Article Text

Abstract
Background Large vessel occlusions are an important cause of ischemic stroke. Imaging goals center on identifying the site of occlusion, the size of the ischemic core and the size of the ischemic penumbra. The etiology of the occlusion is typically inferred by history and demographics, or subacutely during investigation for shunt, hypercoagulable state or other causes. Current generation vascular imaging is based primarily on lumenography. Contours of the vessel lumen on lumenography may suggest the presence of atherosclerosis, dissection or thrombus. High-resolution MRI (HRMRI) techniques can characterize wall morphology in the presence of an occlusion, which may affect clinical care by better definition of intra-occlusion wall characteristics as well as downstream vasculature normally confounded by the lack of antegrade flow.
Methods The HRMRI databases of Cleveland Clinic and Beijing Tiantan Hospital were reviewed to identify patients with large vessel occlusions on lumenography, performed with a diagnostic quality HRMRI. Clinical data were reviewed for each patient and images were analyzed by experienced neuroradiologists at both institutions. Where possible, conventional angiography/lumenography was reviewed for comparison.
Results Nine patients with large vessel cerebral artery occlusions were identified in whom HRMRI characteristics were reviewed and categorized. Images were correlated with demographics, risk factors and the working diagnosis of each case.
Conclusions HRMRI of vascular occlusions can identify wall characteristics and characterize the course and caliber of the vasculature distal to the occluded segment. This information may be useful in determining preferred approaches for endovascular revascularization.
- MRI
- Stroke
Statistics from Altmetric.com
Introduction
Lumenography in the setting of neurovascular ischemia may be useful in acute, subacute and chronic cases, and has been directed towards determining the site of occlusion and later towards the identification of collaterals and the pathway of collaterals in order to assess viability of downstream tissues. Lumenography can be performed via digital subtraction angiography (DSA), CT angiography (CTA) and MR angiography (MRA).1 The addition of time-resolved or four-dimensional (4D) evaluations of vasculature may add another component by improving assessment in slow-flow states.2
High-resolution MRI (HRMRI), primarily performed on 3 Tesla scanners, has been shown to be useful in the setting of vessel wall imaging, initially in the extracranial carotid arteries3 and later in the intracranial vasculature.4–6 Much of the intracranial work has centered on the identification of vasculitis as well as intracranial atherosclerosis.4 In theory, HRMRI may be able to improve the understanding of the type of occlusion present in a vessel, even before medical or endovascular intervention.
Methods
The HRMRI databases of Cleveland Clinic (n=246) and Beijing Tiantan Hospital (Department of Radiology, China-Japan Friendship Hospital, Beijing, China and Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China) (n=440) were searched in accordance with the institutional review boards of the respective institutions. The databases contain patients with heterogeneous diagnoses including aneurysms, dissections, subarachnoid hemorrhage, atherosclerosis, vasospasm, vasculitis as well as reversible cerebral vasoconstriction syndrome. Only patients with a large vessel occlusion on lumenography as well as a diagnostic quality HRMRI examination were included. Patients with incomplete imaging data or with demonstrable antegrade flow through the area of flow restriction were excluded, yielding 10 patients. Clinical data were reviewed for each patient and images analyzed by experienced neuroradiologists at both institutions. Where possible, conventional angiography/lumenography was reviewed for comparison.
