Article Text

Abstract
Filum terminale arteriovenous fistulae are a rare type of arteriovenous shunt generally characterized by a single direct communication between the artery of the filum terminale and a single draining vein. These intradural arteriovenous shunts are three times more common in men than women (mean age 55 years). Symptoms are related to venous congestion, vascular hypertension, and a putative chronic steal phenomenon which result in spinal cord ischemia and myelopathy. Interestingly, hemorrhage has never been reported as a mode of presentation. MRI demonstrates increased flow voids and T2 changes involving the conus and the lower spinal cord, and these findings are not dissimilar from those seen with the more common type 1 spinal dural arteriovenous fistulae. Thus conventional spinal angiography is necessary for a definitive diagnosis and to localize exactly the site of the fistula. Both surgical interruption of the fistula and endovascular embolization are safe and effective therapeutic modalities. However, because of the very small caliber of the feeding artery, endovascular therapy is often not feasible; and thus, surgery remains the method more commonly utilized for their treatment. Definitive treatment consists of obliteration of the direct arteriovenous shunt. In this review, we describe the anatomy, pathophysiology, clinical presentation, imaging, and treatment options of these less common intradural arteriovenous shunts.
- spinal arteriovenous fistula
- intradural fistula
- filum terminale
- cauda equine vascular malformation
- filum terminale arteriovenous fistula
Statistics from Altmetric.com
- spinal arteriovenous fistula
- intradural fistula
- filum terminale
- cauda equine vascular malformation
- filum terminale arteriovenous fistula
Introduction
Filum terminale arteriovenous fistulae (FTAVF) are a rare type of spinal arteriovenous shunt generally characterized by a single direct communication between the anterior spinal artery (ASA) and its distal prolongation, which is the artery of the filum terminale1–4 and a draining vein (figure 1). These lesions cause spinal cord venous congestion, vascular hypertension, and a putative chronic steal phenomenon, which results in spinal cord ischemia and myelopathy. In this review, we describe the anatomy, pathophysiology, clinical presentation, imaging, and treatment options for this rare type of spinal arteriovenous shunt.
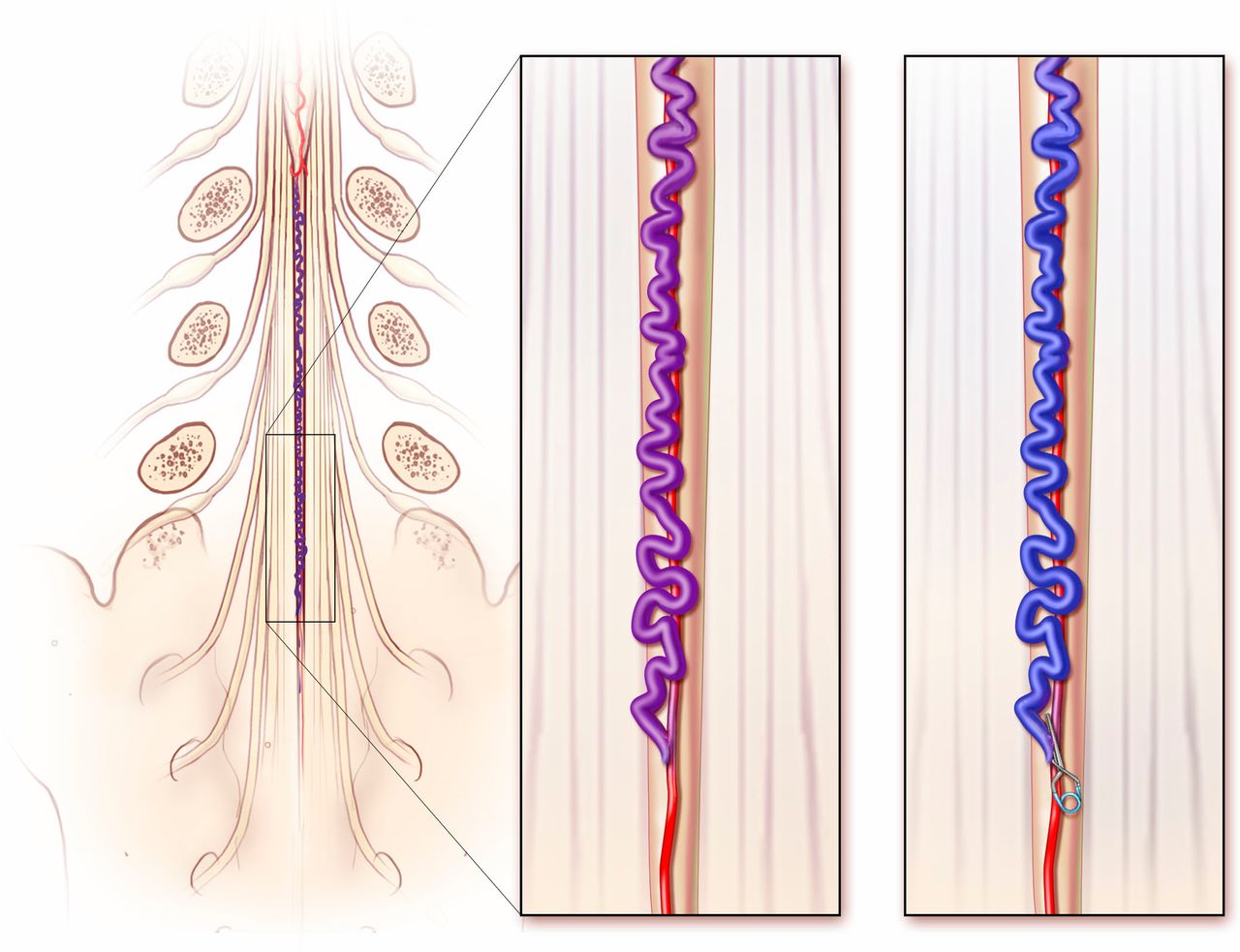
Schematic representation of the nerve roots of the cauda and the filum terminale (left). Enlarged view (center) shows the direct connection between the artery of the filum and a dilated arterialized vein. Definitive surgical treatment consists of clip ligation (right). Endovascular treatment consists of closure of the direct connection along with the proximal portion of the draining vein.
Anatomy
