Article Text

Abstract
Background Surgical clipping and endovascular coiling yield similar functional outcomes for the treatment of saccular aneurysms of the anterior communicating (ACOM) artery. However, surgical treatment may be associated with greater rates of cognitive impairment due to injury of adjacent structures. We aimed to quantify the rates of injury (infarction/hemorrhage) for both clipping and coiling of ACOM aneurysms.
Methods This was a retrospective dual-center radiological investigation of a consecutive series of patients with ruptured and unruptured ACOM aneurysms treated between January 2011 and October 2014. Post-treatment CT or MRI was assessed for new ischemic or hemorrhagic injury. Injury relating to the primary hemorrhage or vasospasm was differentiated. Univariate analysis using χ2 tests and multivariate analysis using binary logistic regression was used.
Results 66 patients treated with clipping were compared with 93 patients treated with coiling. 32/66 (48.5%) patients in the clipping group suffered treatment-related injury (31 ischemic, 1 hemorrhagic) compared with 4/93 (4.4%) patients in the coiling group (3 ischemic, 1 hemorrhagic) (p<0.0001). For patients with subarachnoid hemorrhage, the multivariate OR for infarction for clipping over coiling was 24.42 (95% CI 5.84 to 102.14), p<0.0001. The most common site of infarction was the basal forebrain (28/66 patients, 42.4%), with bilateral infarction in 4. There was injury of the septal/subcallosal region in 12/66 patients (18%).
Conclusions Clipping of ACOM aneurysms is associated with significantly higher rates of structural injury than coiling, and this may be a reason for superior cognitive outcomes in patients treated with coiling in previously published studies.
- Aneurysm
- Technique
- Coil
- CT
- Stroke
Statistics from Altmetric.com
Introduction
The anterior communicating (ACOM) artery represents the most common site for cerebral aneurysm formation and the most common site for ruptured aneurysms.1 The International Subarachnoid Aneurysm Trial demonstrated minimal differences in the rate of poor functional outcome or death between surgical clipping (SC) and endovascular coiling (EVC) for treatment of ruptured aneurysms at this location.2 However, patients may suffer significant cognitive impairment despite favorable functional outcome scores,3–5 and it has been recognized for some time that SC may be associated with greater rates of cognitive impairment than EVC for aneurysms treated at this location.6–8 A post-surgical syndrome of amnesia and confabulation is also recognized,9 although this may well be an oversimplification since various patterns of neuropsychological impairment can occur.10 A number of structures within the basal forebrain, basal ganglia, and limbic system are vulnerable to injury, probably through occlusion of anterior cerebral artery (ACA) or ACOM artery complex perforating branch vessels, notably the recurrent artery of Heubner (RAH) or subcallosal artery.11 ,12 Injuries to the basal forebrain and the fornix specifically have been implicated in resulting in memory impairment.11–18
We aimed to quantify the incidence of treatment-related injury for patients treated with SC and EVC in a consecutive series. We hypothesize that rates of local infarction are greater for patients who undergo SC than for those undergoing EVC procedures. We undertook a radiological review of consecutive patients undergoing treatment for both ruptured and unruptured ACOM aneurysms at two neurovascular centers to assess the rates of local injury for each treatment modality.
Methods
Consecutive patients with ACOM aneurysms treated between January 2011 and October 2014 at two neurovascular centers were included in the analysis. The treatment of both ruptured and unruptured aneurysms was assessed. Patients were treated by six neurovascular surgeons and three interventional neuroradiologists. The decision to clip or coil was not necessarily based on aneurysm morphology but was dependent on the philosophy of the admitting neurosurgeon, some advocating aggressive surgical management with others regularly referring for EVC. However, those lesions that were not favorable for EVC based on neck anatomy were referred for clip occlusion on a case-by-case basis.
CT imaging consisted of triplanar reconstructions acquired using 16–128 section machines. MRI consisted of FLAIR and/or T2 axial and coronal images acquired on 1.5 or 3 Tesla machines. Acute MRI included diffusion-weighted imaging. The presenting CT scan, post-treatment imaging (CT) performed 24–72 h after the aneurysm securing procedure, subsequent CT or MRI scan performed during the course of the patient's treatment, and eventual follow-up imaging at 4 weeks to 6 months was reviewed. Angiography at day 5–10 was also reviewed to record the presence of at least moderate ACA vasospasm (defined as >33% arterial narrowing). The presenting CT scan was interpreted for distribution of hemorrhage (Fisher grade, maximal clot thickness, intraventricular hemorrhage, and intraparenchymal hemorrhage) and presence of hydrocephalus. The surgical approach was assessed from analysis of the post-procedure CT scan. The endovascular technique was recorded from the intra-procedural imaging.