High-resolution sequences
At the North American facility, all scans were obtained on 3 T whole body scanners (Skyra or Trio; Siemens, Erlangen, Germany) with a 20-channel coil. The protocol started with a standard multislab 3D time of flight (TOF)-MRA sequence centered in the circle of Willis for lumenographic identification of any stenosis. HR imaging used four T1-weighted spin-echo sequences in the coronal, axial and sagittal planes. The first was without contrast, followed by three with contrast (gadobutrol, Gadovist; Bayer Schering Pharma, Berlin, Germany): (1) a non-contrast T1 coronal 2 mm section with no gap (TR/TE=11/544 ms), matrix=256×256 and FOV=130×130 mm; (2) a post-gadolinium T1 coronal 2 mm section with no gap and fat suppression and a saturation band (TR/TE=11/544 ms), matrix=256×256 and FOV=130×130 mm; (3) a post-gadolinium T1 axial 2 mm section with no gap and fat suppression and a saturation band (TR/TE=11/750 ms), matrix=256×256 and FOV=130×130 mm; and (4) a post-gadolinium sagittal 2 mm section with a 0.4 mm gap and no fat suppression and a saturation band (TR/TE=10/600 ms), matrix = 256×256 and FOV=130×130 mm.7
At the Asian facility, cross-sectional imaging was performed on a 3 T MR scanner (Signa, Twinspeed 3 T, GE Healthcare, Milwaukee, Wisconsin, USA) and an eight-channel phased array head coil. 3D TOF-MRA was performed for imaging positioning. On the basis of the MRA, the scan plane was angled to ensure that the cross-sectional images were perpendicular to the M1 segment of the middle cerebral artery (MCA) with proton-weighted images of 12–17 sections acquired with an FSE sequence. The parameters for proton-weighted images were: TR/TE=4000/12.9 ms, FOV=16×16 cm, thickness=2 mm, matrix=384×256, NEX=2 and echo train length=10. The cross-sectional voxel size was 0.6×0.6 mm. Fat suppression was applied to reduce fat signal from the scalp. A zero-fill interpolation 512 matrix technique was used to enhance spatial resolution. Total imaging time was 7–10 min.8
Statistical methods
The McNemar test was used to assess the difference in the frequency of each of the five findings under (1) HRMRI versus DSA and (2) HRMRI versus MRA. Exact p values were calculated using the binomial distribution. A significance level of 0.05 was used for all analyses. As this was a preliminary study, no adjustment was made to control the type I error rate.
Results
Ten patients with large vessel occlusions were identified and their characteristics are summarized in table 1. All patients had total or near total occlusions with no demonstrable flow on at least one lumenographic examination. Given that definitive pathologic diagnosis cannot be obtained on any patient without necropsy, their HRMRI findings, probable diagnosis and differential diagnoses are summarized in table 2. Management and outcomes are summarized in table 3.
Patient characteristics
Vessel wall imaging
Management
Statistical results
For all 10 patients, the DSA and MRA findings were identical. HRMRI showed a higher frequency of wall thickening and wall enhancement compared with DSA and MRA (p=0.016 and p=0.008, respectively), and a similar trend was observed for the finding of stenosis (p=0.063). In each of the three patients available for comparison of embolus size, the finding was present in HRMRI and absent in both DSA and MRA (table 4).
Statistical analysis of findings
Imaging findings
Wall enhancement
Thin wall enhancement can be seen in the cavernous internal carotid artery (ICA) and normally terminates after this point. In the setting of an arterial occlusion, wall enhancement may be seen in an underlying atherosclerotic plaque as well as in vasculitis, both of which can theoretically result in occlusion. Limited experience (unpublished data) with dissections suggests that the walls of injured vessels enhance, are thickened, often with the presence of a demonstrable flap (figure 1).

T1 high-resolution MRI from patient 5 with heterogeneous high signal (white arrow) within the mid basilar artery at the point of occlusion. The exact nature of the high signal is uncertain with pathology, but was believed to represent high signal blood.
‘White snake sign’
Distal to the point of vessel occlusion in vessels that would not be imaged by TOF, the distal vessel lumen may be hyperintense on post-contrast T1 imaging using the described protocol. Because the MRI protocol employed at the North American facility uses a post-contrast T1-weighted image with a saturation pulse designed to null inflowing blood, slow flowing blood should not be suppressed, and it is believed that this yields the high intensity appearance on post-contrast HRMRI, contrasting distinctly with the proximal ‘black blood’. For instance, in the case shown in figure 2A–D, traversing the point of occlusion with a microcatheter into the area not seen on TOF but visible as high-intensity lumen on HRMRI was clear of thrombus. This finding may have several implications: (1) the imaged segment may not be completely filled with debris/clot or other material; or (2) the blood flow to that area is sufficiently slow so that it is not saturated. This information can offer insight into the length of an occlusion and the nearest ‘open’ segment (figure 2E,F).

