Article Text

Abstract
Background Flow diversion represents a novel but definitive treatment for recurrent and difficult-to-coil aneurysms of the anterior communicating artery (ACoA) region, of which reports are limited.
Objective To determine the effectiveness of the Pipeline embolization device (PED) in treating aneurysms in the ACoA region.
Methods We retrospectively reviewed an IRB-approved database of patients with an aneurysm at a single institution for patients with ACoA or A1–A2 aneurysms treated with PED. Data analyzed included demographics, aneurysm characteristics, procedural details, follow-up results, and outcomes.
Results A total of 50 procedures were performed on 41 patients, including seven patients who underwent bilateral ‘H-pipe’ PED placement. The average age was 56 years and 46% of the patients were female. The average aneurysm size was 4.5 mm, and two large (>10 mm) aneurysms were treated. The vessel of origin was either the ACoA (26 aneurysms, 63%) or the A1–A2 junction (15 aneurysms, 37%). Eighteen patients (44%) had prior subarachnoid hemorrhage and 20 had previously been treated either with clipping (6 aneurysms, 15%) or coiling (14 aneurysms, 34%). Procedural success was achieved in 48/50 cases (96%) and two cases were aborted. Coils were deployed adjunctively in two cases (4%). Procedural outcomes included no deaths, one major ischemic stroke (2%), and two patients with intracranial hemorrhage (4%). Complete aneurysm occlusion was achieved in 81% of patients at 6 months and 85% of patients at last follow-up digital subtraction angiography.
Conclusions The PED can be used safely and effectively in the treatment of aneurysms of the ACoA region. This represents a good alternative treatment option to microsurgical clipping and endovascular coiling.
- Flow Diverter
- Aneurysm
- Technique
Statistics from Altmetric.com
Introduction
The anterior communicating artery (ACoA) region is a common site for cerebral aneurysms, and these aneurysms account for a disproportionate share of subarachnoid hemorrhage (SAH).1 Among unruptured aneurysms, ACoA aneurysms are at increased risk of rupture at smaller sizes2 ,3 and thus are routinely treated. Aneurysms in this location present a therapeutic challenge for the classic treatment by microsurgical clipping secondary to the anatomic variability, deep location, and presence of numerous vulnerable perforating vessels.4 Since the publication of the International Subarachnoid Aneurysm Trial,5 the treatment paradigm has shifted to favor endovascular treatment of cerebral aneurysms, including those of the ACoA region.6
However, endovascular treatment with coil embolization of ACoA region aneurysms is not always possible and not always definitive. Certain aneurysm types including blister, broad-based, and very small aneurysms are not easily amenable to coiling. In acutely ruptured aneurysms, interventionists may choose a lighter coil pack or dome-occlusive strategy to secure the aneurysm while minimizing the risk of intraprocedural rupture.7 Coiling is also associated with a small but increased risk of aneurysm recurrence and rebleeding compared with microsurgical clipping.8
Flow diversion, initially designed for large and giant internal carotid artery (ICA) aneurysms, represents a new and increasingly accepted treatment modality for intracranial aneurysms of a variety of sizes and locations.9 Innovations including improved catheter technology and simplified device delivery systems have enabled more distal treatments at the level of the circle of Willis and beyond. Flow diversion represents a new and definitive endovascular treatment for recurrent and difficult-to-coil ACoA region aneurysms, of which reports are limited. Here we present a large single-center case series of patients with ACoA region aneurysms who were treated by flow diversion using the Pipeline embolization device (PED).
Methods
A retrospective study was undertaken using an Institutional Review Board approved, prospectively collected database of patients with aneurysms at a tertiary medical center. Individual patient consent was not required or sought as data are collected in a de-identified manner in routine clinical practice at our institution and pose no risk to patients. All patients who underwent PED placement for ACoA or A1–A2 junction aneurysms between October 2012 and May 2016 were identified and included in the study. Pipeline placement was performed as previously described.10 ,11 Patients recovered in the neurocritical care unit and were typically discharged home on post-embolization day 1. Demographic information, clinical history, and outcomes were collected from medical records. Anatomic and technical details were collected from intra-procedure events, angiograms, and operative reports through September 2016. Follow-up cerebral angiography was performed at 6 and 12 months post-embolization. Aneurysm occlusion was graded based on agreement between two experienced neurointerventionists according to the O'Kelly–Marotta scale as no filling, entry remnant, subtotal filling, or total filling.12 Data were recorded as counts, percentages, and means.
