Article Text

Abstract
Background The degree of aneurysm occlusion following coil embolization has an impact on aneurysm recanalization.
Objective To explain the natural history of intracranial aneurysms with neck remnant, Raymond–Roy Occlusion Classification (RROC) class II.
Methods A single-center, retrospective study of 198 patients with 209 aneurysms treated with coil embolization that were initially either RROC class I or II. The angiographic outcomes at short- and long-term follow-up were compared as well as the complication/re-treatment rates. Atypical aneurysms and those that had been previously treated were excluded.
Results Ninety-nine class I aneurysms were compared with 110 class II aneurysms. There was no difference in recanalization rate between the groups (class I 3.3% vs class II 8.5%, p=0.478) at short-term follow-up (8.2 months) and at subsequent follow-ups (21.7 and 52.1 months). There was also no difference in re-treatment rates (class I 3.3% vs class II 8.5%, p=0.196) or complication rates (class I 9.1% vs class II 4.6%, p=0.12). There were no aneurysm ruptures after treatment in either group.
Conclusions The angiographic outcome of aneurysms with neck remnant following coil embolization is similar to that of completely occluded aneurysms in that most remain stable and few recanalize. This understanding could potentially help the interventional neurosurgeon avoid complications such as coil herniation, vessel compromise, and stroke in selected cases. Further investigation with a larger patient population is warranted.
Statistics from Altmetric.com
Introduction
Coil embolization has been used increasingly over the past two decades for the treatment of intracranial aneurysms. Incomplete occlusion and aneurysm recanalization, however, continue to be disadvantages of this approach.1– –4 The Raymond–Roy Occlusion Classification (RROC) system is the standard for evaluating aneurysm occlusion class following coil embolization.5 In this scheme, class I is defined as complete obliteration, class II as neck remnant, and class III as residual aneurysm. The RROC system was not designed to predict the risk of recurrence or of future rupture.
Prior studies have shown that incompletely occluded aneurysms have a higher risk of recurrence.6 ,7 It has also been shown that the degree of aneurysm occlusion after initial treatment is a predictor of risk of subsequent rupture.8 ,9 There are fewer data, however, that specifically deal with the angiographic behavior of class II aneurysms (neck remnant) as defined by the RROC system following treatment in comparison with class I aneurysms. We hypothesize that class II aneurysms, despite being subtotally occluded, behave similarly to class I aneurysms and have a benign angiographic course.
Methods
Participants and study design
This is a retrospective review of intracranial aneurysms treated with coil embolization at a single institution. Inclusion criteria included both ruptured and unruptured intracranial aneurysms treated with coil embolization that were graded either as RROC class I or II immediately after the procedure. Exclusion criteria included atypical aneurysms (eg, fusiform), previous treatment, and those that were graded RROC class III at the end of the procedure. The aneurysms were divided into two groups according to RROC. The group of class I aneurysms included 96 patients with 99 aneurysms, while the group of class II aneurysms included 102 patients with 110 aneurysms. Aneurysmal and subject characteristics were determined by review of both the subject's medical chart and angiographic data.
Aneurysm and procedural characteristics
Aneurysm size was determined qualitatively and quantitatively. The qualitative system involved using the maximum dome diameter and is as follows: small: <10 mm, large: 10–25 mm, and giant: >25 mm. Posterior communicating artery aneurysms were included in the anterior circulation.
Different degrees of procedural assistance were used, including stand-alone, balloon-assisted, and stent-assisted coiling. Coil types included Galaxy (Codman), GDC (Stryker), Hydrocoil (Microvention), Matrix (Stryker), Orbit (Codman), Penumbra PC400 (Penumbra), Target (Stryker), and Trufill (Codman); stent types included Enterprise (Codman) and Neuroform (Stryker). All aneurysm embolizations were performed by two interventional neurosurgeons and one interventional radiologist. In general, aggressive packing of the aneurysm neck was not performed to assure the patency of the parent vessel and branch vessels.
Outcomes assessment
All initial and follow-up angiograms were reviewed by either interventional neurosurgeon ABP or HM and the RROC was applied. Any contrast seen within the aneurysm at the end of the procedure was defined as class III, even if believed to be a result of heparinization or use of antiplatelet therapy. For the purposes of this study, recanalization was defined as refilling of the aneurysm dome (RROC class III). In other words, class I aneurysms that progressed to class II were not classified as recanalized.