The filum terminale is an end structure of the spinal cord with an upper intradural component (filum terminale internum) and a lower extradural component (filum terminale externum). The filum terminale internum is a 15 cm long, thin connective tissue filament that mostly consists of bundles of collagen fibers, some neurogenic tissue, and is covered by pia mater. It connects the caudal apex of the conus medullaris at the L1–L2 level to the end of the dural tube at the second sacral level.5 The arterial vascularization of the filum terminale consists of one single longitudinal axis, the ‘artery of the filum terminale’, which is the caudal extension of the anterior spinal artery and travels in front of the filum progressively decreasing in diameter, adapting to the size of the filum terminale.6 This artery supplies the filum and coccygeal nerve roots through tiny branch arteries.7 It is argued that since there are no radicular nerves originating from the filum, no other artery can supply it.6 However, reports by Djindjian and others suggest that branch arteries from the lateral sacral artery (LSA) and the middle sacral artery can, in fact, supply the filum6 8–13 and are often involved when a fistula is present. The LSA supplies the filum terminale externum (also known as the coccygeal ligament) and is thus continuous with the filum terminale proper and its anterior spinal artery supply.14 Djindjian et al reported the presence of small branch arteries of the LSA and middle sacral artery supplying the coccygeal nerves which adhere to the filum, also lending support to the notion that the LSA can supply the filum.15
The vein of the filum terminale is a single, uniform caliber, venous structure that runs posteriorly along the filum and then turns at the tip of the filum to course superiorly towards the conus basket.16 This venous axis is capable of working in two directions: descending towards the sacral venous plexus or ascending towards the medullary veins.11
Pathogenesis and pathophysiology
The pathogenesis of FTAVF still remains unclear. Some authors speculate that intradural arteriovenous malformations, such as FTAVF, are congenital.17–19 Others believe that FTAVF may be of acquired origin due to the fact that most patients present in the latter half of adulthood.20 21 Lending support to the notion that some of these lesions are congenital in nature are cases in which FTAVF were associated with neural tube defects, including diastematomyelia, tethered cord, syringomyelia and hypoplastic sacrum, and spina bifida suggesting a possible association between these lesions and neural tube defects .2 6 Ultimately there is no direct evidence supporting either an acquired or congenital etiology for these lesions. Overall, the general consensus in the literature seems to be that these fistulae are acquired in nature and are created by some angiogenic phenomena.