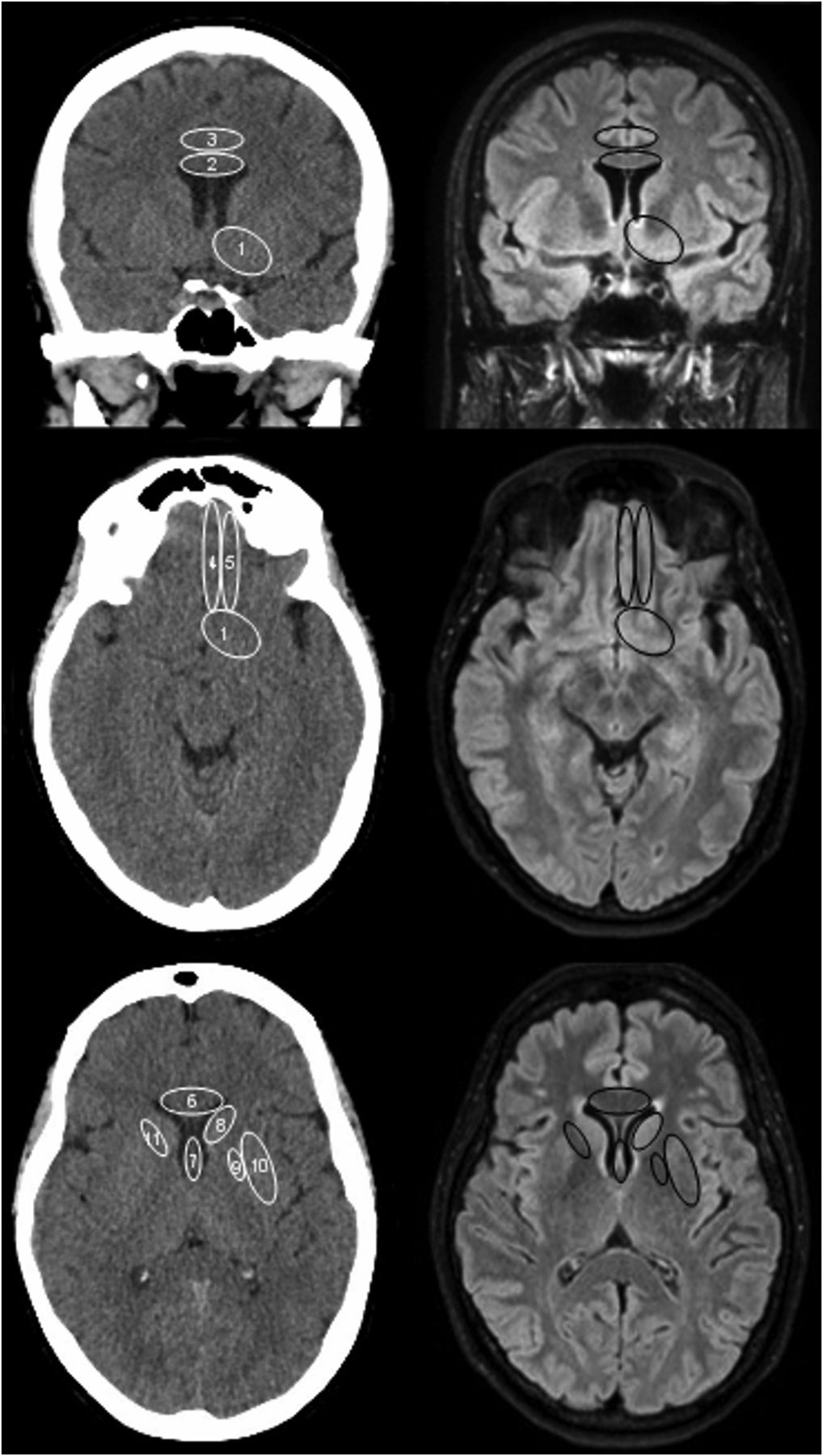
The location and rate of treatment-related infarction or hemorrhage was assessed on CT imaging performed 24–72 h after treatment (this was supplemented by MRI in two patients). Localization of injury was based on a standardized visual proforma (figure 1) to assess specific structures, but also included each ACA territory. Basal forebrain lesions were also specifically assessed for involvement of the more medial subcallosal or septal structures (figure 2). Treatment-related injury was defined as new hypodensity (ischemic injury) or hyperdensity (hemorrhage) on the post-treatment CT images. Where available, post-treatment MRI was also included in the assessment. If follow-up CT or MRI was available (MRI most commonly performed for post-coiling follow-up), this was cross-referenced with the post-treatment imaging for eventual gliosis to improve diagnostic certainty. CT hypodensities relating to ventricular drain insertion or hydrocephalus and those lying adjacent to hematomas were differentiated from new focal low density appearing on the post-treatment imaging. Low density in the perisylvian regions secondary to surgical access/retraction was not included in the analysis of treatment-related injury. Gyrus rectus hypodensity was categorized as having parenchymal injury whether secondary to infarction or resection, but was classified as ischemic injury rather than resection when the full length of the gyrus and adjacent gyri were involved whereas focal low density within the gyrus was categorized as resection, especially if a cavity containing gas was demonstrated. Infarcts secondary to the acute injury or vasospasm were also differentiated through co-analysis of the presenting CT scan and subsequent angiographic and CT imaging, respectively.

Proforma for identification of infarct location (multiplanar CT reconstructions, left and FLAIR axial and coronal images, right): (1) basal forebrain; (2) body of corpus callosum; (3) cingulate gyrus; (4) gyrus rectus; (5) medial olfactory gyrus; (6) genu of corpus callosum; (7) fornix; (8) caudate nucleus; (9) globus pallidus; (10) putamen; (11) anterior limb of internal capsule.
