Article Text

Abstract
Background Intracranial access techniques in modern neurointerventions have shifted towards more robust access platforms. The long guide sheath is one of the building blocks of triaxial systems used in intracranial embolizations. Here we present our experience with the AXS Infinity LS long sheath in the triaxial platform for the implantation of the Pipeline embolization device (PED).
Methods We retrospectively identified patients who underwent PED Flex treatment with the AXS Infinity LS at a single institution. Procedural data collected included parent artery tortuosity, patient demographics, vasodilator use, aneurysm characteristics, equipment utilized, and catheter-related complications.
Results A total of 95 cases were completed using the AXS Infinity LS for the triaxial platform foundation in PED Flex treatment of cerebral aneurysms. Mean patient age was 56.2±12.2 years (range 21–86). Average aneurysm size was 6.9±6.2 mm (range 1–38). There were 89 anterior circulation cases (94%) and 6 posterior circulation cases (6%). Significant cervical ICA tortuosity was present in 11/89 (12%) and moderate to severe cavernous ICA tortuosity was present in 29/89 (33%). Mean fluoroscopy time was 40.0±19.8 min. In 14/95 cases (15%), vasospasm prophylaxis or treatment with intra-arterial verapamil infusion was performed. Catheter access-related complications included asymptomatic iatrogenic dissection in one case (1%) from the distal intracranial catheter and groin hematoma in one case (1%). No parent vessel wall abnormalities were visualized in the region of the Infinity long sheath on final control angiography in all 95 cases.
Conclusion The AXS Infinity LS is the newest long guide sheath available for modern neurointerventional procedures. We have shown its utility in augmenting the triaxial access platform in PED Flex cases by providing enhanced distal tip trackability with added support in the aortic arch and proximal great vessels.
- aneurysm
- endovascular
- flow diversion
- guide catheter
- distal access
- pipeline embolization device
Statistics from Altmetric.com
Introduction
The access techniques of modern neurointerventional procedures have shifted from a classic biaxial set-up to sturdier triaxial systems. This transition towards robust catheter access platforms is the result of advances in modern neuroendovascular devices requiring larger size delivery systems such as the Pipeline Embolization Device1 (PED; Medtronic Neurovascular, Irvine, California, USA), the Woven Endobridge Device2 (WEB; MicroVention Terumo, Tustin, California, USA) and the Surpass flow diverter3 (Stryker Neurovascular, Freemont, California, USA). Advances in ischemic stroke care with stentrievers and aspiration techniques have also driven neurointerventional procedures to the triaxial platform.4
Much has been published about the new class of hybrid distal intracranial catheters (DICs), such as the Navien DIC (Medtronic Neurovascular) and AXS Catalyst 5 (Cat 5; Stryker Neurovascular), that are integral to the triaxial systems in aneurysm flow diversion treatments.5–7 These catheters have flexible rounded soft tips allowing for trackability into various intracranial locations.5–10 The fundamental building block of the triaxial platform in these cases, however, is the long guide sheath, such as the Flexor Shuttle Sheath (Cook Medical, Bloomington, Indiana, USA) and the Neuron MAX (Penumbra, Alameda, California, USA). Published literature on the use of long guide sheaths is scant and only presented within the context of DIC experiences.1 3 11–13 The AXS Infinity LS (Infinity; Stryker Neurovascular) is the newest addition to the long guide sheath family specific for neurointerventions. The Infinity has a supportive multi-durometer shaft adapted from the catheter technology improvements developed with DICs (eg, rounded tip edges, multi-durometer). We present in this report our experiences using the Infinity in cerebral aneurysm treatments with PED flow diversion.
Methods
Patient selection
We retrospectively reviewed a prospective single-center aneurysm database to identify all patients with cerebral aneurysms consecutively treated with Pipeline embolization using the Infinity long guide sheath from July 2016 (first availability of Infinity at the institution) to January 2017.