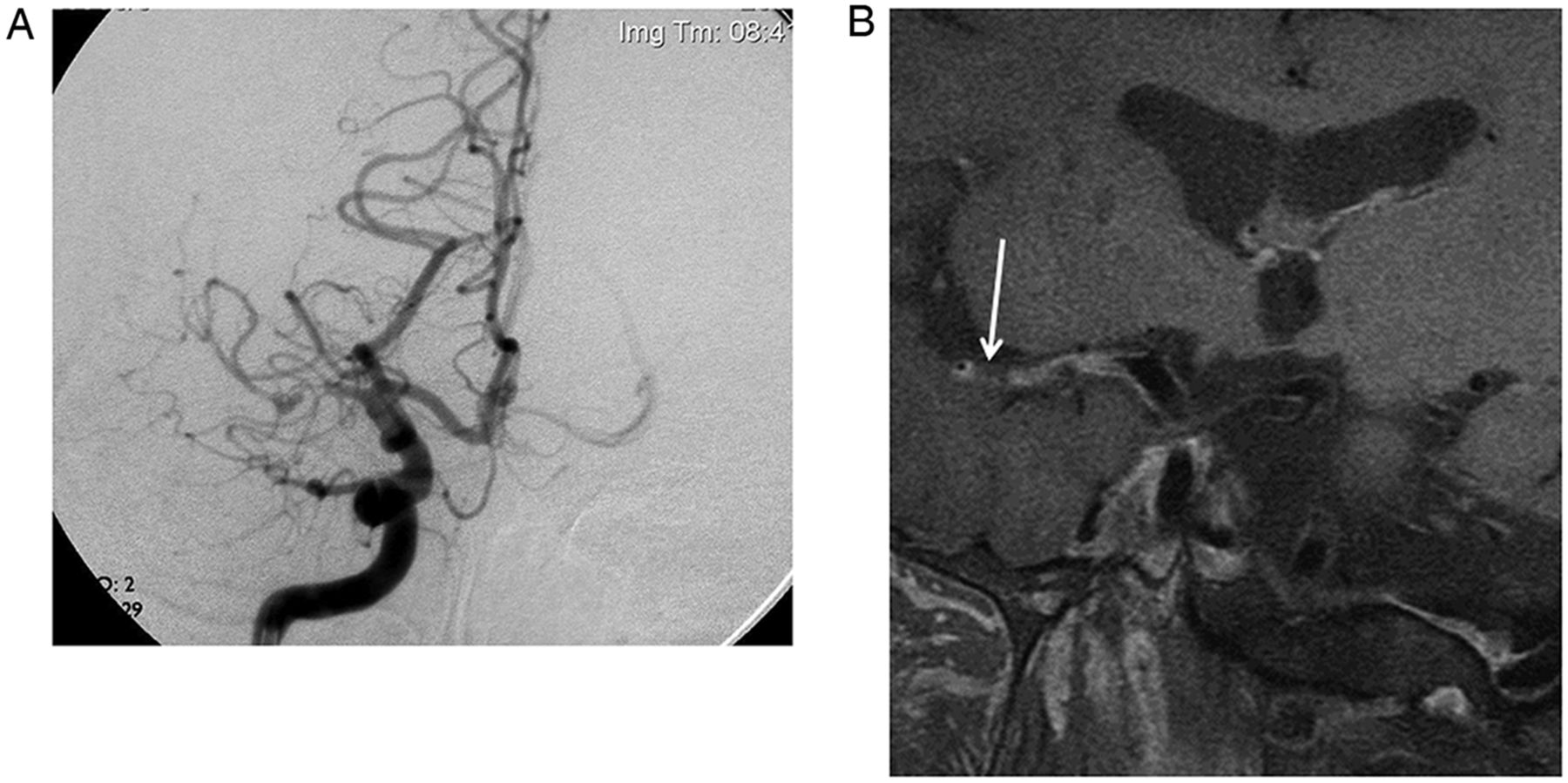
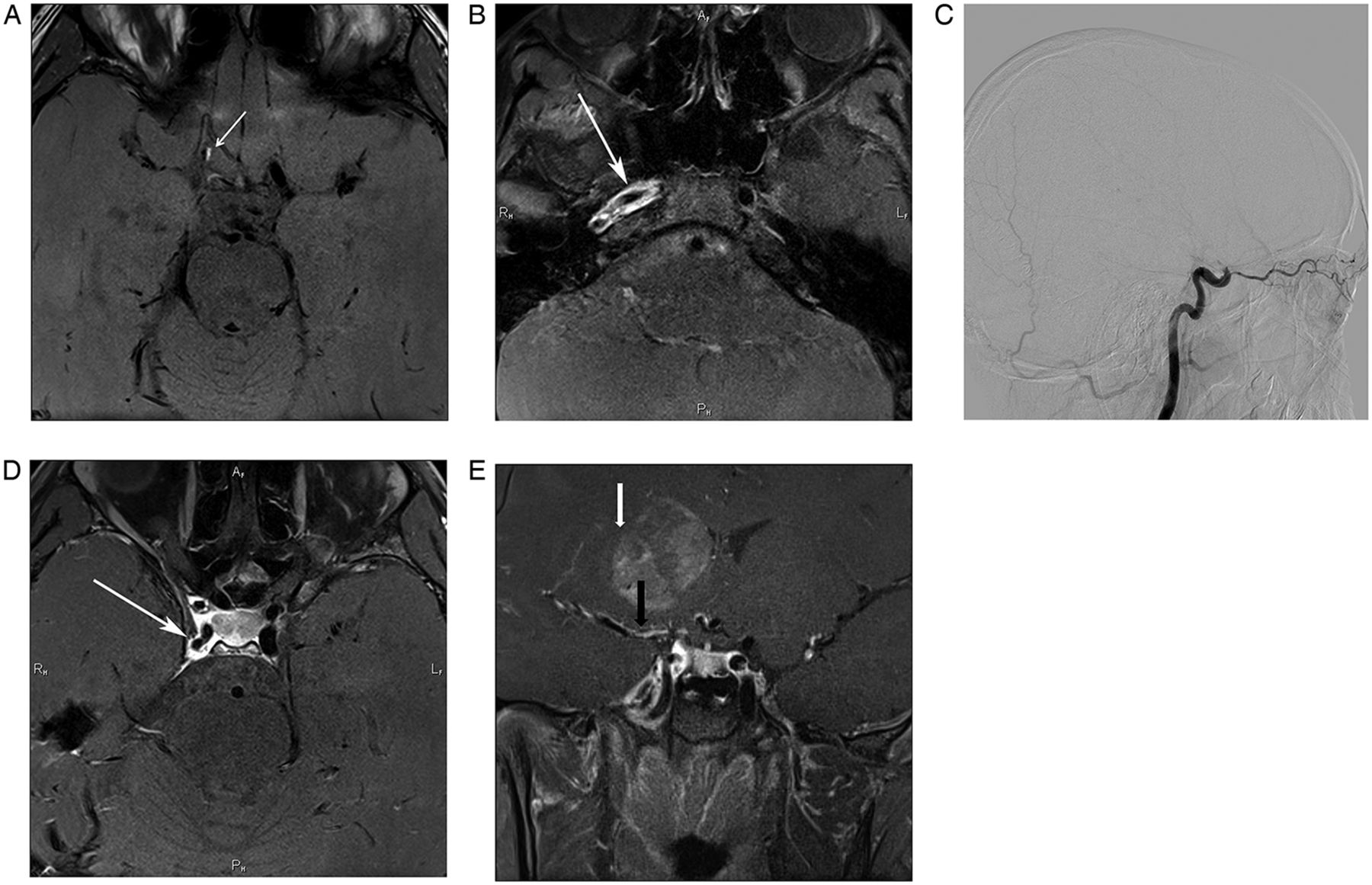
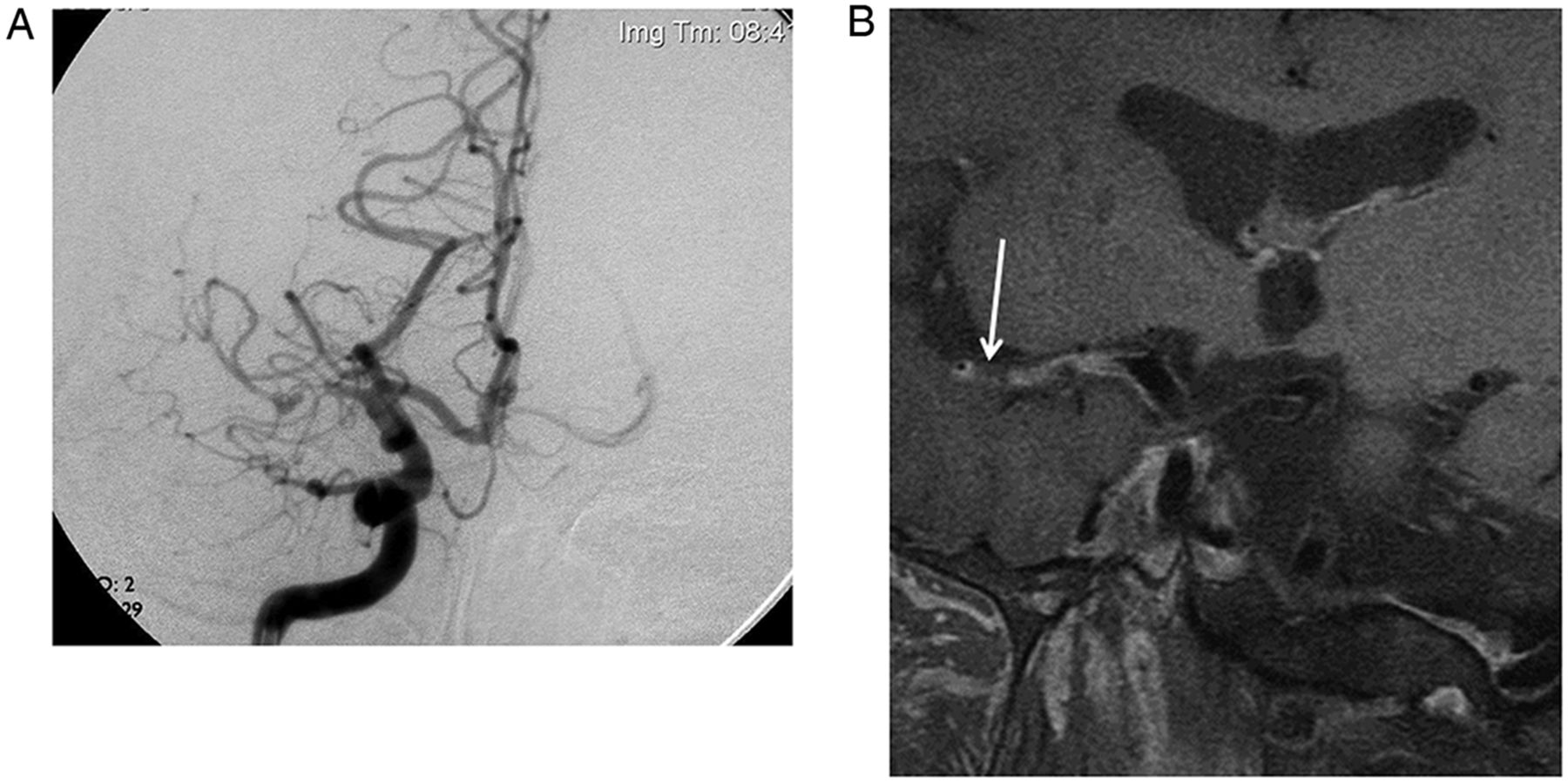
Examples of ‘white snake sign’. (A) Contrast-enhanced T1 high-resolution MRI (HRMRI) from patient 5 showing uniform high signal in the expected location of the post-posterior inferior cerebellar artery (PICA) right V4 segment (white arrow). (B) Conventional catheter angiography of the right vertebral artery does not opacify the post-PICA right V4 segment (white arrow). Subselective catheterization (not shown) demonstrated patency without thrombus. (C) Contrast-enhanced T1 HRMRI from patient 6 showing high signal in the vessel (arrow) distal to the point of occlusion that does not opacify on early frames during conventional digital subtraction angiography of the left internal carotid