It is widely agreed, that in the presence of FTAVF, there is increased venous pressure secondary to the increased blood flow through the fistulous point. The increased venous pressure is transmitted to the conus and the spinal cord, resulting in a congestive myelopathy. Moreover, the low pressure shunt may encourage flow through the arteriovenous fistulae (AVF) with consequent arterial steal and spinal cord ischemia/dysfunction. Although venous hypertension can result in venous varices (figure 2), hemorrhage from FTAVF has never been reported.
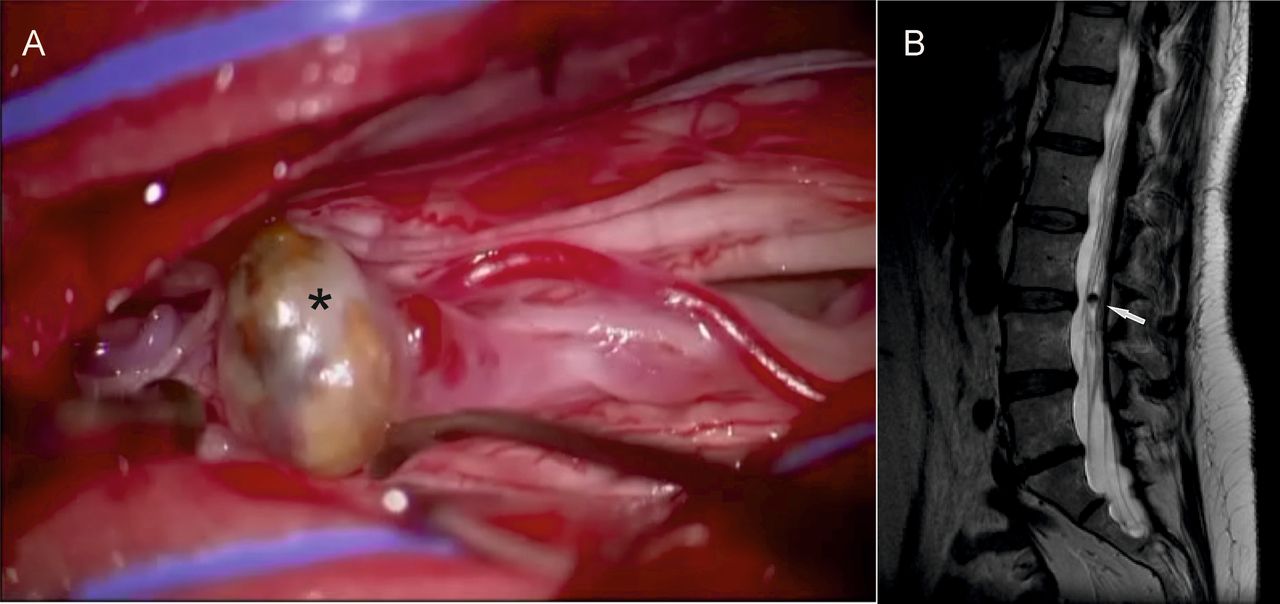
This middle-aged patient came for an evaluation in 2016 with a history of intermittent bilateral leg weakness, progressive left leg weakness, and loss of sensation. The patient had been noticed elsewhere to have serpiginous flow voids in the lower spine since 2008, but two catheter spinal angiograms performed elsewhere failed to show a vascular malformation. Intraoperative exploration revealed a thrombosed calcified venous varix (A, asterisk) corresponding to the round structure seen on MRI (B, arrow). The actual fistula (not shown) was at lower level and was successfully interrupted by clip ligation.
Classification
Initially described by Djindjan in 1977, FTAVF were classified among the spinal arteriovenous malformations or perimedullary spinal AVF.22 Historically, many have advocated using a similar classification scheme to that of perimedullary AVF,23 relying on location (ventral vs dorsal), number of feeders, size, and dilatation of draining veins.4 24 The most common classification scheme is that of Kim and Spetzler. Type A fistulae are intradural ventral AVF, which are small and have a single feeder. Type B fistulae are intermediate sized and have a major feeder from the ASA and minor feeders at the level of the fistula. Type C fistulae are giant, multi-pediculate with massively dilated venous channels with an extraordinary high blood flow.4 Because of the different morphology (usually single hole direct arteriovenous communication) and the unique location along the filum terminale, we advocate considering this specific, although rare, entity as a separate form of intradural arteriovenous shunt.