Statistical analysis
Differences in pretreatment variable distribution between classes I and II were assessed using the Mann–Whitney test or χ2 test for continuous and categorical variables, respectively. A Kaplan–Meier analysis and the log-rank test were used to determine differences in time to recanalization and re-treatment. All ranges were reported as IQR, which is a more robust measure of dispersion than simple range. All data management and analyses were conducted using SPSS V.20.0 (IBM, Inc, Armonk, New York, USA).
Results
Patient, aneurysm and treatment characteristics
The baseline patient and aneurysms characteristics were similar between groups and similar to those of most aneurysms series in the literature (tables 1 and 2). The majority of patients were female (71%), the majority of aneurysms were small (87.6%) and in the anterior circulation (92.8%). Ruptured aneurysms comprised 64.1% of the study population. The only difference between groups was the greater number of internal carotid artery bifurcation aneurysms in the class I group. There were no significant differences in treatment between the two groups in coil/stent type, number/volume of coils used, packing density, and procedure time (table 3).
Patient characteristics
Aneurysm characteristics
Procedure characteristics
Angiographic outcomes
In the class I group, 61 (61.6%) patients had a short-term angiographic follow-up at an average of 8. 8 months. Excluding patients who died during their initial admission secondary to complications of subarachnoid hemorrhage, and patients who were not yet within the correct time period for a first follow-up, the short-term follow-up yield was 66.3%. In the class II group, 71 (64.5%) patients were available for short-term angiographic follow-up at an average of 7.7 months. As above, excluding patients who died and were not ready for follow-up, the yield was 71.0%.
The recanalization rate at short-term follow-up was statistically the same in both groups (class I 3.3% vs class II 8.5%; p=0.478). Thirteen class I aneurysms (21.3%) worsened to class II at short-term follow-up, but none of these aneurysms worsened to class III at any point and were not regarded as ‘recanalized’ for the purposes of this comparison study. In addition, 12/71 (16.9%) class II aneurysms progressed to thrombosis (class I) at short-term follow-up (table 4). Multivariate analysis failed to demonstrate any patient, aneurysm, or procedural factors that were associated with a higher risk of recanalization in the overall population. Large aneurysm categorical size, however, was associated with recanalization among class I aneurysms (p=0.005) but not among class II aneurysms (p=0.090).
Initial and follow-up RROC
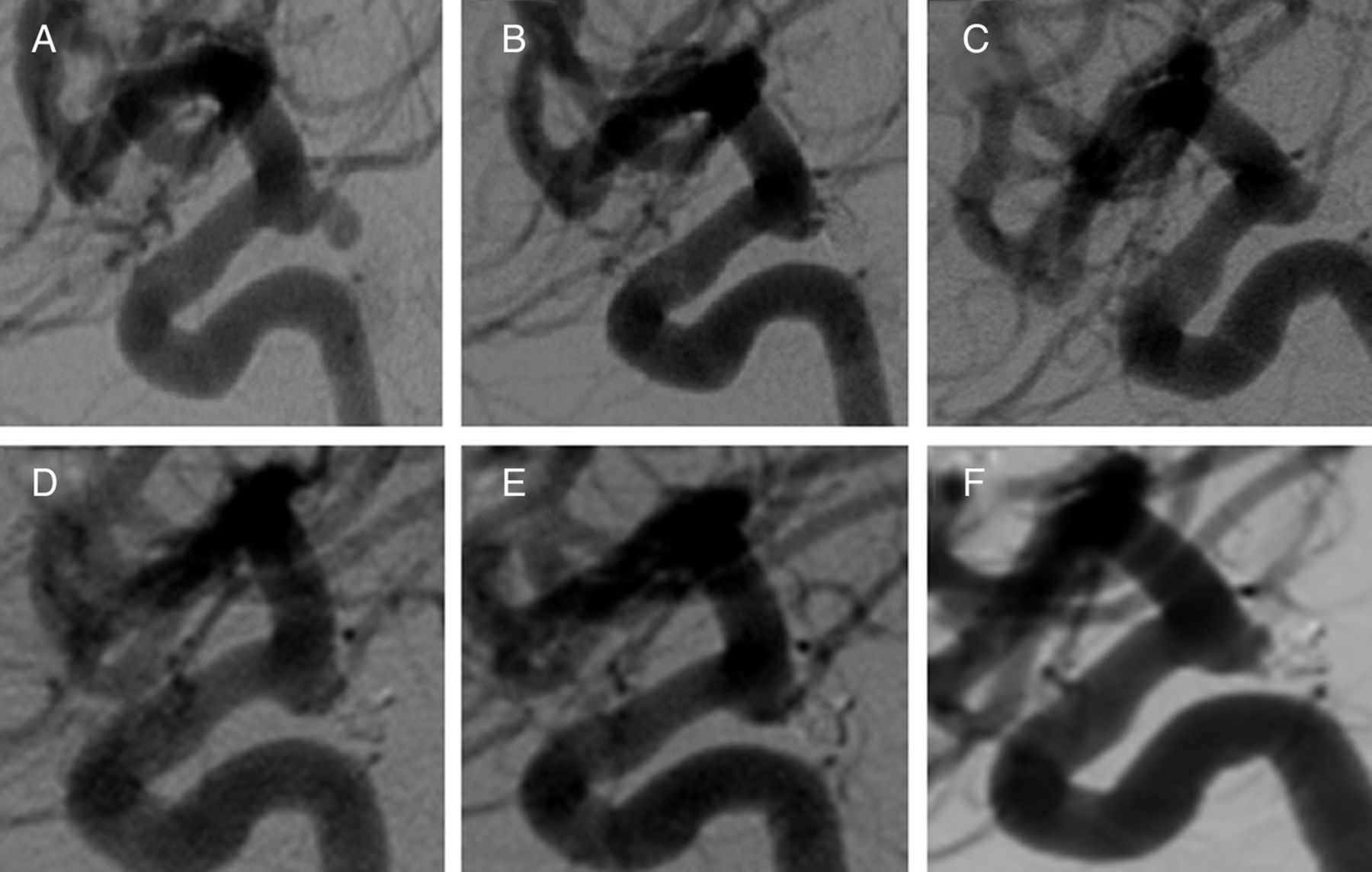
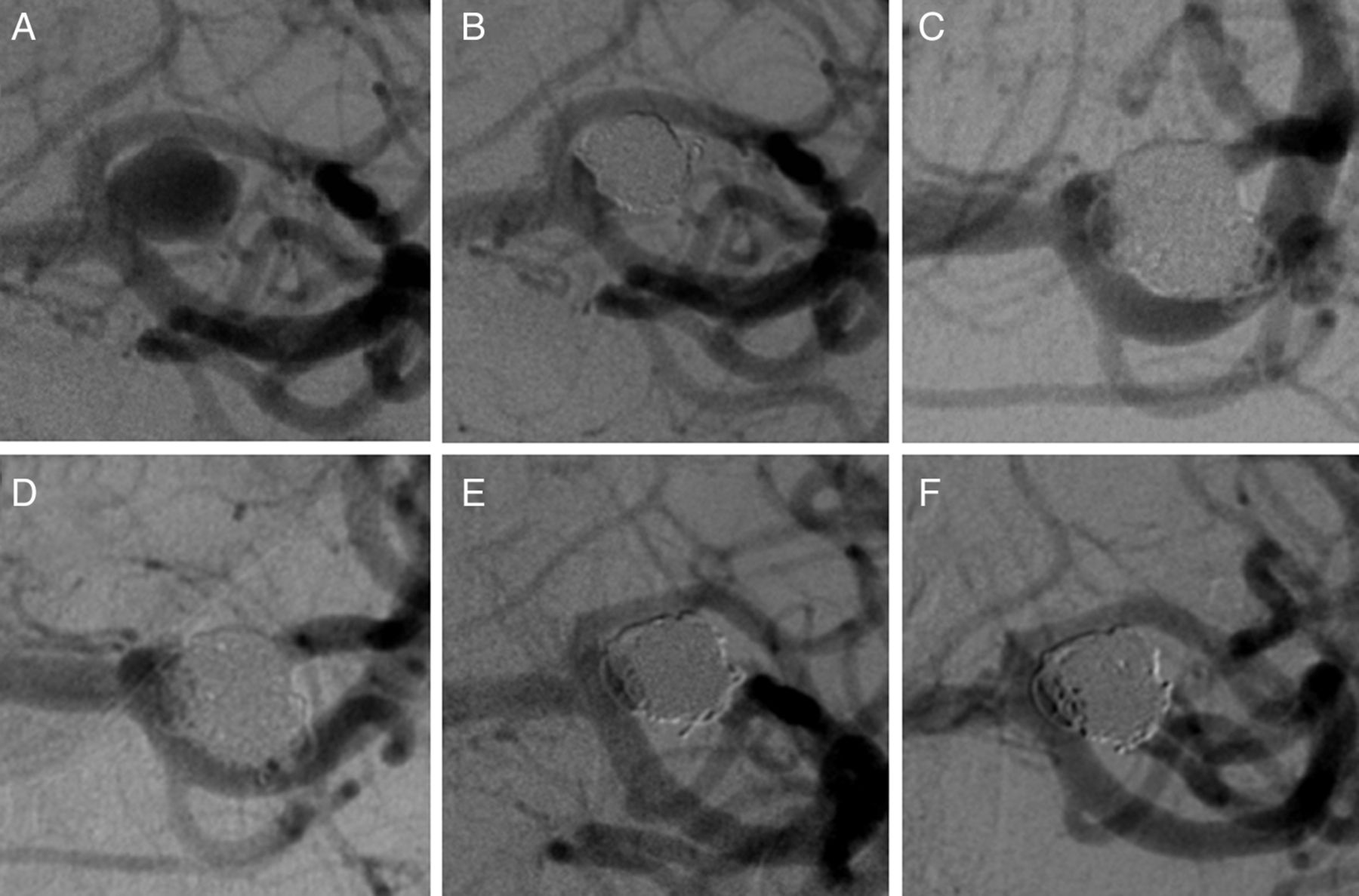