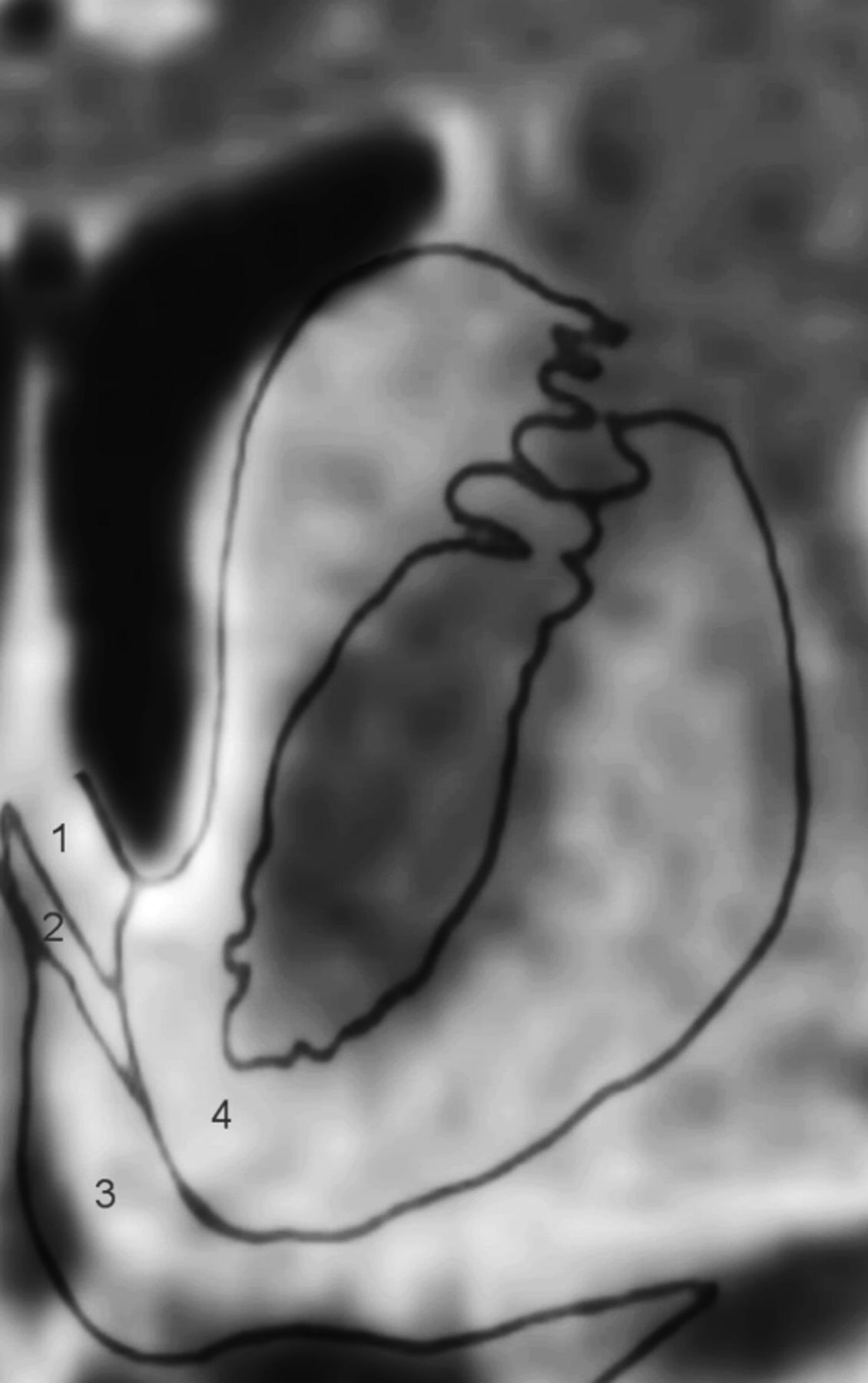
Structures within the basal forebrain: (1) septum; (2) diagonal band of Brocca; (3) subcallosal area; (4) nucleus accumbens.
The data were compared using univariate and multivariate analysis. Univariate analysis was undertaken using analysis of variance for continuous variables and χ2 tests for non-parametric data. Multivariate analysis was also undertaken for variables impacting on treatment-related injury in the group with subarachnoid hemorrhage (SAH) using binary logistic regression. Statistical significance was defined as a p value <0.05.
Results
Sixty-six patients who underwent SC were compared with 93 patients treated with EVC. Of the SC patients, 45 (71.2%) presented with SAH compared with 75 (80.6%) of the EVC patients. Descriptive statistics for each treatment modality are shown in table 1. There was no significant difference in the baseline parameters or in the rate of moderate to severe vasospasm. Nine of the 66 SC patients and 39 of the 93 EVC patients had follow-up MRI available in addition to CT.
Baseline characteristics of the study groups
The balloon-assisted coiling technique was used in 63 patients (67.7%), simple coiling in 23 (24.7%), and stent-assisted coiling in 7 (7.5%). In the surgical group, a modified orbito-zygomatic approach was used in 41 (62.1%) patients and a fronto-temporal approach in 25 patients (37.9%).
Thirty-two of the 66 (48.5%) patients in the SC group demonstrated local post-treatment injury. Eight of 21 (38.1%) patients with unruptured aneurysms and 24 of 45 (53.3%) patients with ruptured aneurysms developed injury following a clipping procedure (p=0.2485). Four of the 93 patients in the EVC group developed treatment-related injury (4.4%). All patients had suffered SAH. The distribution of lesions is shown in table 2. In one patient in each of the SC and EVC groups, this was due to a peri-procedural hemorrhage rather than infarction.