Results
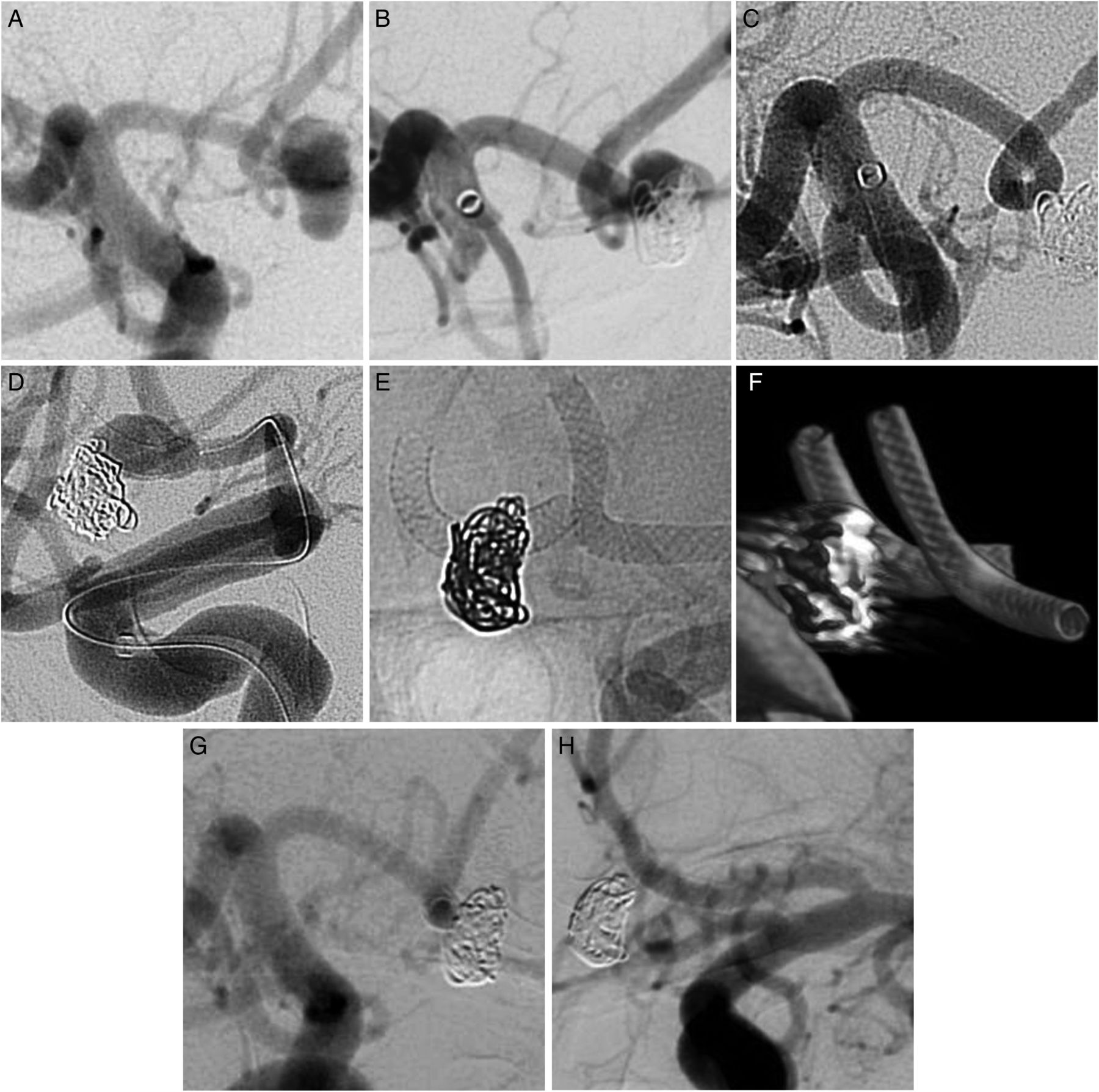
A total of 50 procedures were performed on 41 patients, including seven patients who underwent bilateral anterior cerebral artery (ACA) PED placement (‘H-pipe’) in a staged fashion (figure 1). The average age was 56 years and 46% of the patients were female. The average aneurysm size was 4.5 mm and two large (>10 mm) aneurysms were treated. The vessel of origin was either the ACoA proper (26 aneurysms, 63%) or the A1–A2 junction (15 aneurysms, 37%). Eighteen patients (44%) had prior SAH and 20 had previously been treated either with clipping (6 aneurysms, 15%) or coiling (14 aneurysms, 34%) (table 1).