Epidemiology and clinical manifestations
FTAVF are one of the least common types of spinal vascular malformations. In our review of the literature, we found 39 cases of FTAVF from 1977 to 2017 (table 1). Mourier et al identified only two cases in a 20 year series of spinal AVF25 while Rodesch et al found that these lesions represented just 3.1% of all intradural AVF.26 Indeed, FTAVF account for <5% of spinal intradural arteriovenous malformations.27 While perimedullary AVF classification schemes are often used in the characterization of these lesions, these lesions are distinct from perimedullary AVF, which usually occur in younger patients and may contain a giant draining vein.1 In contrast, FTAVF commonly present in older patients (~55 years) and are three times more common in men.
Summary of cases reported in the literature
As in other spinal vascular malformations, the myelopathy seen in FTAVF patients is secondary to spinal venous congestion. Thus the clinical presentation is often identical to that of patients with SDAVF, with the most common presentation of FTAVF being a slowly progressive myelopathy. Interestingly, hemorrhage has never been reported. Due to their non-specific clinical manifestations, FTAVF are often misdiagnosed as polyradiculopathy and polyneuropathy or as the result of spine degenerative disease (~20% of cases).17 Motor weakness is the most common complaint reported in 80% of cases, followed by sensory disturbances in 77%, back pain in 72%, bladder and bowel disturbances in 67%, and sexual dysfunction in 10%. The most common location of fistulous point is L3–L5 (38% of cases), with sacral location in 20% of cases.
Histopathology
There have only been a few reported histopathologic analyses of FTAVF. These cases confirm that, in general, there is a single arteriovenous connection and no intervening nidus associated with these lesions.5 Microscopic examination of the fistulous point demonstrates a fragmented internal elastic lamina of the markedly dilated vein, with muscular layer abnormalities, which is directly attached to a thinned arterial wall containing rudimentary and fragmented elastic lamina with fibrofatty changes.16 20 At the fistulous point, collagen fibers gradually increase in the wall of the artery; there is arterialization of the proximal draining vein.9