Data collection
Data on patient demographics, aneurysm characteristics, proximal tortuosity, vasodilator use, procedural equipment, technical details, and peri-procedural complications related to the catheter access were collected. Factors assessed for proximal tortuosity included cervical ICA tortuosity (defined as a 90° turn, hairpin turn, or corkscrew loop) and cavernous ICA grade.14 Data are presented as counts.
Endovascular procedure
Details regarding the PED procedure have been previously described.1 13 14 Patients were preoperatively treated with aspirin 325 mg and clopidogrel 75 mg daily for at least 5 days prior to the planned treatment. P2Y12 assay for platelet inhibition testing was not routinely performed.15 16 Systemic anticoagulation with heparin was given during the embolization. Through an 8F femoral short sheath, a triaxial system was used for all procedures consisting of a long guide sheath, a DIC, and a 0.027 inch microcatheter. An Infinity was the long guide sheath utilized successfully in each case. The DICs used included Navien (Medtronic Neurovascular), Catalyst 5 (Stryker Neurovascular), Sofia (MicroVention Terumo) and InNeuroCo Intermediate Catheter (InNeuroCo, Sunrise, Florida, USA). The 0.027 inch PED delivery microcatheter used included the Marksman microcatheter (Medtronic Neurovascular), Phenom 27 microcatheter (Medtronic Neurovascular), and VIA27 microcatheter (MicroVention Terumo).
Results
A total of 95 PED treatments were identified where the AXS Infinity LS served as the foundation of the triaxial system for PED Flex embolizations. Tables 1 and 2 summarize the details of all cases.
Case summaries
Procedural details
Patient and aneurysm characteristics
Eighteen men and 77 women were treated. Mean patient age was 56.2±12.2 years (range 21–86). Average aneurysm size was 6.9±6.2 mm (range 1–38). Seventy-four of the 95 aneurysms (78%) had no prior treatment while 3/95 (3%) were previously clipped, 12/95 (13%) were previously coiled, and 6/95 (6%) were previously treated with a flow diverter. Eighty-nine of the PED cases (94%) were in the anterior circulation and six (6%) were in the posterior circulation. The most common PED implantation along the internal carotid artery (ICA) was the paraophthalmic/clinoidal segment (36/69, 52%), followed by the supraclinoid/posterior communicating (19/69, 27%), cavernous segment (10/69, 14%), ICA termination (2/69, 3%), and cervicopetrous (2/69, 3%) segments. In addition to ICA aneurysms, 12 (13%) anterior cerebral artery (ACA) aneurysms were treated and eight (8%) middle cerebral artery (MCA) aneurysms were treated. Of the six posterior circulation aneurysms treated, the locations included V4 (n=1), PICA (n=1), mid-basilar (n=1), basilar apex (n=2), and P1 segment (n=1).
Proximal vascular access characteristics
Figure 1 illustrates a case example of the arch support provided by the Infinity long sheath in widened type III aortic arches. Significant cervical ICA tortuosity, defined as a 90° turn, hairpin turn or corkscrew loop, was encountered in 11 of the 89 (12%) anterior circulation cases. Figures 2 and 3 illustrate the robust support provided by the Infinity in cases with proximal ICA tortuosity. Minimal cavernous ICA tortuosity (type IA and IB) was observed in 60/89 (67%), while moderate to severe cavernous ICA tortuosity (type II–IV) was present in 29/89 cases (33%). The most common positions of the distal intracranial catheter support were proximal cavernous (n=39, 41%), distal cavernous (n=31, 33%), supraclinoid (n=14, 15%).

AXS Infinity LS straightens widened type III aortic arch in PED Flex treatment of recurrent coiled left posterior communicating artery (PCom) aneurysm. (A) Left common carotid roadmap, anteroposterior view, at the level of the aortic arch shows navigation of Infinity straightens type III arch. Black arrow shows Infinity distal tip, double white arrowhead indicates straightened section of aortic arch from Infinity support. (B) Left common carotid roadmap, lateral view, demonstrates stability of Infinity position as the Catalyst 5 navigates through proximal internal carotid artery (ICA) tortuosity. Black arrow shows Infinity distal tip, black arrowhead shows Catalyst 5 distal tip. (C) Left internal carotid digital subtraction angiography (DSA), lateral view, demonstrating the recurrent coiled left PCom aneurysm. (D) Final control DSA, lateral view, showing implanted PED Flex device from proximal left M1 into supraclinoid ICA.