Demographic characteristics of study patients
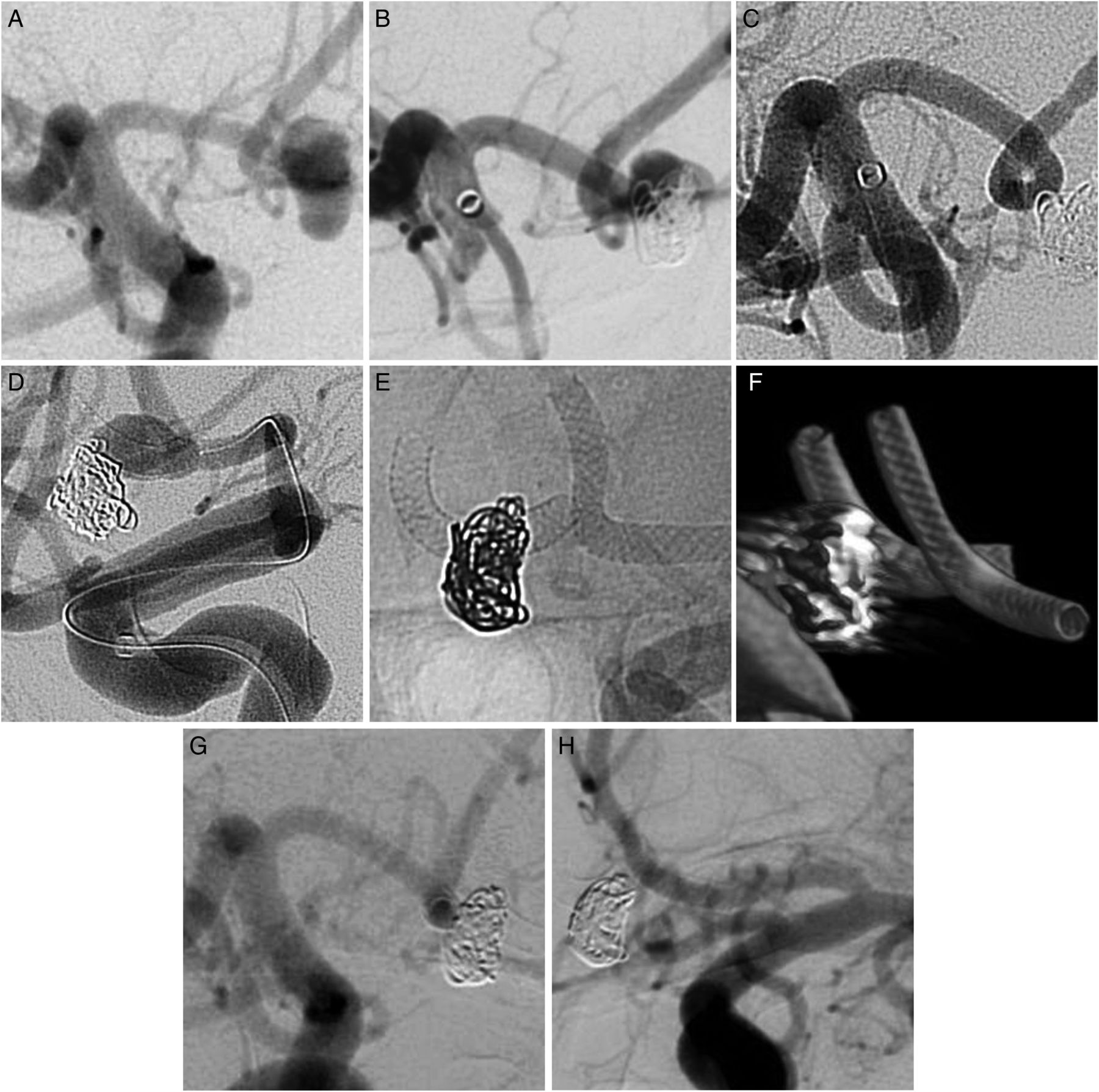
Bilateral Pipeline embolization device (PED) ‘H-pipe’ treatment of neck residual from previously ruptured and coiled 6 mm anterior communicating artery (ACoA) aneurysm in a person in their 40s. (A) Right internal carotid artery (ICA) digital subtraction angiogram (DSA) showing 6 mm ruptured ACoA aneurysm. (B) Six-month follow-up right ICA DSA showing neck recurrence. (C) Right ICA DSA following right A1–A2 PED implantation. (D) Left ICA DSA showing neck filling 6 months following right A1–A2 PED implantation. (E) Left ICA DSA and (F) Dyna CT following bilateral A1–A2 PED implantation. (G) Right ICA DSA and (H) left ICA DSA showing complete occlusion of ACoA aneurysm 6 months following left A1–A2 PED implantation to complete ‘H-pipe’.
Procedural success was achieved in 48 cases (96%). One case with significant proximal vessel tortuosity was aborted because the PED would not open using the Navien and Marskman catheter combination. This case was successfully completed at a later date when attempted with an AXS Catalyst 0.058 inch distal intracranial catheter and Via 0.027 inch microcatheter. The other unsuccessful case was an attempted second stage H-pipe on a previously ruptured 15 mm ACoA aneurysm that was aborted because the device could not be well visualized through the coil mass.
During the procedure, the most common access system used was a triaxial system using a Navien 0.058 inch distal intracranial catheter (40 cases, 80%) and Marksman 0.027 inch microcatheter (40 cases, 80%). Significant cervical ICA tortuosity was encountered in 13 cases (26%). Challenging cavernous ICA anatomy (grade III or IV)13 was present in 26% of cases. The most common final position of the distal intracranial support catheter was the supraclinoid ICA in 21 cases (42%) and the distal cavernous ICA (in proximity to the anterior genu) in 16 cases (32%).
Among the successful cases, the PED was deployed from ipsilateral A1 to contralateral A2 in three cases (6%) and ipsilateral A1–A2 in the remainder (45 cases, 94%). Two devices were used in one case (2%) and one device was used in 47 cases (98%). The average fluoroscopy time and radiation exposure were 36 min and 1994 cGy, respectively. Intra-arterial (IA) verapamil was administered in 16 cases (32%), most commonly for vasospasm prophylaxis prior to positioning a microcatheter in the ACA. Coils were deployed adjunctively in two cases (4%) at the time of PED placement, and balloon angioplasty was performed in three cases (6%) to improve wall apposition of the PED (table 2).