Distribution of treatment-related injury for clipped and coiled patients
The median number of regions involved per patient in the SC group was three. Nineteen of 41 patients (46.3%) with a modified orbitozygomatic approach and 13/25 (52%) with a frontotemporal approach suffered injury (p=0.6554). For ruptured aneurysms, SC was a stronger predictor of treatment-related infarction than EVC on multivariate analysis (OR 24.42, 95% CI 5.84 to 102.14, p<0.0001), along with large aneurysm size (≥10 mm) (OR 6.73, 95% CI 1.08 to 41.98, p<0.05) when taking into account aneurysm neck width, local hematoma width (≥10 mm), intraparenchymal extension of hemorrhage, intraventricular extension of hemorrhage, and older patient age (≥65 years) (see table 3).
Multivariate ORs for treatment-related infarction for patients with treated ruptured anterior communicating artery aneurysms
The site of the most common lesion was the basal forebrain (28 patients with 33 lesions, bilateral in four patients). The basal forebrain lesion was present on the side of the approach in 25/28 (88.9%) patients. Basal forebrain lesions were accompanied by caudate head lesions in 9/28 cases (figure 3). This was the next most common site for treatment-related injury. Injury to the basal forebrain occupied or extended into the more medial subcallosal or septal region in 12 patients in the SC group. The fornix and genu of corpus callosum lesions were seen in five (7.5%) and seven (10.6%) of the 66 SC patients and in three (3.3%) of the 93 EVC patients (figure 4). Gyrus rectus lesions were classified as ischemic in six of nine patients and after resection in three.

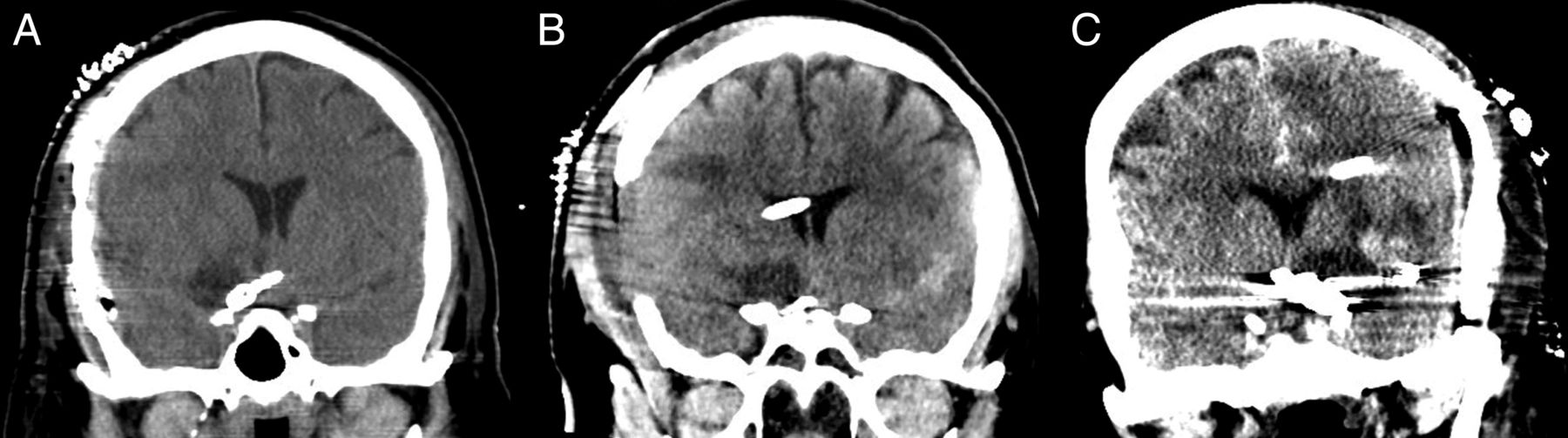
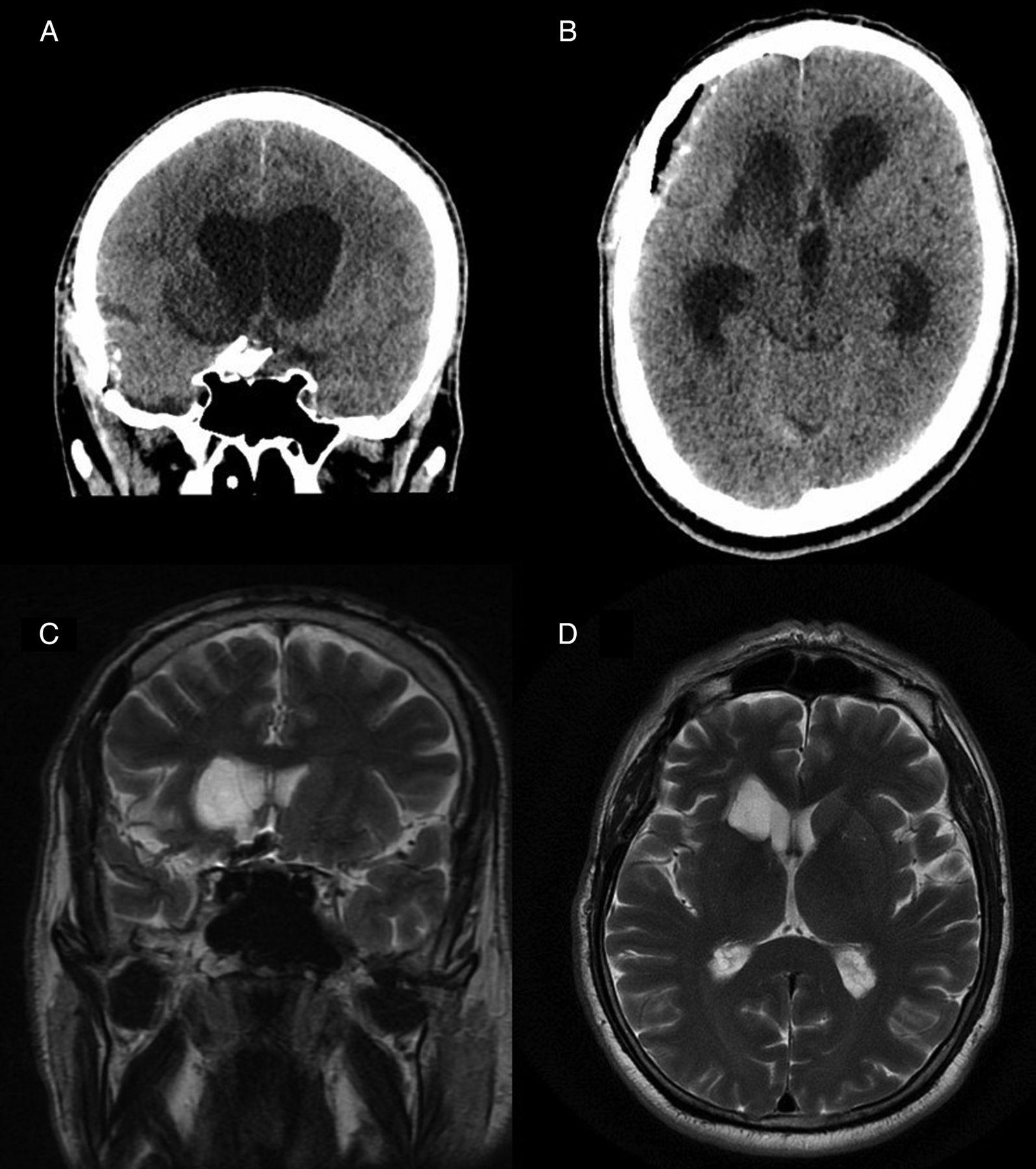