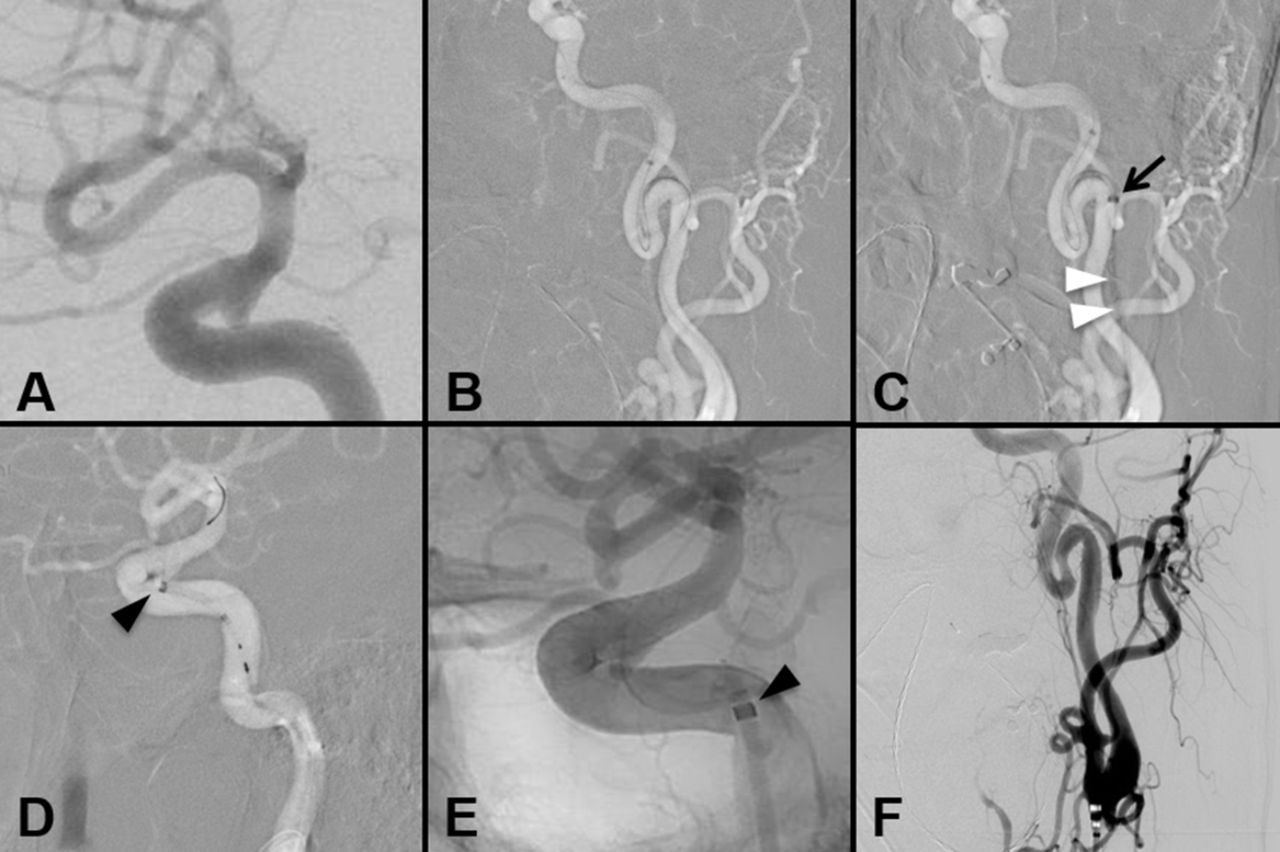
AXS Infinity LS straightens tortuous proximal internal carotid artery (ICA) in PED Flex treatment of a giant 33 mm left ICA cavernous segment aneurysm. (A) Left internal carotid digital subtraction angiography (DSA), lateral view, demonstrating the giant left ICA cavernous segment aneurysm. (B) Left common carotid roadmap, anteroposterior view, demonstrating severe proximal ICA tortuosity. (C) Left common carotid roadmap, lateral view, illustrates straightening of cervical ICA tortuosity by Infinity. Black arrow indicates Infinity distal tip, double white arrowhead indicates the straightened segment of ICA from Infinity support. (D) Left common carotid roadmap, lateral view, demonstrates stability of Infinity position as the Catalyst 5 navigates across the aneurysm. Black arrow indicates Infinity distal tip, black arrowhead indicates Catalyst 5 distal tip. (E) The Pipeline device is visualized across the neck of the aneurysm. (F) Post-procedural control DSA demonstrates the coil mass, Pipeline construct, and widely patent parent ICA and distal vessels without dissection, spasm, or injury.