Case characteristics
The average length of stay was 3.0 days and 69% of patients left on post-procedure day 1. There were no deaths. No significant complications were encountered in 43/48 cases (90%) and permanent morbidity occurred in only one patient (2%). Complications encountered included one major stroke (2%) and two patients with intracranial hemorrhage (ICH) (4%). The major stroke occurred in a patient with a previously ruptured and coiled 4 mm right A1–A2 aneurysm who developed altered mental status and right hemiparesis 2 days following PED implantation. Digital subtraction angiography (DSA) demonstrated partial stent thrombosis with pial collaterals from the ipsilateral middle cerebral artery (MCA) to the ACA. Thrombolysis was not performed due to concern for hemorrhagic conversion of ACA territory stroke seen on MRI, and the patient remained with hemiparesis at discharge to rehabilitation. This case has been described previously.14 Both ICHs were in a dependent right frontal territory, one <10 mL and one 40 mL, and both resulted in transient left-sided weakness that resolved prior to patient transition to rehabilitation. Device thrombosis was observed during the procedure in one patient (2%) and resolved with abciximab administration without postoperative deficits. Transient postoperative aphasia was observed in one patient (2%) without imaging correlate (table 3).
Procedural outcomes
Follow-up angiography was available for 34/41 patients (83%) after successful completion of the procedure. This included 26/31 patients (84%) treated with ipsilateral A1–A2 PED, 3/3 (100%) ipsilateral A1 to contralateral A2, and 5/7 (71%) with completed bilateral A1–A2 PED (H-pipe). Across the entire cohort (unilaterally and bilaterally treated patients), 4/7 patients (57%) without postoperative angiography were within 6 months of treatment. Complete aneurysm occlusion was achieved in 25/29 patients (86%) treated with single-stage PED. Subtotal aneurysm filling was present in the remaining four patients (14%). Average follow-up for patients undergoing H-pipe was 7.7 months compared with 10.6 months for the single-stage PED, as the H-pipe procedures have been performed more recently. Following completion of an H-pipe (two-stage procedure), complete aneurysm occlusion was observed in 80% of cases at longest follow-up during the study period (table 4).
Aneurysm occlusion
Discussion
In this series of 41 patients undergoing 50 procedures, flow diversion of ACoA region aneurysms with the PED showed high rates of aneurysm occlusion and low complication rates. Complete occlusion was achieved in 81% of patients at 6 months and 85% of patients at last follow-up DSA (average of 10.4 months). Symptomatic ischemic complications occurred in a single patient (2%) and hemorrhagic complications occurred in two patients (4%). Only one patient (2%) had permanent neurological deficit. This is comparable to or better than large studies of PED use for carotid aneurysms,15–18 despite the smaller vessel size, manipulation of more distal vasculature, and increased density of small perforator arteries. This demonstrates that the PED can be safely employed to treat aneurysms of the ACoA region.
While some have speculated in the literature that placing oversized devices in small distal vessels may reduce wall coverage and the flow diversion effect,7 we observed high occlusion rates with the PED in ACoA region aneurysms, consistent with the general population of patients treated with PED in which complete occlusion was achieved in 70–80% at 6 months15 and approaching 90% after more than 1 year after stopping dual antiplatelet therapy.19 In 4/29 patients (14%) treated with single-stage PED, there was interval remodeling with decreased but subtotal aneurysm filling at last follow-up angiogram. Because these patients were within 12 months of treatment and had not completed their antiplatelet taper, they do not represent treatment failures. If follow-up imaging continues to demonstrate progressive closure of the aneurysm as the antiplatelet medications are tapered, retreatment is not performed. Treatment would be considered a failure if there was persistent residual filling 24 months after treatment with the patient tapered down to low-dose aspirin, and no patient met this criterion.
Previously published reports of PED embolization for ACoA region aneurysms have similarly shown high rates of aneurysm occlusion. Thirteen ACoA region aneurysms were included among 20 ACA aneurysms treated with PED by Dabus and colleagues. Complete occlusion was achieved in 81% of patients with follow-up angiogram at a mean 10 months post-procedure.20 Lin and colleagues demonstrated complete occlusion at 3- or 6-month post-procedural angiography in three ACoA region aneurysms among 28 distal anterior circulation aneurysms treated with PED.21 Post-embolization DSA showed complete occlusion in two of four patients with ACoA region aneurysms treated by Gawlitza and colleagues; the other two had decreased aneurysm diameter while still on clopidogrel and within 6 months of treatment.22
The overall symptomatic ischemic stroke rate of 2% in the present study compares favorably with the general population of patients treated with PED. The prospective Pipeline for Uncoilable or Failed Aneurysms (PUFS) trial included 107 PEDs and had an ischemic stroke rate of 2.8%.15 Similarly, a meta-analysis by Kallmes and colleagues found that even the safest PED for small (<10 mm) anterior circulation aneurysms had an ischemic stroke rate of 2.7%.17
Complication rates associated with flow diversion of ACoA aneurysms were comparable to alternative endovascular treatments and compared favorably with open surgical clipping. In this study, permanent neurological morbidity was 2%. By comparison, a recent meta-analysis of 14 studies including 862 unruptured ACoA aneurysms showed treatment-related morbidity (defined as modified Rankin Scale score of 2–6) of 0.8%, 4.4%, and 7.9% associated with endovascular coiling, microsurgical clipping, and stent-assisted coiling, respectively. While microsurgical clipping of ACoA aneurysms holds an advantage over endovascular coiling in terms of durability, it remains to be seen whether clipping holds a similar advantage over flow diversion. The meta-analysis of unruptured ACoA aneurysms showed angiographic recurrence and retreatment of 0% associated with clipping compared with 7.2% and 4.9%, respectively, associated with coiling.23 In the present study, complete occlusion was seen in 85% of aneurysms at an average last follow-up of 10.4 months post-treatment. As mentioned previously, patients with residual filling had not completed post-procedural antiplatelet tapering. Occlusion rates will increase with time,19 but it cannot be determined whether they will match clipping. The inclusion of previously clipped aneurysms in this study is clear evidence that post-clipping recurrence rates must not be zero.