Coronal (A) and axial (B) CT demonstrating right caudate nucleus, anterior limb or internal capsule, and putaminal infarct extending into the region of the nucleus accumbens. T2-weighted MR coronal (C) and axial (D) images in a different patient demonstrate a similar pattern.

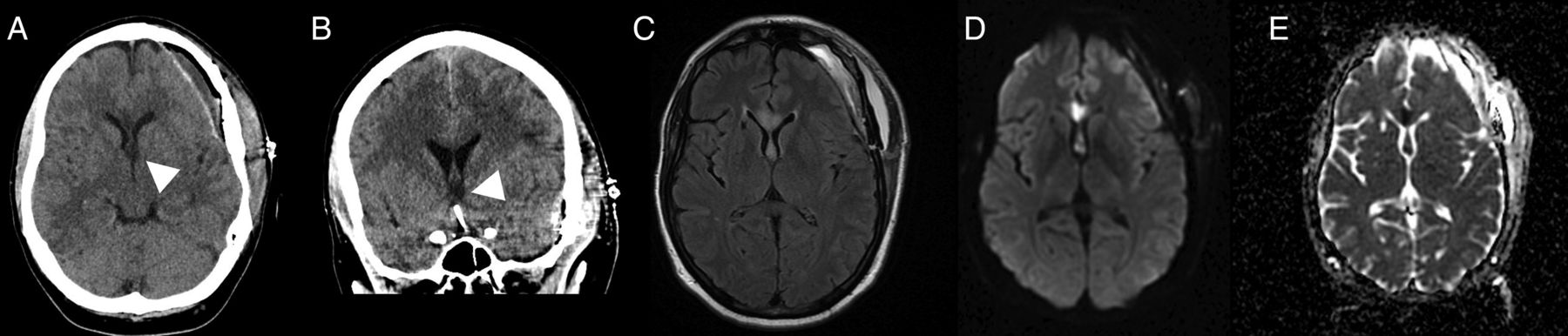
Axial (A) and coronal (B) CT demonstrating low density in the genu of the corpus callosum, fornix and subcallosal region indicative of an ischemic injury. Axial FLAIR (C), diffusion-weighted imaging (D), and apparent diffusion coefficient maps (E) demonstrating forniceal and genu of corpus callosum infarction.
Several patterns of infarction were recognized. These included:
basal forebrain injury associated with caudate, internal capsule, and lentiform nucleus injury akin to the territory of the RAH (figure 3);
septal/subcallosal infarction in association with forniceal and genu of corpus callosum infarction akin to the territory of the subcallosal artery (figure 4);
unilateral subcallosal infarction (figure 5);
unilateral basal forebrain injury involving the nucleus accumbens but sparing the subcallosal/septal region (figure 6);
a combination of any of the above patterns (figure 7);
body of corpus callosum infarction (figure 8).

Axial FLAIR (A) and T2 coronal (B and C) images demonstrating ischemic injury to the right septal and subcallosal region. Note also the high signal in the contralateral left subcallosal region, although this is less marked. Coronal CT reconstructions (D–F) in three additional patients with a similar pattern of infarction.
Coronal CT reconstructions in three different patients (A–C) demonstrating low density in the basal forebrain involving the region of the nucleus accumbens.
