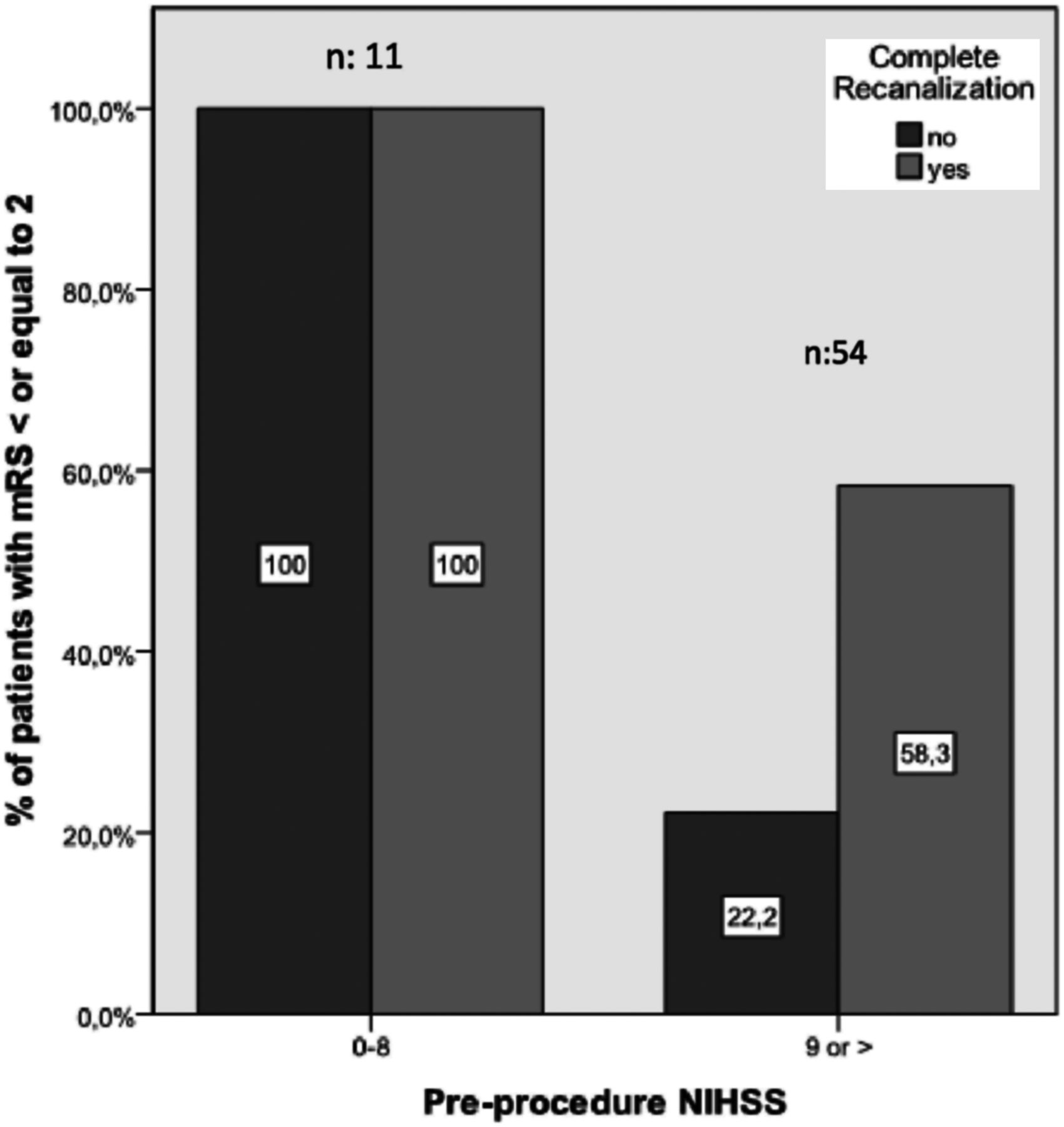
The benefits of recanalization were more obvious in patients with initial NIHSS >8. All patients with initial NIHSS ≤8 had good clinical outcome independently of recanalization status. In patients with NIHSS >8 recanalization increased the chances of good outcome from 22.2% to 58.3% (p=0.05) (figure 1).

{kind=link}
Bars show rate of patients with good clinical outcome (modified Rankin score (mRS) ≤2) at 3 months according to preprocedure National Institutes of Health Stroke Scale (NIHSS).