Imaging
MRI is the first recommended diagnostic step in the evaluation of any potential spinal vascular pathology. Because of the similar pathophysiology of FTAVF to other direct spinal vascular shunts, the typical MRI findings associated with these lesions are very similar to those of perimedullary AVF, dural AVF, and epidural AVF.1 Prominent vascular flow voids (46%) and vascular enhancement (67%) are extremely common (figure 3A, B). On spine MRI, they are typically associated with high T2 signal involving the conus and extending up the spinal cord (70%) (figure 3C).
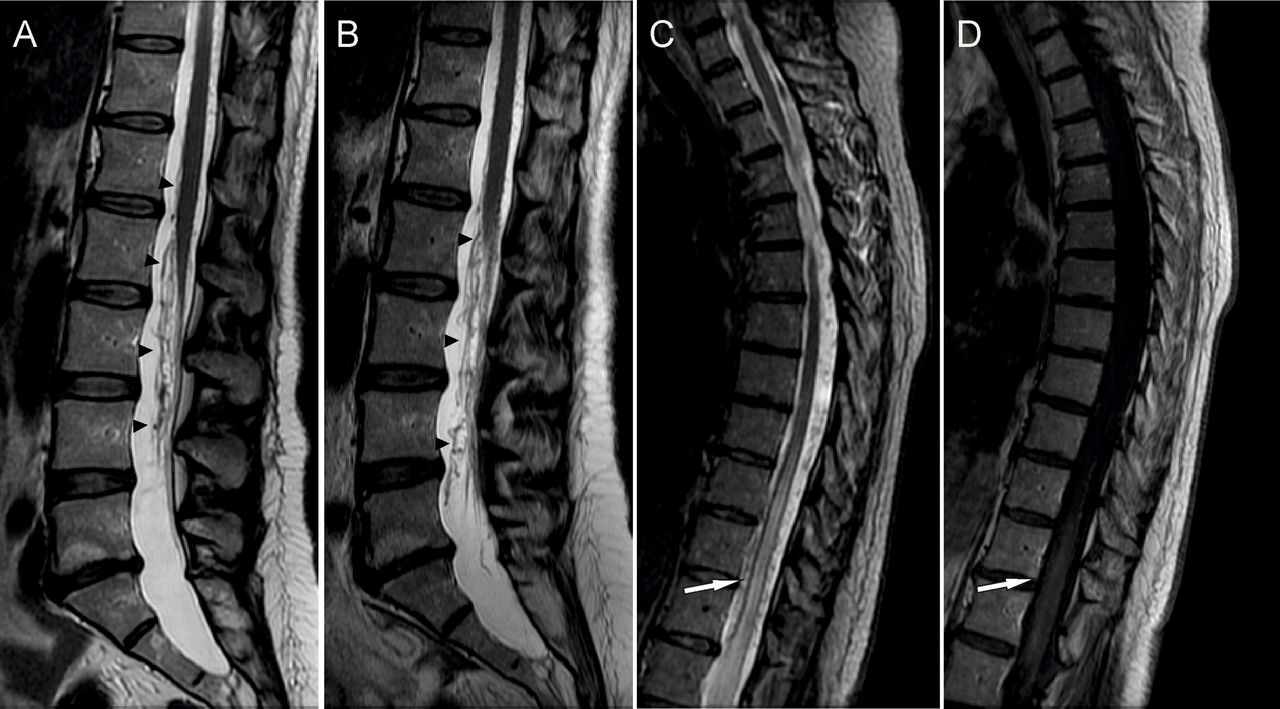
Same patient as in figure 2. (A) T2 weighted sagittal thoracolumbar MRI (2008) shows flow voids at the level of the conus medullaris with tortuous venous drainage ascending along the spinal cord (arrowheads). (B) Two years later, T2 weighted sagittal thoracolumbar MRI shows increased flow voids over the spinal cord with more evident venous tortuosity (arrowheads). (C) T2 weighted thoracolumbar MRI shows hyperintense signal extending from the conus medullaris to a more cephalic region of the spinal cord (arrow). (D) Contrast-enhanced T1 weighted thoracolumbar MRI in 2016 shows spinal cord enhancement (arrow).
While spinal MR angiography (MRA) can occasionally be helpful in differentiating these lesions from dural AVF and epidural DAVF, its main role is to confirm the presence of a fistula and help narrow down potential arterial territories in preparation for definitive catheter angiography.1 In general, DSA is a must in order to accurately characterize the angioarchitecture of the lesion, identify all arterial feeders, and examine for the presence of any additional associated spinal vascular malformations.28 On spinal angiography, FTAVF are typically characterized by a focal, single hole fistula located well below the conus in the lower lumbar spine (figure 4). The fistulous point is usually defined by the transition from the smaller artery to the larger proximal draining vein. Most FTAVF are located from L3 to L5 and, in 80% of