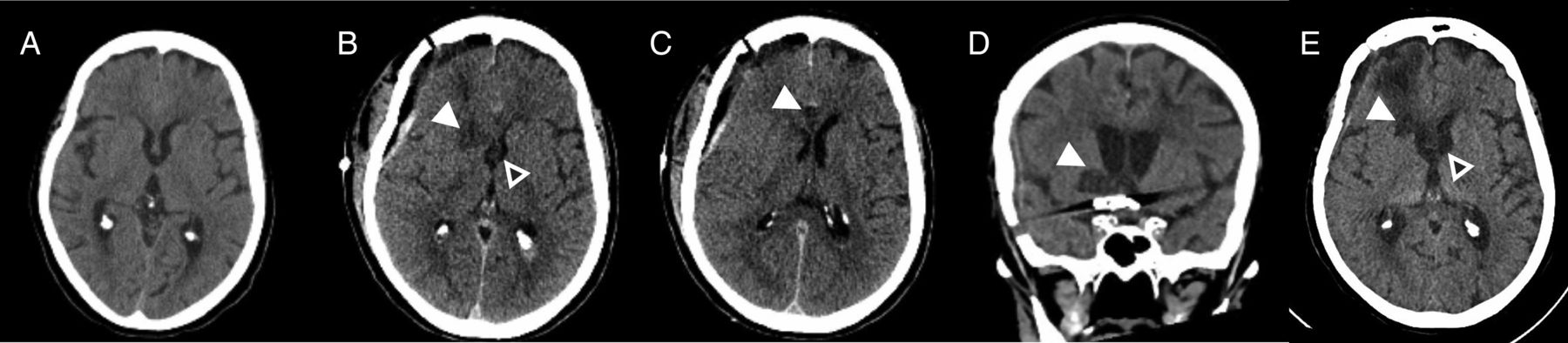
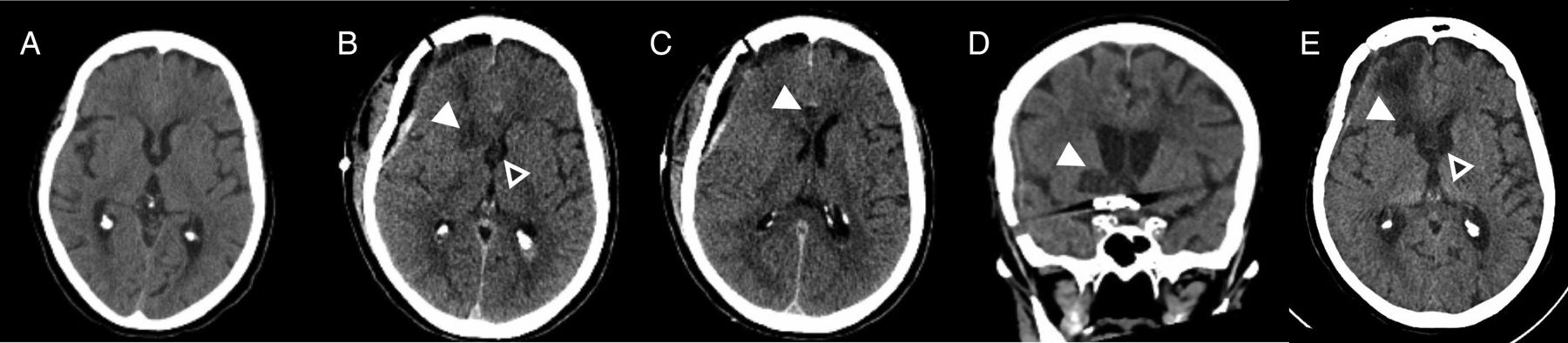
Baseline axial CT (A) and immediate post-clipping axial CT scans (B and C) demonstrating right caudate/basal forebrain infarction (white arrowhead) with forniceal (hollow arrowhead) and genu of corpus callosum infarction (white arrowhead). Follow-up coronal (D) and axial CT scans (E) demonstrating right basal forebrain infarct extending into the right septal region (white arrowhead), right caudate and internal capsule infarct (white arrowhead) and forniceal infarct (hollow arrowhead).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sagittal CT reconstructions in three different patients (A–C) demonstrating body of corpus callosum infarction (white arrowheads).
Discussion
It has been demonstrated in several studies that SC may result in inferior cognitive outcomes following treatment of ACOM aneurysms.6–8 Domains of memory, attentional, and executive functions may be affected. A number of case reports and series have suggested that lesions of the basal forebrain and/or fornix are predominantly responsible for memory deficits.10–18 Prefrontal lesions may be associated with attentional, executive, and psychopathological dysfunctions.10 We aimed to quantify the difference in the rate of treatment-related structural injury for SC and EVC of both ruptured and unruptured aneurysms. In a consecutive population of patients with treated ACOM aneurysms, the rate of local treatment-related injury was significantly greater in the SC group than in the EVC group. Forty-nine per cent of the SC group versus 4.4% of the EVC group had treatment-related injury. Clipping was a strong predictor of treatment-related injury on multivariate analysis. The infarct rate for coiling was in line with a recent systematic review of the literature.19 The majority of the surgical lesions were probably ischemic in etiology; most were on the side of the surgical approach. One possibility is that the clip(s) may result in compromise of adjacent minute perforators, that perforators need to be sacrificed to access the aneurysm, or that the direct exposure and handling of the artery may result in subsequent ischemic lesions.