{kind=link}
{kind=link}
{kind=link}
AXS Infinity LS provides robust support in severe proximal internal carotid artery (ICA) tortuosity for PED Flex treatment of left dissecting ICA ophthalmic segment aneurysm. (A) Left internal carotid digital subtraction angiography (DSA), lateral view, demonstrates the left, broad-based dissecting ICA ophthalmic segment aneurysm. (B) Left common carotid roadmap, anteroposterior view, demonstrating proximal access with severe ICA tortuosity. (C) Left common carotid roadmap, anteroposterior view, straightening of cervical ICA from Infinity navigation. Black arrow shows Infinity distal tip, double white arrowhead shows straightened segment of ICA from Infinity support. (D) Left common carotid roadmap, lateral view, demonstrates stability of Infinity position as the Catalyst 5 navigates across the aneurysm. Black arrowhead indicates Catalyst 5 distal tip. (E) Left internal carotid native fluoroscopy, lateral view, demonstrates deployed PED Flex device across the aneurysm. Black arrowhead indicates Catalyst 5 distal tip. (F) Final control DSA, anteroposterior view, demonstrates a widely patent left proximal ICA post PED implantation without vessel injury, spasm, or dissection.
Procedural characteristics
All 95 consecutive cases were completed with successful PED implantation. Mean fluoroscopy time was 40.0±19.8 min and mean radiation exposure was 2260±1123 mGy. In 14/95 cases (15%), vasospasm prophylaxis or treatment with intra-arterial verapamil infusion was administered via the Infinity and/or DIC. The Catalyst 5 (72/95, 76%) and VIA27 (91/95, 96%) were the most common DIC and PED delivery microcatheters used, respectively. Access-related complications included iatrogenic dissection from DIC positioning (1/95, 1%) and groin hematoma (1/95, 1%). On final control angiography, no parent vessel wall abnormalities were visualized in the region of the Infinity long sheath.
Discussion
In this report we outline our experience with the AXS Infinity LS long sheath as the foundation of the triaxial system for 95 consecutive cases of PED Flex embolizations in cerebral aneurysm treatments. All 95 cases successfully achieved aneurysm embolization with PED implantation via an Infinity long guide sheath. Significant cervical ICA tortuosity was present in 12% of the cases and moderate to severe cavernous ICA tortuosity (type II–IV) was encountered in 33% of cases. In only 15% of cases was intra-arterial verapamil infusion for vasospasm prophylaxis or treatment administered through the Infinity and/or DIC. Of the 95 cases, only two catheter-related complications occurred: one iatrogenic dissection from DIC positioning and one groin hematoma.