A second angiographic follow up was available for 36.4% of class I aneurysms at an average of 21.9 months and 37.4% of class II aneurysms at an average of 21.5 months. There were no recanalizations in either group at this time point. A delayed angiographic follow-up was available in 14.1% of class I aneurysms at an average of 44.4 months and 19.1% of class II aneurysms at an average of 57.1 months. No class I aneurysms and one class II aneurysm exhibited recanalization at this time point. Two aneurysms had very delayed follow-up at 8 and 9 years and displayed stability of the neck remnant (figures 1 and 2).
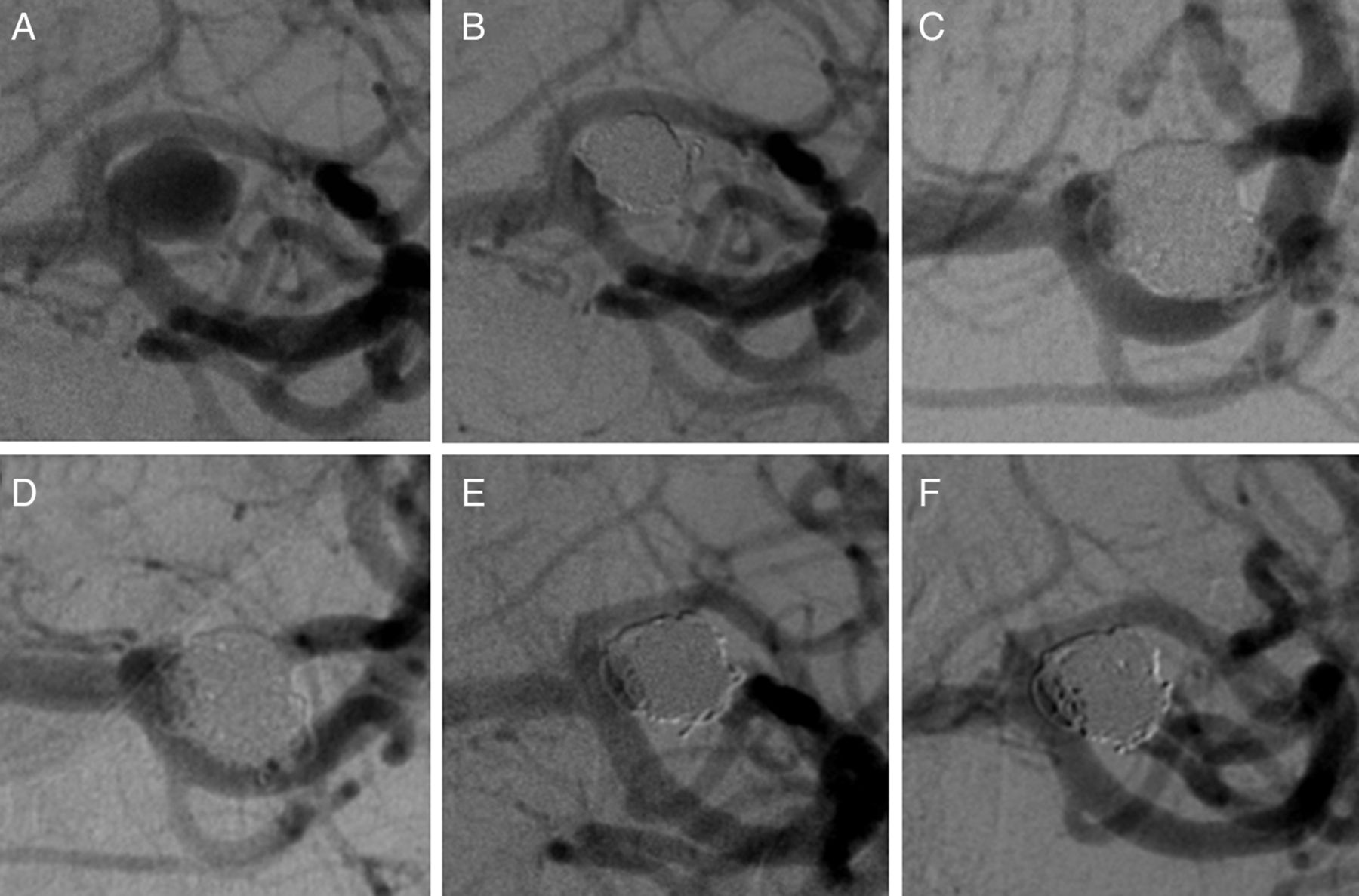
An unruptured left middle cerebral artery aneurysm (A) that was treated with stand-alone coiling. A neck remnant was allowed to prevent coil collapse and obstruction of either M2 branch (B). The neck remnant remained stable at 5 months (C), 18 months (D), 3 years (E) and 8 years (F).
{kind=link}
{kind=link}
A ruptured right posterior communicating artery (pcomm) aneurysm (A) that was treated with stand-alone coiling. A neck remnant was allowed to prevent occlusion of the pcomm that originated from the aneurysm neck (B). The neck remnant remained stable at 14 months (C), 3 years (D), 5 years (E), and 9 years (F).
Re-treatment and complications
The re-treatment rate was the same in both groups (class I 3.38% vs class II 8.5%; p=0.196). The adverse event rate was the same in both groups (class I 9.1% vs class II 4.5%, p=0.189) (table 5). There were also no differences in adverse events for either class I (p=0.807) or class II (p=0.285) when subdivided by categorical size. The rate of death or permanent disability secondary to the adverse event was the same in both groups (class I 4.0% vs class II 1.8%, p=0.337). There were no episodes of aneurysm rupture or re-rupture after treatment.
Adverse events
Discussion
Because aneurysm recanalization after coil embolization is not an insignificant problem,1– –4 it is important to understand which aneurysms have a higher risk of recurrence in order to guide initial and follow-up management. Certain studies have implicated the degree of aneurysm occlusion as being a significant determinant of risk of recanalization,6– –8 while others have suggested other factors such as aneurysm size, neck size, rupture status, aneurysm multiplicity, packing density, and time to follow-up.10– –12
Common sense would suggest that class II aneurysms should have a higher recanalization rate than class I aneurysms because there is residual filling of the neck that, over time, might transform into a recurrent aneurysm via coil compaction. On the contrary, this study shows that there is no difference between the recanalization rate of class I and class II aneurysms. Both groups were equally matched except that there were more internal carotid artery bifurcation aneurysms in the class I group. This finding may simply suggest that this particular aneurysm location is often amenable to achieving a RROC class I result.