Part of the reluctance to use the PED in the ACoA region arises from reports of ischemic stroke attributed to occlusion of perforating arteries, including medial lenticulostriates and the recurrent artery of Heubner, covered by flow diverting devices. In an early report, Van Rooij and colleagues placed a telescoping PED to treat a large A1 aneurysm with complex morphology, and the patient developed cognitive impairment and memory dysfunction that was attributed to perforator occlusion from left basal ganglia infarction.24 Other studies have shown that perforator issues that occur are infrequent with more routine treatments and are often transient or silent and discovered only on routine postoperative imaging.20 ,22 ,25
In a retrospective study of 25 patients with ACA or MCA aneurysms treated with PED at multiple centers in Spain, perforator issues appeared to cluster in the four patients with ACoA region aneurysms. In that series, one patient experienced transient weakness on postoperative day 3 from perforator territory ischemia and another patient who had two PEDs placed was found to have asymptomatic anterior caudate hypodensity on routine post-embolization head CT.26 The authors speculated that PED deployment across the acute angulation of the A1–A2 junction may result in increased metal coverage at the inner curvature where perforator density is high and lead to perforator occlusion. In our cohort of 50 procedures, including one case of overlapping PED, no symptomatic perforator infarctions were observed. Small asymptomatic ‘silent’ infarcts are common after endovascular procedures, but the significance is unknown.27 In the present study, routine post-procedure imaging (eg, MRI) was performed only for symptomatic patients with new neurological deficits. The frequency of silent infarcts cannot therefore be estimated.
The reluctance to use the PED for ACoA region aneurysms also arises from concern for covered side branch occlusion. In a retrospective study of 32 patients with anterior circulation bifurcation aneurysms, Saleme and colleagues provided a useful framework for assessing this risk. They separated patients into two groups in which the covered side branch either had direct collaterals (as with most ACoA region aneurysms and A1 aneurysms with a patent ACoA and contralateral A1) or supplied a terminal-type circulation. In the former