The most common site of infarction was the basal forebrain with approximately 42% of patients in the SC group suffering injury to this location; 14% of patients in the SC group also suffered infarction of the caudate nucleus. Other authors have demonstrated that clipping represents an independent risk factor on multivariate analysis for postoperative ACA territory infarction.20 The finding of such a high rate of treatment-related ischemic injury in this series is surprising. A review of all-cause infarction at all locations in clipped patients treated in the tirilizad trials demonstrated that 707 (27%) out of 2741 patients developed cerebral infarction,21 but other authors have recognized high rates of postoperative infarction in patients with ACOM artery aneurysms.8 ,22 Using CT imaging, Umredkar et al22 demonstrated a postoperative infarct rate of 42.5% in patients with SAH who underwent SC. The current study could be criticized for relying on CT hypodensity for diagnosis in the majority of patients. There is a possibility that postoperative edema could limit specificity. However, where subsequent follow-up imaging was available, these regions demonstrated residual low density and/or atrophy implying regions of permanent structural injury. Use of triplanar imaging could have resulted in a greater rate of lesion pick-up compared with studies using axial imaging only. Additionally, there were recurring patterns of hypodensity in regions not normally subject to retraction or resection in the majority. Furthermore, our findings are in keeping with those of a cohort of 50 patients (14 EVC, 36 SC) in whom a significantly greater number of SC patients suffered foci of encephalomalacia on follow-up MRI.8 In that series, 33% of SC patients had basal forebrain lesions, 28% corpus callosum lesions, 11% caudate lesions, and 64% had frontobasal lesions.
An additional finding in this study was that infarction of structures presumed to be supplied by ACOM perforators including the subcallosal artery was greater in the SC group; lesions of the septal or subcallosal area that may harbor structures more vital with regard to memory10 ,23 were seen in 12 SC patients (18%) and one EVC patient (1.1%). Infarcts of the fornix (7.5% vs 1.1%) and genu of the corpus callosum (10.5% vs 3.3%) were also more common in the SC patients. We suspect that this may well be an underestimation of the true incidence of subcallosal artery or ACOM perforator disruption since MRI was not used universally or acutely. Interestingly, it also illustrates that these vessels can rarely be vulnerable during EVC procedures, although perhaps less often than in SC procedures.
We noted a number of patterns of infarction (figures 3⇑⇑⇑⇑–8): (1) more lateral basal forebrain injury sparing the septal and subcallosal structures but involving the nucleus accumbens; (2) basal forebrain injury in addition to caudate, internal capsule and lentiform nucleus injury; (3) isolated basal forebrain injury involving the septal and subcallosal structures unilaterally; (4) fornix, subcallosal region and genu of corpus callosum; and (5) body of corpus callosum infarction. We suggest that the first two patterns are secondary to either A1 or A2 perforators or RAH disruption and the latter three patterns are due to disruption of subcallosal artery, median callosal artery, or other ACOM artery perforators.
Perforators may arise from the A1 and A2 ACA; 2–15 perforating arteries travel superiorly and posteriorly from the A1 into the anterior perforated substance.24 Additionally, perforating branches of the A2 segment are located along the first 5 mm of the vessel and penetrate the brain at the gyrus rectus and olfactory sulcus.24 The most important perforator is the RAH. This vessel doubles back on its parent ACA and passes above the carotid bifurcation and middle cerebral artery into the medial part of the sylvian fissure before entering the anterior perforated substance. In a more recent autopsy study25 the RAH was found as a single vessel in 77%, as double arteries in 17%, and was absent in 6%. The origin of the RAH was from the junction of the ACA and ACOM artery in 62.3%, from the proximal A2 segment in 23.3%, and from the A1 segment in 14.3%. Both the length and diameter of the vessel can vary widely. During surgery the vessel is liable to injury during elevation of the frontal lobe from the optic nerve and chiasm or during exposure of the A2 segments.26 Occlusion of the RAH may result in infarction of the caudate head, anterior limb of the internal capsule, putamen, globus pallidus and basal forebrain.
The ACOM artery perforators are highly variable in number and territory supplied.27 Broadly, they can be categorized as hypothalamic, subcallosal, and median callosal and may vary in number from 0 to 11.27 ,28 The subcallosal artery and the implications of occlusion have been described in two recent case series.11 ,12 This is usually a single vessel and typically the largest of the arteries arising from the ACOM artery. The subcallosal artery supplies the bilateral subcallosal areas, but also the bilateral columns of the fornix and the genu of the corpus callosum. It may extend to the body of the corpus callosum and is therefore recognized as the medial callosal artery.28 The unilateral subcallosal infarction recognized in this study is not consistent with previous descriptions of the subcallosal perforators since a bilateral supply is often stressed in descriptions of these vessels.27 ,28 However, we were using CT to assess many of these patients, and limitations in sensitivity for ischemic changes in relatively small structures (whereby less marked contralateral ischemia was present but not recognized) could account for this finding (see figure 5).