Few studies have aimed to specifically evaluate the behavior of class II aneurysms. In 2000, Hayakawa et al13 investigated the natural history of 178 aneurysms with neck remnants after coil embolization. They found an overall 49% recanalization rate of class II aneurysms with large neck size and large aneurysm size, defined similarly to our study, were risk factors for recanalization. In 2006, Yamazaki et al,14 investigated the predictors of angiographic changes in neck remnants of ruptured aneurysms treated with GDC coils. Although the study population only included 37 class II aneurysms, they found an overall 48.6% recanalization rate with dome diameter and terminal aneurysm location being independent risk factors for recanalization.
A number of studies have evaluated the angiographic outcome of coiled aneurysms, but without specifically focusing on the outcome of class II aneurysms.6 ,7 ,15– –22 Among these studies, there is a wide range of recanalization among class II aneurysms, ranging from 0 to 49% with an average of 21.4% (table 6). Interestingly, the lower recanalization rates were seen in more recent studies, which may be a by-product of increased experience and improved adjunctive devices/techniques. In our study, we observed a low recanalization rate of 8.5% in the class II group that was not statistically different from that of the class I group. Furthermore, these recanalization rates were both lower than the overall recanalization rate of all coiled aneurysms of about 20% quoted in a large systematic review.2
Literature review
Although recent, large, prospective trials have suggested that coil embolization results in less morbidity than surgical clipping,1 ,4 coiling is not without its own set of complications including, but not limited to, aneurysm rupture,23 coil migration,24 vessel compromise, and cerebrovascular accident.25 The boundary between the aneurysm neck and the parent vessel is very small and coils can easily protrude or completely herniate out of the aneurysm neck into the parent vessel and cause vessel compromise and thromboembolic complications.
The knowledge that class II results are acceptable and often stable may allow the interventional neurosurgeon to feel comfortable about stopping the procedure with this result rather than taking the additional risk of placing coils in the neck and potentially compromising the parent vessels or causing a thromboembolic complication. In our study, the complication rates were not statistically different, and this may be a result of our overall approach as mentioned above, to not aggressively pack the neck with coils. Finally, the knowledge that class II results are often stable may decrease the number of invasive angiographic follow-ups that are necessary to assure stability.
This study is limited by its retrospective nature and the subjective nature of the RROC system. Although we report the complication, re-treatment, and post-treatment rupture rates, we do not report clinical follow-up, which is arguably more important than angiographic follow-up. The vast majority of aneurysms in this study are small and in the anterior circulation and the results may possibly only apply to these types of aneurysm (this is true, however, of many aneurysm studies).
While our study did not detect statistical differences between groups, there were trends towards higher recanalization and re-treatment in the class II group and higher adverse events in the class I group. These trends may become significant in a larger patient population with increased angiographic follow-up, and further investigation with a larger sample size is certainly warranted. In either scenario, the risk of recanalization should be weighed against the risk of an adverse event when faced with the decision to place additional coils in the aneurysm neck.
Conclusions
Our findings suggest that intracranial aneurysms with neck remnant following coil embolization have a natural history similar to that of completely occluded aneurysms with a low recanalization rate. This knowledge is useful and might help the interventional neurosurgeon avoid procedural complications such as coil herniation, vessel compromise, and stroke as well as predict which patients need closer angiographic follow-up. Further investigation with a larger patient population is warranted.
References
Footnotes
Contributors ABP, HM, and JRM conceived the study. JRM collected the data. ABP and HM performed the angiographic review. EKO carried out the statistical analysis and created the tables. RADL prepared the figures. JRM, EKO, and RADL prepared the manuscipt. All authors reviewed and corrected the manuscipt.
Competing interests ABP is a consultant for Penumbra. This disclosure is unrelated to the study.
Ethics approval Institutional review board.
Provenance and peer review Not commissioned; externally peer reviewed.