group, which included eight ACoA region aneurysms, the covered vessel was occluded on follow-up angiography 71% of the time, and none of these patients had symptoms or showed ischemic lesions on MRI 6 months after treatment. By contrast, covered side branches supplying a terminal circulation remained patent in 91% of patients on follow-up angiography and 22% of patients experienced symptoms associated with vessel narrowing or occlusion.28 Others reporting results for ipsilateral PED for ACoA region aneurysms have speculated about the potential hazard of this treatment in the presence of agenesis or hypoplasia of contralateral A1.25
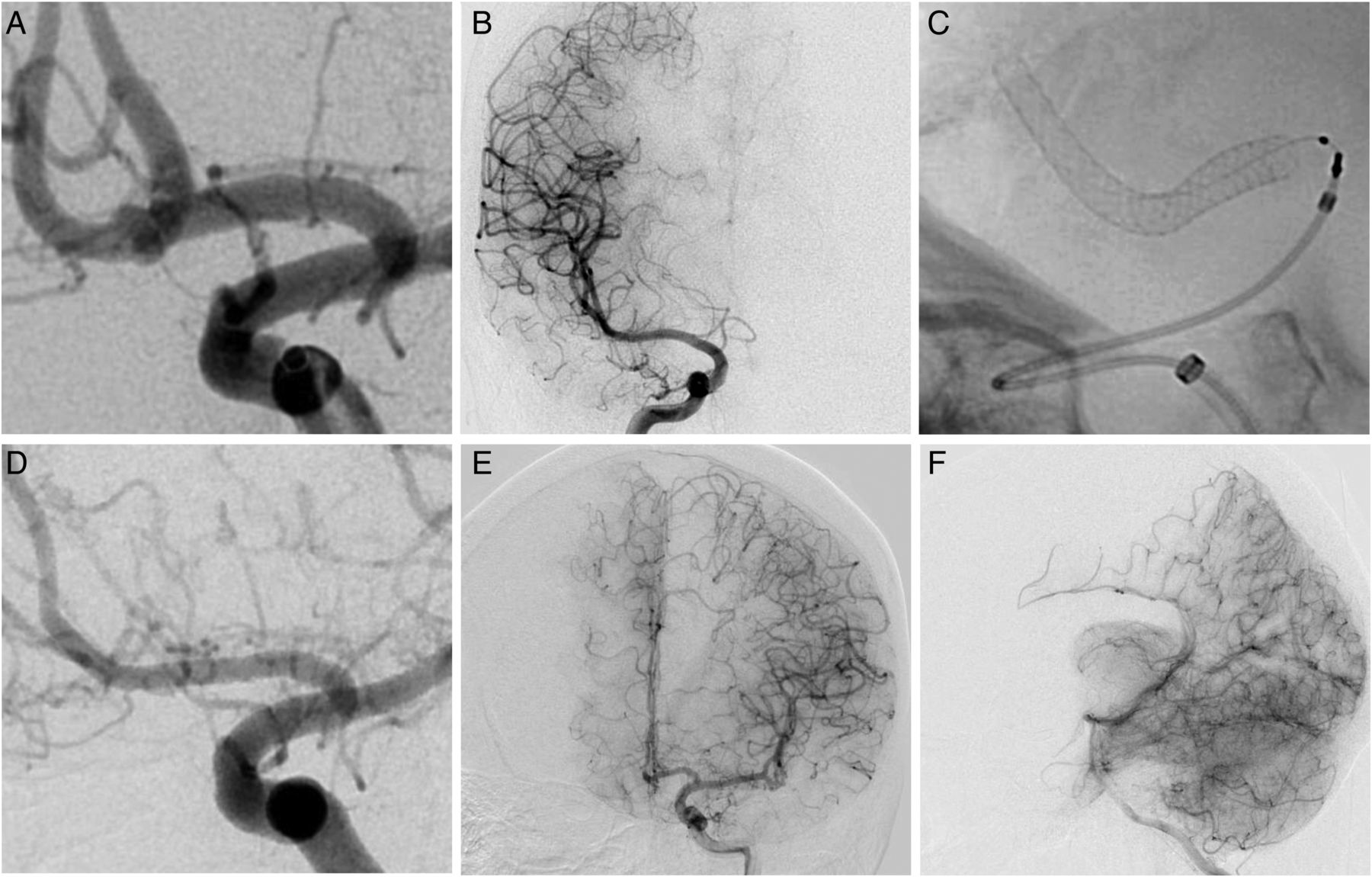
In the current study a hypoplastic A1 was present in seven patients, none of whom experienced transient or sustained ischemic symptoms during a period of collateral recruitment. Among those with follow-up angiography, three patients with eccentric aneurysms treated with an ipsilateral A1–A2 PEDs developed more robust flow through the hypoplastic A1 to supply the covered contralateral ACA territory (figure 2). Three patients with true ACoA region aneurysms were treated with an ipsilateral A1 to contralateral A2 construct covering the ipsilateral A2. In both patients follow-up angiography showed progressive occlusion of the ipsilateral A2 with pial collaterals from the MCA and posterior cerebral artery supplying the dependent ACA territory (figure 3). Covering a side branch that supplies a terminal-type circulation simultaneously reduces blood flow to dependent parenchyma and promotes flow through collateral networks. In our experience, neoendothelialization along the stent to occlude the covered side vessel and growth of collateral networks are two processes that appear to proceed apace according to tissue demands. None of these angiographic changes in blood flow resulted in clinical symptoms.
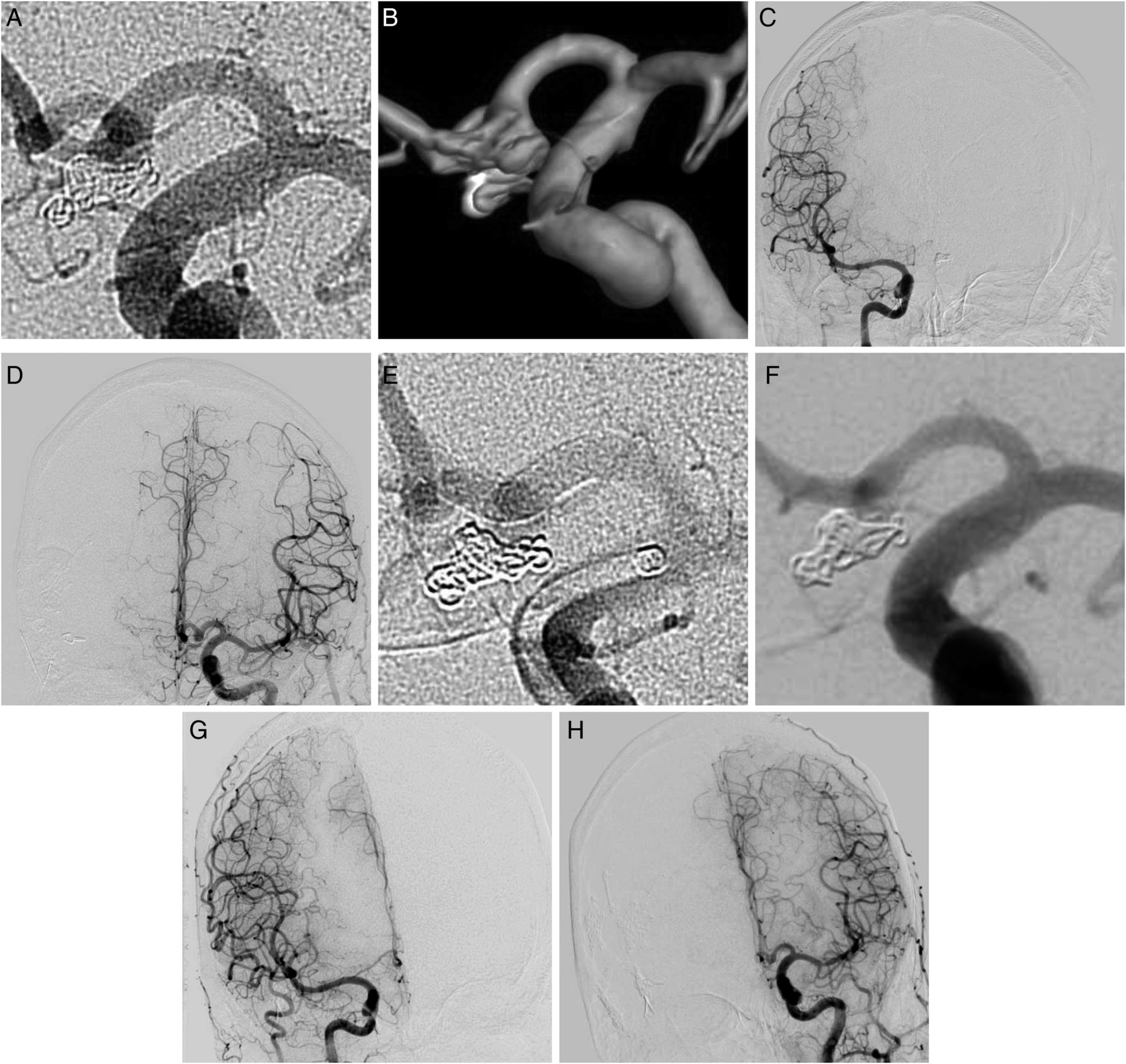
Pipeline embolization device (PED) treatment of a 4 mm neck residual of previously ruptured and coiled anterior communicating artery (ACoA) aneurysm. (A) Left internal carotid artery (ICA) digital subtraction angiogram (DSA) and (B) three-dimensional reconstruction demonstrating aneurysm neck residual. (C) Pre-procedure right ICA DSA showing hypoplastic right A1 and (D) left ICA injection filling the right anterior cerebral artery (ACA) territory. (E) Left ICA DSA following PED implantation from ipsilateral A1–A2. (F) 12-month follow-up DSA with complete aneurysm occlusion. (G) 12-month follow-up right ICA DSA showing enlargement of hypoplastic right A1 and (H) minimal filling of the right ACA territory on left ICA injection.