The basal forebrain contains a number of structures that are believed to play a role in cognition. These include the nucleus accumbens, substantia innominata, nucleus basalis of Meynert, and medial septal-diagonal band of the Brocca complex.23 Basal forebrain lesions have been linked to the occurrence of amnesia and/or confabulation in a number of case reports and series,10 ,13–18 and a functional imaging study has also suggested that the basal forebrain is likely to play a role in episodic memory recall.29 The medial septal-diagonal band of the Brocca complex region is likely to be an important interface within the so-called septohippocampal system.10 Bilateral basal forebrain lesions do produce more severe memory deficits.10
The fornix is a compact fiber bundle connecting the hippocampus with the hypothalamus and a number of other structures including the septal area of the basal forebrain. It is an important constituent of the Papez circuit and is involved in the formation and consolidation of declarative memories.11 Diffusion-weighted MRI-proven infarction limited to the fornices has been reported in conjunction with acute onset of amnesia, suggesting that an isolated injury to this structure may be critical.12 Injuries to other vulnerable structures including the corpus callosum and caudate nucleus have also been implicated in resulting in neurobehavioural sequelae.30 ,31 Caudate nucleus lesions may result in depression, agitation, abulia, neglect (right-sided lesions), memory disturbance (particularly if bilateral), dysarthria, aphasia (left-sided lesions), movement disorders (ballistic, choreatiform), or motor weakness.32 There is controversy as to the role of the gyrus rectus in cognition, particularly as the gyrus rectus is deliberately resected to gain access to the aneurysm on occasions.26 An association between memory quotient and gyrus rectus resection was demonstrated in a neuropsychological analysis of 32 patients with clipped ACOM artery aneurysms.33 Other studies have failed to demonstrate an association.10 ,34
A number of studies have found significantly increased rates of cognitive impairment in patients with ACOM artery aneurysms treated with SC as opposed to EVC. Chan et al6 studied 18 patients who had undergone treatment for ruptured ACOM aneurysms, half with SC and half with EVC; 33% of the SC patients showed severe impairment of memory and executive function whereas no EVC patient demonstrated this impairment. Fontanella et al7 assessed 37 consecutive WFNS grade I or II patients who underwent treatment of ACOM aneurysms within 48 h of rupture; 20 of 37 were treated with SC and 17 were treated with EVC. Both groups were compared with 16 angiogram-negative patients with SAH and 18 normal controls. All patients were neurologically intact at discharge and were Glasgow Outcome Scale 1 at 6-month follow-up after SAH. Surgically treated patients showed a significant worse performance on the logical memory and on the frontal lobe executive functions compared with controls, while the endovascular group and the angiogram-negative group showed a significant decrease only in the literal fluency score. Furthermore, the surgical group showed a significant impairment in using grammatical and syntactical rules to produce sentences. Proust et al8 studied 36 SC and 14 EVC patients at 14-month follow-up. They found no difference in executive dysfunction although there was a significant impairment of verbal memory in the SC group.
These results raise the question of how to optimize patient treatment in future. However, while cognition is a factor that may impact on a patient's life, it needs to be weighed against other factors such as safely securing the aneurysm and durability of treatment. Balloon assistance has increased the number of patients who can be treated using the endovascular techniques without a significant increase in complication rate.35 For elective cases, a number of case series have described success in stent-coiling at the ACOM location.36 ,37 In the largest series comprising 64 patients37 the morbidity was 1.6% and mortality was 1.6%; 5.5% required retreatment. A systematic review of stent-coiling at all locations in patients with SAH who were managed with dual antiplatelet therapy demonstrated clinically significant intracranial hemorrhagic complications in 27 (8%) of 339 patients, including 9 (10%) of 90 patients known to have had ventricular drain-related hemorrhages. Clinically significant thromboembolic events occurred in 16 (6%) of 288 patients.38 Perhaps a trial comparing more aggressive endovascular approaches (eg, using stents or even flow diversion) with SC for less favorable aneurysms, particularly for locations such as this, would be worthwhile. Such a study should include neuropsychological testing as part of the outcome measures.
Limitations of the study
This was a retrospective study of a relatively small patient sample reflecting practice at two centers only. There was inherent bias as to which patients were selected for EVC or SC. Some aneurysms were referred for SC on the basis of being morphologically challenging for endovascular treatment whereas others were selected for SC on the philosophy of the managing neurosurgeon, some favoring surgical management. It is conceivable that the rate of infarction for EVC patients would have been greater if less favorable aneurysms were treated using an endovascular approach. The imaging assessment was predominantly with CT, which has an inherent lack of sensitivity for identification of lesions in this anatomical region, especially in the presence of clip or coil artifact. Another potential source of error was the limited specificity of CT hypodensity for infarction. In the absence of diffusion-weighted MRI, it could be claimed that a proportion of the focal hypodensities noted could represent postoperative edema. We were also unable to assess the rate of microinfarction with diffusion imaging that is known to complicate endovascular procedures. However, follow-up MRI was available for many EVC patients and we believe that, if MRI was available for all SC patients, then the differences in the rate of structural injury may have been more marked. At this stage we do not have cognitive test scores available for this cohort with which to assess the neurophyschological significance of the radiological findings, and we can only hypothesize based on other reports in the literature as discussed. It is possible that many patients did not suffer overtly clinically detectable neurocognitive deficits despite the high rate of injury as few SC patients were imaged with MRI during their postoperative course.
Conclusion
This retrospective analysis suggests that the degree of structural damage in regions known to impact on the cognitive outcome of the patient incurred through treating ACOM aneurysms using SC is significantly greater than that for EVC. Further work is necessary to assess the direct effect on cognitive outcomes.
References
Footnotes
Contributors All authors contributed to the manuscript and study.
Competing interests None.
Ethics approval The study was approved by the Northern Sydney and Central Coast Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.