Compared with traditional biaxial approaches, the triaxial system offers a more stable platform for one-to-one microcatheter movement in intracranial locations, which in turn provides enhanced microcatheter feedback to improve procedural safety. The ease and safety of establishing triaxial systems have been demonstrated in the literature.7–10 13 This paradigm shift in neurointerventions over the past 5 years to the routine practice of robust catheter access systems precipitated from the flow diversion era where the delivery of these devices required larger (0.027 inch inner diameter) delivery microcatheters.17 The resulting evolution in catheter technology ushered in new access support catheters, the DICs, which incorporate a hybrid design of soft nitinol-wound flexible mid-sections with hyperflexible distal tips for enhanced trackability through the intracranial circulation.5–7 The limitation of these DICs is their lack of proximal body shaft support.5 As such, the DICs are best used in combination with a triaxial platform where a long guide sheath, such as the Flexor Shuttle Sheath or a Neuron MAX, can provide the necessary proximal stability across the aortic arch and proximal carotid artery.
One of the original long guide sheaths, the Flexor Shuttle Sheath, was initially designed as a ‘two-in-one’ device for carotid artery stenting, marrying the proximal shaft support of a guide catheter with a longer soft-tipped sheath. Compared with classic guide catheters, the Flexor Shuttle Sheath has superior kink resistance from coil reinforcement of the shaft. The Shuttle Sheath can be navigated over the arch with a distal tapered inner dilator over a glidewire, or with a coaxial Slip-Cath selective catheter specifically designed for the Shuttle Sheath. Unlike conventional guide catheters where the labeled size refers to the outer diameter, the labeled size of the long guide sheath refers to its inner diameter.
As advances in catheter engineering with the DICs moved the access support system further into the intracranial circulation, concurrent developments have been made with the long guide sheaths, first with the Neuron MAX and more recently with the AXS Infinity LS. Table 3 summarizes the specifications of the Shuttle Sheath, Neuron MAX, and the Infinity sheaths. All three long guide sheaths have PTFE-lined lumens, hydrophilic coating, and radiopaque marker bands at the distal end. The hydrophilic coating enhances lubricity of the long guide sheaths for facile trackability throughout its length. Compared with the traditional short sheaths, the longer length of these guide sheaths provides a more stable pathway for navigation of DICs intracranially to the target pathology. Compared with the Shuttle Sheath, the Neuron MAX incorporated the braiding technology of intracranial catheters, offering kink resistance for the length of the long guide sheath and enhanced torque capabilities. The braiding technology also provides increased trackability and softness of the Neuron MAX’s distal most segment, but at the cost of overall support. In our experience the mid-shaft support of the Neuron MAX around the aortic arch is inferior to the Shuttle Sheath. This limitation is known to be amplified in older patients with widened tortuous arches.
6 Fr Long guide sheaths
The AXS Infinity LS is the newest addition to the long guide sheath armamentarium of the neurointerventionalist. Similar to the Neuron MAX, the Infinity catheter shaft is reinforced with a stainless steel braid. Built into the Infinity are the newest advancements in catheter design—namely, a rounded distal tip shape and multiple transition zones that provide variable stiffness for targeted shaft support along the length of the Infinity. This design augments distal tip softness and trackability, while enhancing mid-shaft support for stability around the aortic arch and the great vessels proximally. Compared with the Neuron Max, the multi-durometer variable stiffness design of the Infinity was optimized to reinforce the support along the segment that corresponds to the aortic arch and the proximal segments of the great vessels, where anatomical challenges can often be encountered. The superior arch support provided by the Infinity in a PED Flex case with a widened type III aortic arch is illustrated in figure 1. Online supplementary video 1 and video 2 demonstrate the utility of the Infinity as a supportive tool around the aortic arch to reform a 6 Fr Select Simmons 2 catheter in the left subclavian artery. Figures 1–3 highlight the superior performance of the Infinity LS over the Shuttle Sheath and Neuron MAX in providing robust support in navigating severely tortuous proximal ICAs (figures 2 and 3) or aortic arches (figure 1), while maintaining distal end trackability. As such, for ultra-trackable DICs that rely on the proximal stability of a long guide sheath for distal intracranial positioning, the Infinity would be the preferred base catheter or long sheath.