{kind=link}
{kind=link}
{kind=link}
Pipeline embolization device (PED) treatment of an enlarging fusiform 4 mm anterior communicating artery (ACoA) aneurysm in a person in their 40s. (A) Left internal carotid artery (ICA) digital subtraction angiogram (DSA) showing ACoA aneurysm and filling of bilateral A2. (B) Right ICA DSA showing hypoplastic right A1. (C) Left ICA DSA following left A1 to right A2 PED implantation. (D) 12-month follow-up left ICA DSA showing aneurysm occlusion and occlusion of covered left A1 (E) with pial collaterals from the middle cerebral artery and (F) pial collaterals from the posterior cerebral artery supplying the left anterior cerebral artery territory.
Finally, the reluctance to use the PED in the ACoA region also arises from concern for stent occlusion (acute or delayed). Martin and colleagues hypothesized that thrombosis and in-stent stenosis may be more likely in small distal vessels where a 1–2 mm reduction in arterial caliber is a greater impediment to laminar flow, but observed neither complication in their series of 12 patients at Canadian institutions treated with the PED for aneurysms arising from vessels <3 mm in diameter.29 In our series, one patient developed stent thrombosis intra-procedurally, which resolved completely with abciximab administration. One patient developed a stroke related to stent thrombosis, discovered outside the window for thrombolysis. Three patients (8%) had mild non-flow-limiting in-stent stenosis on follow-up DSA which is comparable to rates of 5–10% in the general PED population.9 ,30 Our institutional protocol is to perform follow-up angiography 6 months after treatment and discontinue clopidogrel at this time, assuming no significant intimal hyperplasia. Aspirin is tapered from 325 mg to 81 mg daily with similar results on angiography 12 months after treatment. Patients with in-stent stenosis were maintained on dual antiplatelet medication for six additional months without complications. Follow-up angiography on patients with in-stent stenosis showed improvement or resolution in all cases.