cases, are supplied by one feeder, the artery of the filum terminale. However, feeding arterial supply from the LSA and middle sacral artery in addition to the artery of the filum terminale has been reported in at least four cases.6 11–13 While there is some controversy as to whether or not dural feeders such as the LSA or middle sacral artery can supply FTAVF, these arteries can be recruited in the setting of a high flow fistula as demonstrated in figure 4.
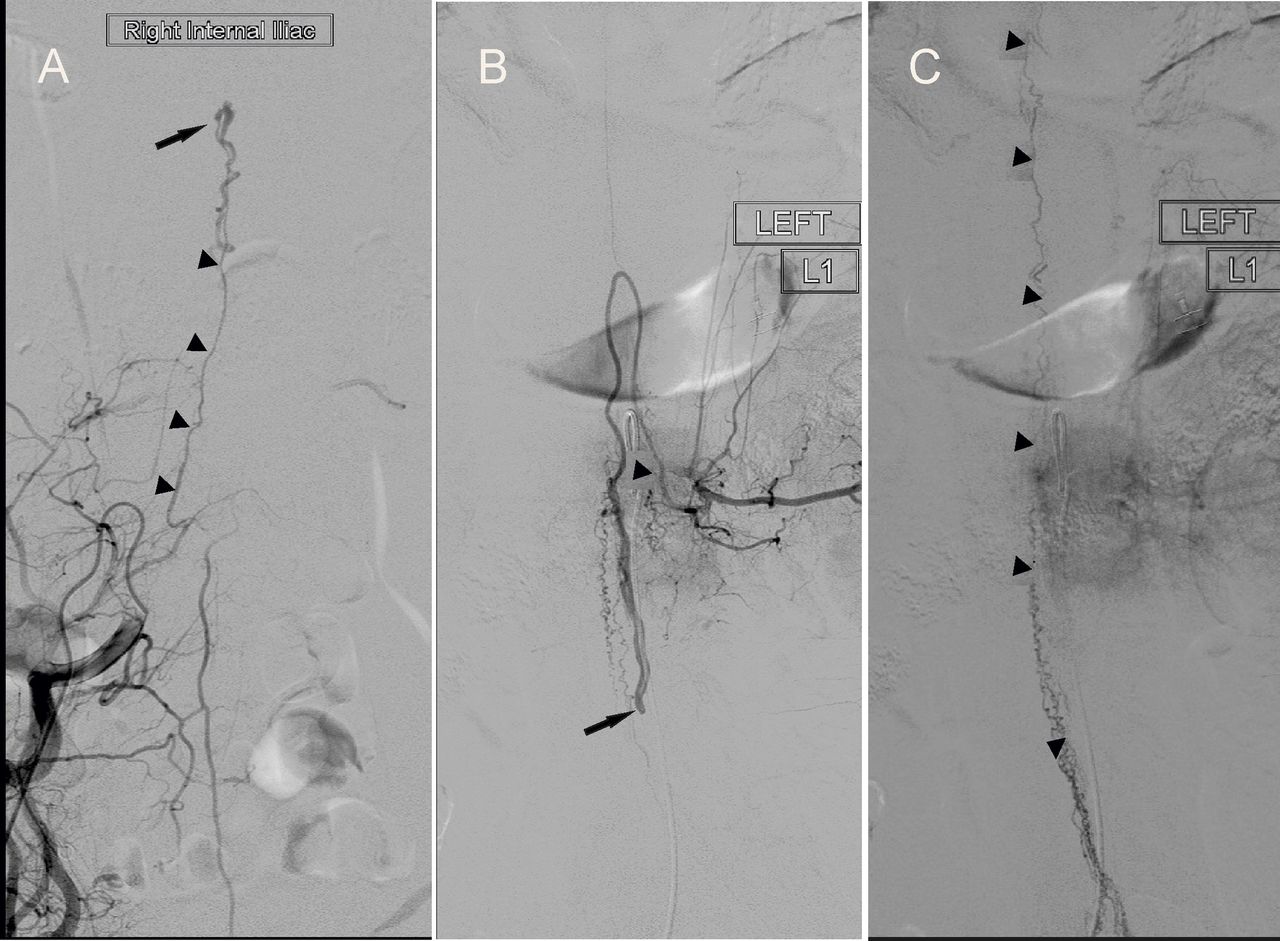
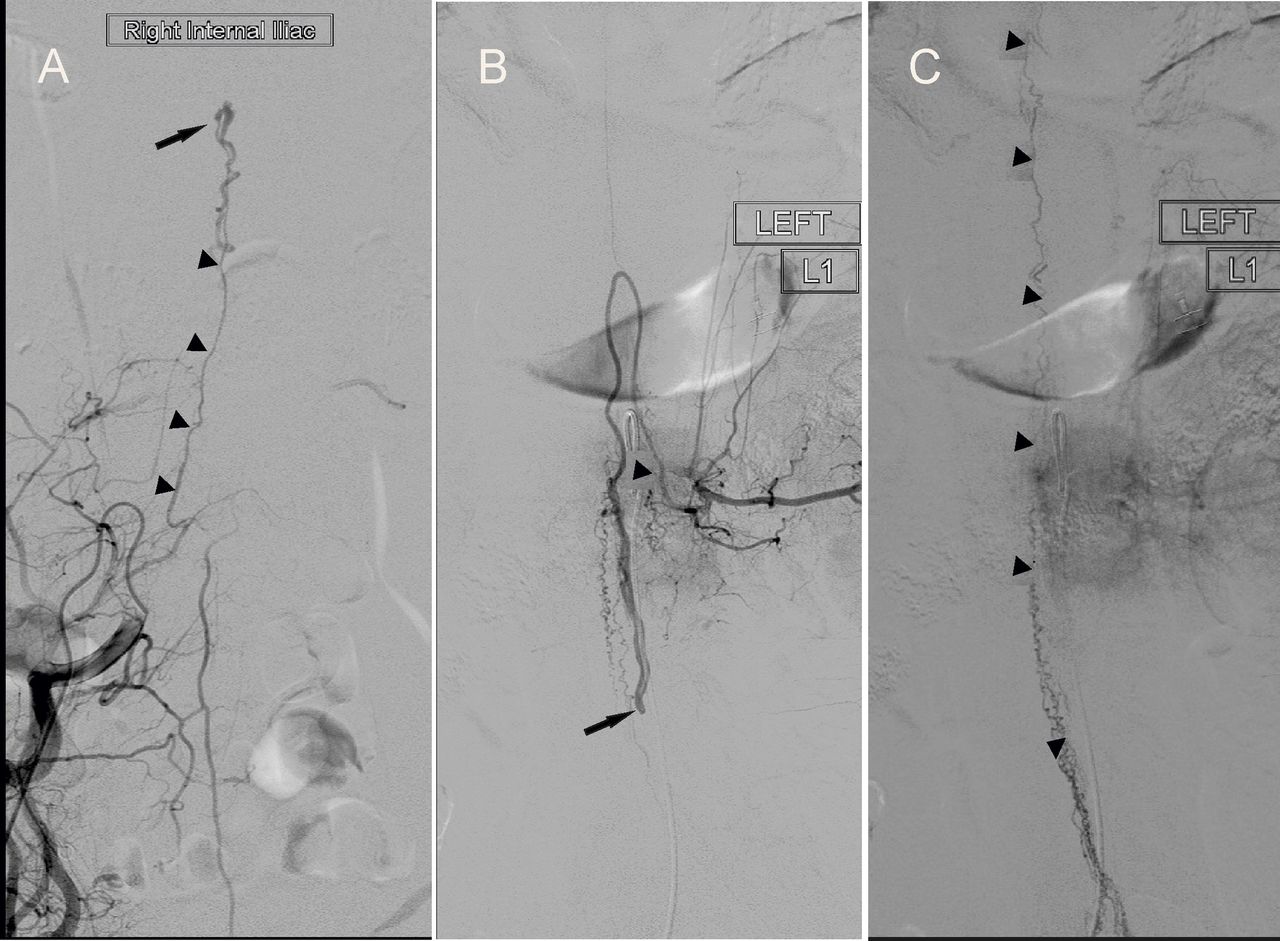
(A) Same patient as in figures 2 and 3. Spinal angiogram shows an arteriovenous fistula of the filum terminale at L3–L4 level (black arrow) fed by the right lateral sacral artery (arrowheads). (B) Spinal angiogram in a different patient with a longstanding history of complete loss of function below the T12 level shows an arteriovenous fistula at the level of the L2–L3 interspace (arrow) fed by the anterior spinal artery arising from the left L1 lumbar artery. (C) Same patient as in figure 4B, late venous phase, shows venous drainage running both cranially and caudally along the spinal cord and cauda equina (arrowheads).
Treatment
The ultimate therapeutic goal of FTAVF treatment is complete obliteration of the fistula with preservation of the spinal cord circulation. This can be achieved through both surgical and endovascular strategies. The key factor in treating these lesions is safe isolation of the feeding artery, fistulous point, and draining vein.
A number of factors play a role in the decision of whether a lesion should be treated with endovascular or surgical techniques, including preoperative morbidity and functional status, local expertise and angioarchitecture of the fistula, and size and tortuosity of the feeding artery. Both endovascular and surgical techniques can be safe and effective in the treatment of these lesions.29
Some authors suggest that the distance from the top of the arterial feeder to the fistulous point should be taken into consideration in determining the choice of treatment.13
Surgical techniques