In our experience, the Infinity can be used safely without evidence of vessel injury related to positioning of its distal tip. This is attributable to its rounded distal tip shape. This is in stark comparison to the squared-off tip of both the Neuron MAX and the Shuttle catheters, and the traditional tapered tip configuration of femoral sheaths that were designed to avoid a ledge at the sheath/dilator interface. The rounded tip configuration of the Infinity provides the optimal tip design for atraumatic navigation through the great vessels and is an added advantage to the triaxial approach of modern access systems. Intra-arterial verapamil infusion for vasospasm prophylaxis or treatment was administered through the Infinity and/or DIC in only 15% of cases. This demonstrates the true atraumaticity of the tip of the Infinity LS long guide sheath.
The technical considerations for using a long guide sheath include both the manner of insertion and distal navigation. The long guide sheaths are pre-packaged with inner vessel dilators with a distal taper to allow for direct access into the body over a guidewire, without the need for a short introducer sheath. From our initial PED experience and triaxial systems, our preferred femoral access technique is to first insert a standard short 8 Fr sheath (10 cm). Our rationale is that direct insertion of the long guide sheaths may increase the risk of access site infections because of more direct skin contact over the length of the long guide sheaths when advancing into position (commonly used length for anterior circulation is 90 cm). Additionally, positioning of the long guide sheath across the arch often requires back and forth movements, which can also increase the risk of access site infections from the in and out movement of the long guide sheath at the groin. Aside from minimizing infection concerns, inserting the long guide sheath through a standard short sheath allows for direct control of the long guide sheath without hindrances from surrounding skin and soft tissue at the groin. In terms of navigating the long guide sheath, the technical nuance is whether to use an inner select catheter or an exchange technique. Our preferred method of navigation is to use a 6 Fr select catheter within the 6 Fr long guide sheath. This technique provides a seamless, no step-off transition between the long guide sheath distal tip and the select catheter, enabling primary selective navigation into the desired vessel (proximal internal carotid artery or V1/2 vertebral) in an atraumatic manner compared with an over-the-wire exchange technique. For either the Neuron MAX or Infinity, the 6 Fr Select Catheter (Penumbra) is the only select catheter available in the marketplace, in 125 cm length with four different tip shapes.
Conclusion
Robust intracranial access platforms with triaxial systems that consist of a long guide sheath and distal intracranial catheter are becoming essential for the safe and effective delivery of modern neuroendovascular devices. The AXS Infinity LS is the newest addition to the family of long guide sheaths. The Infinity incorporates advanced designs in catheter technology of a rounded distal tip and multi-durometer variable stiffness for enhanced support around the aortic arch and great vessels proximally. We have demonstrated the functionality of the Infinity as a tool to mitigate proximal tortuosity. The Infinity augments the triaxial access platform by providing needed support without sacrificing distal tip trackability.
References
Footnotes
Contributors LML drafted the manuscript and critically revised the manuscript for important intellectual content. NBB, JKC, MTB and BJ assisted with the data collection and analysis. GPC performed treatment procedures and assisted in critically revising the manuscript. JH and RJT crucially reviewed the important intellectual content of the manuscript. ALC performed treatment procedures and critically revised the important intellectual content. All authors read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ALC is a proctor for the Woven Endobridge (WEB) device (Sequent Medical, Aliso Viejo, California, USA), a proctor for the Surpass device (Stryker Neurovascular, Fremont, California, USA) and a consultant for Stryker Neurovascular, a proctor for the Pipeline Embolization Device (Medtronic Neurovascular, Irvine, California, USA) and a consultant for Medtronic, and a proctor for the FRED device (MicroVention, Tustin, California, USA) and consultant for MicroVention. GPC is a consultant for Medtronic, MicroVention and participates in clinical trials for Medtronic and Stryker. LML is a proctor for the Pipeline Embolization Device (Medtronic Neurovascular), a consultant for MicroVention and participates in clinical trial for Stryker. The other authors have no conflict of interest. No author received financial support in conjunction with the generation of this submission.
Ethics approval Johns Hopkins Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from this study.