The results presented here demonstrate flow diversion as a useful tool for treating ACoA region aneurysms but raise questions about when to deploy it. Flow diversion is not appropriate in the acute phase of SAH, given the need to immediately secure the aneurysm and the obstacle dual antiplatelet therapy poses to additional interventions. However, there were 18 patients in this study with a history of SAH from a ruptured ACoA region aneurysm, the majority of whom were initially treated with coiling. At our institution and elsewhere,7 a ‘dome-occlusive’ coiling strategy is sometimes pursued in acute SAH to minimize the risk of intra-procedural rupture or coil prolapse into a parent vessel that may later develop vasospasm. For such aneurysms, flow diversion is appropriate as a planned definitive intervention for neck residual once the vasospasm window has passed and the patient recuperated or in the event of aneurysm recanalization. Retreatment was performed within 6 months of SAH in these cases (14 patients, 78%) whereas late recurrence and retreatment after more than 12 months was less common (4 patients, 22%). As an initial treatment, flow diversion may be an appropriate alternative to coiling for very small, blister, or fusiform aneurysms. Patients with wide-necked ACoA aneurysms are difficult to treat with coiling and are traditionally good candidates for microsurgical clipping. In this study, among the 21 patients with no prior treatment, 18 (85%) had wide-necked aneurysms either with a dome-to-neck ratio <2 or a neck >4 mm. In each case, flow diversion rather than microsurgical clipping was chosen either because of complex medical comorbidities, blister or fusiform morphology, patient refusal of open surgery, or a plan for staged treatments in multiple vascular distributions.
None of the complications in this series was observed in patients who underwent H-pipe embolization, either during the first or second stage. These procedures are staged for two reasons: Firstly, it cannot be absolutely predicted which patients will require bilateral treatments, although aneurysms that fill robustly on injection from both ACA are the most likely candidates, secondly, we do not use the PED in more than one major vascular distribution during a single procedure to reduce the risk of simultaneous bilateral ischemic or hemorrhagic complications in dependent vascular territories. Whenever a patient who has previously been treated with PED undergoes a second procedure we are conscious of the fact that the response to clopidogrel can accumulate over time.31 Patients are assessed clinically for excessive bruising or spontaneous bleeding and P2Y12 values are checked pre-procedurally to assess for hyper-response. More sophisticated single PED deployment techniques, such as barreling the device, may also reduce the need for future H-pipe constructs.
Success in treating ACoA aneurysms with flow diversion relies on a variety of technical considerations. The first consideration is access. As with all endovascular cases, tortuosity of the proximal vasculature from the aortic arch to the intracranial vasculature can increase the complexity of the procedure. For ACoA region aneurysms, the cervical ICA, cavernous ICA,13 ICA–A1 transition, and the A1–2 transition are all sites where tortuosity can exist and influence the procedure. In our experience, judicious use of distal intracranial catheters (Navien and AXS Catalyst 5) and positioning these catheters in true distal locations32 is important for the success of these cases, particularly in situations of severe tortuosity. Robust catheter support enables one-to-one device manipulation, superior push of the PED delivery wire, and improved retracking of the 027 catheter. The second consideration is the device selection and deployment. We use a single PED whenever possible to avoid double covering perforating arteries and avoid the added vessel manipulation during deployment of a second device. Device deployment includes using robust distal access to ‘push’ the device out of the microcatheter. Further loading the device/catheter during deployment through the A1–2 junction helps to improve vessel wall apposition in this area. This not only improves coverage of an aneurysm neck (especially for A1–2 junction aneurysms) but it also prevents malapposition of the device in regions of critical perforators, such as the recurrent artery of Heubner. The small PED used for these procedures (typically devices with a diameter of 2.5 mm) often opens well without significant manipulation. As such, we limit the amount of post-deployment device manipulation (eg, balloon angioplasty), and therefore vessel manipulation, only to those cases where there is clear angiographic evidence of incomplete device apposition. Given that PED treatment for ACoA region aneurysms involves tracking 027 catheters into smaller vessels compared with PED cases in the ICA, we frequently use IA calcium channel blockers to prevent or treat flow-limiting vasospasm. There is little concern for overdilating the vessels beyond limitations in PED diameter (as might be the case with an ICA that measures close to 5 mm) because most PED devices sized 2.5 mm are already oversized compared with the ACA vessel.
The primary limitations of this study include its retrospective non-randomized nature and the relatively short follow-up period compared with other treatment modalities. Although multi-year follow-up is not available at this time, aneurysm occlusion rates >80% were achieved in the short follow-up period that we have. Progressive aneurysm occlusion over time is common after flow diversion, and we expect occlusion rates to increase as more follow-up is available. Furthermore, the follow-up that did occur was likely to capture clinically relevant complications as delayed complications are uncommon.
Conclusions
This series of 50 PED procedures demonstrates that flow diversion with the PED is a safe and effective treatment for aneurysms of the ACoA region. This represents a valid alternative option to microsurgical clipping and endovascular coiling when appropriate.
References
Footnotes
GPC and MTB are joint first authors.
Contributors All authors contributed significantly to conception, data acquisition, and analysis; all drafted and revised manuscript contents; and all approved the final version of the manuscript. GPC and MTB contributed equally to this paper.
Competing interests AC is a consultant and proctor for Medtronic, Styker, and Microvention. GPC is a consultant for Medtronic and Microvention.
Ethics approval Ethics approval was obtained from the Johns Hopkins University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The relevant anonymised patient level data are available on reasonable request from the authors.