Surgical treatment is the favored technique for most of these lesions as approximately 75% of the cases in the literature have been treated surgically. Monitoring of somatosensory and motor evoked potentials is a useful adjunct to both surgical and endovascular treatment to secure good clinical outcomes and avoid spinal cord infarct.2 6 8 9 11 12 16 18 20 21 27–34 Surgery is suggested when the FTAVF has a single feeder with long distance to the AVF and is generally thought to be safer than endovascular treatment.34 The overall success rate is close to 100%, and complication rates are low (<5%).15 21
Surgical obliteration requires a precise intraoperative view of the fistulous point in order to avoid injury or occlusion of normal spinal vessels.8 A laminectomy, with removal of the ligamentum flavum, is required to expose the dura. We prefer a linear midline durotomy followed by separate opening of the arachnoid. The roots of the cauda equine are gently displaced to expose the filum. The feeding artery can then be recognized as it is smaller than the other parallel draining vein. Intraoperative ICG fluorescein angiography is very useful in identifying the exact shunt location. In the proximity of the actual connection, the artery and the vein may actually be in tight contact for a segment longer than the shunt itself. Separation of the artery and the vein along this area of tight adherence is important to occlude the fistula at the exact location of the shunt. After the connection is identified, we place a temporary clip to interrupt the shunt while we monitor electrophysiological parameters to make sure that occlusion of the shunt does not interfere with neural function. Considering that FTAVF are fed by the ASA, and that the filum terminale has no neurologic function, some authors suggest sectioning of the filum above the fistulous point.24 Although this strategy has been reported to be successful in three cases,20 24 we do not think sectioning of the filum is necessary if the actual fistula is identified and occluded. Intraoperative spinal angiography has been shown to be technically feasible, safe, and helpful in identifying vascular angioarchitecture during and after the procedure but we do not consider it necessary with the availability of ICG fluorescein.