artery (D), only to fill later. Note the ‘black blood’ appearance of the proximal high-flow M1. (E) Contrast-enhanced T1 HRMRI showing pencil point thinning (arrow) of the vessel with wall enhancement, which may be of either atherostenotic or inflammatory nature. While the patient was initially stable, the patient subsequently declined neurologically. Information from the HRMRI led to direct stenting of the lesion (F).
Probable thrombus
Filling defects in areas of slow flow are starkly visible, such as in figures 3A–C and 4A–D. Limited experience with these findings makes differential characteristics in post-contrast imaging uncertain. Further experience may determine which imaging characteristics correlate with which kinds of thrombus, as well as interpreting enhancement characteristics. It is possible that further thrombus characterization may be able to provide information as to thrombus consistency and rigidity and ease of lysis and thrombectomy.
(A) Axial contrast-enhanced T1 high-resolution MRI (HRMRI) from patient 7 shows an interface and meniscus between a filling defect in a large slow flow vertebral artery which is predominantly filled with unsuppressed high signal gadolinium-enhanced blood. The arrow shows the interface between the filling defect and the vessel. (B) Coronal contrast-enhanced T1 HRMRI which shows the probable thrombus filling the distal vertebral artery and proximal basilar artery (white arrow) with resumption of suppressed blood in the mid basilar artery (double arrow). (C) Corresponding left vertebral artery injection which does not opacify the basilar or contralateral vessels.