Symptomatic intracranial hemorrhage (SICH) occurred in six patients (9%), of whom three achieved recanalization and three did not (p=0.53) and two of them had been treated with IV tPA. The use of a stentriever in an M2 branch did not increase the rate of SICH (a stentriever was used in five of the six cases; p=0.169). One patient presented an arterial dissection during the procedure and one patient experienced a local hematoma at the puncture site.
Nine patients died (13.8%) On univariate analysis, preprocedure NIHSS was associated with mortality (NIHSS 19.8 vs 13.3 p<0.01). None of the deaths was related to SICH.
Discussion
Our study describes for the first time outcomes of patients with acute stroke who had an M2 MCA occlusion treated with endovascular procedures in routine practice in the era of stentrievers. The study shows that achieving induced recanalization led to better outcomes without significantly increasing the rate of complications.
In acute stroke management, identification of an occlusion in the M2 segment of the MCA may provide the treating physician with the dilemma of whether or not to start endovascular treatment. Physicians might consider that the limited endangered area does not justify the risks and costs of the procedure. However, on the other hand, a small but strategic cerebral infarct may lead to significant permanent neurological impairment.
The prognosis and best management of acute distal intracranial arterial occlusions, including M2 MCA, is not clear. A recent study describing the natural history of patients with stroke who did not receive any reperfusion treatment showed that up to 44% of patients presenting with a distal MCA occlusion did not achieve a good outcome at 3 months.11 A substudy of the IMS II trial,4 in which patients were treated with IA tPA + endovascular ultrasound with the EKOS catheter, showed that although only 10/23 (43.5%) M2 occlusions achieved grade 3 arterial occlusive lesion recanalization, up to 16/23 (69.6%) achieved mRS 0–2 outcome. A recently published subanalysis of the PROACT trial,5 showed that in patients with documented M2 occlusion, IA treatment with urokinase tripled the rate of recanalization (53% vs 16%) and doubled the chance of a favorable functional outcome (53% vs 28%) as compared with best medical treatment. Another study suggested a greater reduction of infarct volume with IA therapies before stentrievers were widely available as compared with either IV tPA or no reperfusion treatment.12 In that study, the magnitude of infarct volume reduction was maximal in proximal occlusions but still significant for M2 MCA occlusions. The authors found that independently of occlusion site, a baseline NIHSS cut-off point of ≥14 points identified best responders to IA therapies. Our work that specifically studied patients with an M2 occlusion treated with improved devices such as stentrievers showed that patients with a baseline NIHSS>8 benefited most from recanalization.
Our study was intended to help clinicians in the decision-making process of indicating an endovascular procedure in patients with M2 MCA occlusion in a routine clinical practice setting in which devices with improved features6 ,7 such as stentrievers are available. While all patients with an initial NIHSS≤8 achieved a good outcome independently of final recanalization, in patients with NIHSS >8 the outcome was markedly influenced by the achievement of recanalization (mRS 0–2: 58% vs 22%). This fact combined with the high observed rate of recanalizaton and the low rate of complications, as compared with previous studies that showed death rates >20%,2 ,5 advocates the use of stentrievers in confirmed M2 MCA occlusions, especially if causing moderate to severe symptoms.
Our study has several limitations for a descriptive study. First, the small sample; second, although the majority of the devices were stentrievers, there were other treatments, such as IA tPA; and finally, it did not include a control group receiving no intervention that could confirm our findings. However, this is a consecutive, prospective and externally audited series that shows for the first time trends in safety and improved outcome in patients with distal MCA occlusions treated under routine clinical conditions in the era of stentrievers. Most patients were treated in high-volume centers with interventionalists with extensive experience with stentrievers. This should be taken into account when applying the conclusions of our study to other situations.
Conclusion
Endovascular treatment of M2 MCA occlusion with stentrievers seems safe. Induced recanalization may double the chances of achieving a favorable outcome, especially in patients with moderate to severe symptoms.
References
Footnotes
-
Contributors MR and AF participated in the conception and design of the study. MR, AF and SA analyzed and interpreted the data. MR, AT, PC, MG, PGB, VO, XU, JM-F, DC and JR treated and included the patients in the study. MR carried out the statistical analysis and wrote the article. All authors advised, reviewed and approved the manuscript.
-
Competing interests MR is the recipient of a grant from Instituto de Salud Carlos III, Ministerio de Economía y Competitividad (FIS: PS09/01660). AS is the recipient of a Rio Ortega grant from the Instituto de Salud Carlos III, Ministerio de Economía y Competitividad.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.