(A) Contrast-enhanced T1 high-resolution MRI (HRMRI) through the level of the V4 segments showing patent flow void in the pre-posterior inferior cerebellar artery (PICA) left V4 in patient 8. Note the adjacent enhancing perivertebral venous plexus. Arrow points at irregular wall and patent flow evinced by ‘black blood’. (B) Delayed frames in a conventional digital subtraction angiogram in patient 8 shows the absence of the left P1 segment (top arrow), duplicated left superior cerebellar arteries and an irregular dissection of the left V4 pre-PICA segment (bottom arrow). (C) Contrast-enhanced T1 axial HRMRI through the level of the dissection showing irregularity and enhancement of the dissected segment on the left, and minimal lumen in an occluded right vertebral V4 segment on the right (arrow). Note the ‘black blood’ appearance in the anterior portion of the vessel and heterogeneous enhancing intensity of the posterolateral portion. (D) Contrast-enhanced T1 coronal HRMRI of the basilar artery showing white unsuppressed enhancing blood in the mid basilar artery with a filling defect extending into the left P1 segment (arrow).
Wall morphology and contour
Both outer and inner wall morphology can be assessed on HRMRI of blood vessels.4–6 ,9 The characteristics of the inner contour may indicate atherostenosis or post-inflammatory stenosis.4–6 ,9 At times, the outer contour of the vessel may also be narrowed.5 ,10 The implications and etiology of outer wall negative remodeling is uncertain, but may have implications for angioplasty and stenting. Figure 5A,B shows DSA and HRMRI of a vessel with atherostenosis, plaque and remodeling.
(A) Digital subtraction angiogram of the right internal carotid artery showing high-grade stenosis and subsequent occlusion of the right M1 segment. (B) Proton-weighted non-contrast high-resolution MRI of the right middle cerebral artery in plane showing wall thickening and narrowing, followed by high-grade stenosis then finally occlusion (arrow). Orthogonal images (not shown) eventually show lack of signal void in the middle of the vessel course.
Concentric wall enhancement and thickening
Concentric wall thickening and enhancement has been described as a finding associated with vasculitis.4 Swartz et al4 described the target sign as a circular area of enhancement and thickening when the imaging plane is oriented perpendicular to the vessel. In our experience, the target overlaps with findings in certain patients with a multitude of atherosclerotic risk factors. Differentiating vasculitic/vasculopathic wall enhancement from atherostenotic lesions is presently uncertain to this group. Angioplasty of such lesions may or may not be unavoidable in acute ischemic stroke, but the durability of the result would also be uncertain. Figure 2E shows a lesion with concentric wall thickening in a 49-year-old patient while the remaining vessels appear normal. It is uncertain whether the lesion was atherosclerotic or vasculopathic, both before and after angioplasty and stenting. However, in occlusions with wall thickening and stenosis, HRMRI may prompt operators to avoid using thrombectomy or thrombolytic approaches to revascularization and choose angioplasty or stenting before intervention even begins.
Venous enhancement
While not strictly abnormal, venous enhancement is common, probably related to slower flow, and these findings by interpreting physicians are important in case normal enhancement of venous structures is mistaken for pathologic enhancement of a blood vessel wall (figure 6A,B).

(A) Venous enhancement of the cavernous sinus around the suppressed cavernous carotid blood flow on contrast-enhanced T1 high resolution MRI (HRMRI). (B) Middle Sylvian vein tributary enhancement rather than pathologic wall enhancement (arrow) on contrast-enhanced T1 HRMRI.
Dissection
Limited experience in the imaging of dissected vessels may show wall enhancement. Our group currently describes findings as dissection only when a flap is identified. Gadolinium enhancement of non-suppressed slow flowing blood may make identification of an actual flap difficult. Use of non-enhanced T1-weighted imaging with flow suppression may help identify subintimal hemorrhage (figure 7A), while post-contrast images often show vessel wall enhancement in adjacent vessels (figure 7B–E). Of note, catheter angiography results in transient increases in endoluminal pressure local to the injection,11 raising the possibility of distension of an otherwise collapsed or partially collapsed vessel.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
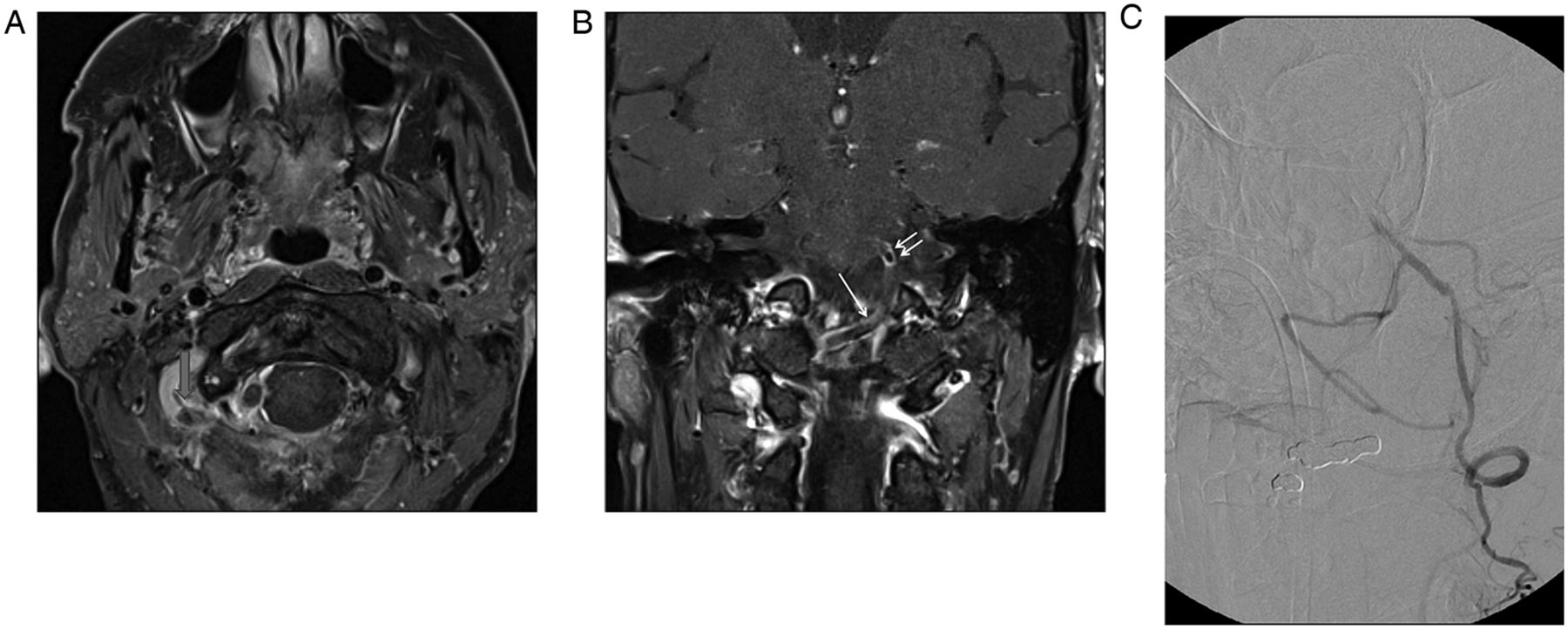
(A) Non-enhanced T1-weighted high-resolution MRI (HRMRI) of the supraclinoid internal carotid artery (ICA) in patient 9. Note the high signal in the right ICA supraclinoid segment, probably representing subintimal blood (arrow). (B) Axial contrast-enhanced T1 HRMRI post contrast at the level of the petrous bone showing enhancement of the wall and narrowing of the flow void in the right ICA (arrow). This may represent collapse of the vessel and expansion of the potential space around the ICA, as well as vessel wall enhancement. Comparison with angiography (C), which shows normal caliber in the aforementioned vessel with abrupt termination at the level of the observed dissection. (D) Axial contrast-enhanced T1 HRMRI showing narrowing of the cavernous segment in an enhancing cavernous sinus. (E) Coronal contrast-enhanced T1 HRMRI showing narrowing of the M1 segment with prominent venous drainage and possible wall enhancement (black arrow) as well as enhancement of a right basal gangliar infarct (white arrow).
Discussion
Vascular imaging in the setting of acute ischemic stroke and ischemic cerebrovascular disease has been performed largely to localize the site of the occlusion, leaving the interpreter to assess the probable nature of the occlusion by observing the luminal characteristics of the column of contrast within the vessel, be it iodine, gadolinium, flow-related enhancement or even carbon dioxide in earlier eras. Because these techniques intrinsically image what is in the vessel, the occluding object must be inferred.
Potential clinical impact
Both medical and endovascular revascularization is currently based on the assumption that the occlusion is thrombus.12 ,13 In the North American population it is likely that this assumption is correct, as many ischemic strokes result from emboli from carotid atherosclerotic disease, atrial fibrillation-related complications, intracardiac shunts, hypercoagulable states as well as idiopathic thrombi. On the other hand, it is possible that some idiopathic emboli are not emboli at all, and represent in situ vasculopathy, atherosclerosis or even an intracranial dissection. Given the high survival rates following ischemic stroke and the low rate of necropsy, a true understanding of the rate of these other causes of occlusion remains lacking.
In contrast, in populations in East Asia the rate of intracranial atherosclerosis is much higher and, as such, the ratio of intracranial vascular occlusions that are related to acute thrombosis related to an underlying atherosclerotic plaque might be much higher.14 ,15
Analyzing efficacy and outcome data after medical and endovascular interventions may be influenced adversely by grouping all of the above occlusions into the overall category of cerebrovascular occlusion. Given that response rates may differ with respect to different etiologies, accurate characterization of the nature of the occlusion may have implications in terms of selection of therapeutic modality and in subgroup analysis in clinical trials.
For instance, an MCA M1 occlusion due to in situ atherosclerosis with overlying acute thrombus may be best treated by direct stenting as a first-line treatment, whereas clot maceration, aspiration and extraction may prove to be preferential in bland clot. Similarly, intravenous tissue plasminogen activator may prove to be particularly ineffective in high-grade pre-existing atherosclerosis or in blocks of calcific emboli.
HRMRI may prove to better characterize the nature of the occlusion and the surrounding wall tissue than MRI or CT alone. Furthermore, HRMRI can characterize the vessel course and caliber distal to the occlusion as well as in areas of slow flow. This may be helpful in therapeutic planning, guiding a neurointerventionalist in the expected course of the wire and catheter behavior in segments invisible on DSA.
Limitations of study
The databases acquired by the two originating institutions contain patients primarily identified in the subacute setting, reflecting the present logistical difficulty in acquiring a highly specialized protocol in the acute emergency patient. Only one of the patients imaged appeared to have an occlusion due purely to an in situ embolus. The HRMRI appearance of such an embolus needs to be better defined, especially with regard to the time course of the occlusion.
As mentioned above, the pathological diagnosis is dependent on necropsy and thus is difficult to obtain. Definitive radiologic–pathologic correlation will depend on the acquisition of necropsy soon after imaging findings, although HRMRI may also be useful to show wall enhancement of extracranial vessels, aiding in identifying biopsy targets in surrogate sites such as the superficial temporal artery (unpublished data).
HRMRI in an acute setting is challenging and the imaging protocol is motion sensitive, so obtaining diagnostic quality imaging in uncooperative patients may be difficult. At present our institutions’ protocols require 7 min for a 2D HRMR acquisition in a single plane. Optimizing protocols for acute intervention may require omitting pre-contrast imaging.
Another limitation relates to the fact that the majority of patients imaged in our series were acquired in the early subacute phase; it is uncertain whether other findings may be more evident in the hyperacute or chronic phases in these disease states.
The statistical analysis performed yielded p values of <0.008 for wall enhancement on HRMRI versus MRA and DSA, and p<0.016 for wall thickening in the same comparison. This improved sensitivity in this small series without pathological correlate probably reflects the fact that wall thickening and enhancement are not ordinarily detectable on other imaging studies. However, the meaning of such a statistical finding is of questionable value given that only HRMRI can detect the finding in question.
Conclusions
HRMRI techniques can be used to characterize a vascular occlusion. The present small series demonstrates vessel wall characteristics at the site of occlusion, as well as luminal characteristics downstream. Imaging occlusions in the acute setting with rapid HRMRI protocols will require increased coordination, but may yield information helpful to both vascular neurologists and interventionalists in treatment and device selection as well as trial design. At present, HRMRI may serve as a problem-solving tool in quasi-stable patients with large vessel occlusions. Further research will be necessary to better define the variety of lesions that may cause large vessel occlusions as well as to establish radiologic/pathologic correlation.
Acknowledgments
The authors thank Christine Moore for her excellent editorial assistance.
References
Footnotes
FKH and XZ contributed equally to this work.
Contributors FKH: Conceived and designed the research. FKH, XZ, XL, W-JJ: Acquired the data. MSH, KU, JAB: Analyzed and interpreted the data. FKH: Draft the manuscript. FKH, XZ, W-JJ, MSH, SEJ: Made critical revisions of the manuscript. FKH, XZ, SEJ, KU, JAB, MSH, XL, W-JJ: Approved the final manuscript.
Competing interests None.
Ethics approval Ethics approval was obtained from Cleveland Clinic and Beijing Tiantan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.