Endovascular techniques
Embolization of FTAVF requires microcatheter selection of the arterial feeder and navigation towards the most distal part of the artery, just proximal to the fistula. Endovascular treatment is preferred if a safe microcatheterization close to the fistulous point can be achieved.1–4 13 16 21 24 35 Due to the high risk of tearing/dissecting the ASA while trying to navigate a very small vessel or causing thrombosis and vasospasm, especially when inserting and withdrawing the microcatheter system, we and others recommend surgical treatment considering the low morbidity associated with this type of surgery and the high occlusion rates.1 2 13 In cases of high flow fistulae, the ASA can be markedly dilated, which can make catheterization of the vessel safer.6 Some authors prefer to perform neurophysiologic monitoring of motor and somatosensory evoked potentials during such embolization procedures as well as provocative testing with intra-arterial lidocaine,36 although the reliability of this provocative test is controversial because of the possibility of reflux of the anesthetic agent, which may invalidate the test and give a false positive.
Due to the lack of neural structures within the filum terminale, embolization of FTAVF fed by non-ASA feeders should carry a low risk. In cases where there are multiple feeders including the ASA, there is always a risk of causing ASA injury due to reflux of embolic material. This is probably more common with newer liquid embolic agents such as Onyx than glue due to the marked permeability of Onyx. Liquid polymers such as butyl-2-cyanoacrylate (glue) allow for more precise control with satisfactory results.31 Coils can also be used to occlude larger shunts. Like in any AV fistula, the key to complete and durable occlusion is obliteration of the proximal draining vein along with the actual fistulous point. Overall, embolization was performed in 33% of reported cases with an overall complete obliteration rate of 76%. In two cases, embolization was attempted but failed, and patients required definitive surgical intervention.1 10 29
Outcome and follow-up
After the obliteration of FTAVF, regardless of the type of treatment, the pressure in the spinal veins will decrease, which invariably results in gradual improvement, or at least stabilization, of symptoms.1 Progressive improvement, although not necessarily complete regression, of motor and sensory symptoms occurs in >90% of cases. Similar to patients with type I spinal dural arteriovenous fistulae, bladder and bowel dysfunction, when present, are less likely to improve.6 24 28
Radiological signs of treatment success included reduced size of the dilated perimedullary veins, decreased cord swelling, and decreased spinal cord hyperintensity on T2 weighted MRI (figure 5). However, there is often not a direct correlation between radiological and clinical improvement.6 37 Regarding angiographic follow-up, although some authors prefer MRA due to its less invasive nature, we feel that, except in very selected cases, angiography is necessary to confirm complete exclusion. After a negative (for persistence of the fistula) postoperative DSA, MRI with MRA is indicated to confirm persistent obliteration and demonstrate progressive improvement/resolution of MRI findings caused by the fistula. After definitive treatment, recurrence of the fistula is quite rare, being described only in one case after inadequate distal embolization of fistula feeders.13

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Preoperative imaging showing edema and enlargement of the spinal cord with increased T2 signal change. (B) Three months after successful surgical treatment (not shown) there is normalization of the diameter of the cord with reduction of the edema as demonstrated by the regression of the T2 changes with decreased cranial extension when compared with the preoperative images.
Conclusion
FTAVF are rare lesions, often presenting with symptoms secondary to venous hypertension and congestive myelopathy. These fistulae consist of a direct arteriovenous shunt located below the conus medullaris along the course of the filum terminale. The shunt is more commonly between the continuation of the anterior spinal artery, after it has become the artery of the filum terminale and an enlarged draining vein, with the high pressure being transmitted cephalad to affect drainage from the conus and spinal cord. Catheter angiography is the gold standard to demonstrate the specific type and location of the fistula and to precisely define the angioarchitecture. Because of the small size and the tortuosity of the feeding artery, surgery is often the preferred treatment, while endovascular treatment is a reasonable alternative in cases where distal safe catheterization immediately proximal to the fistulous connection can be achieved. The majority of patients will experience improvement of their motor and sensory symptoms, and recurrences, after definitive treatment, are extremely rare.
References
Footnotes
Contributors EG, WB, and GL were involved in the conception and design of the work. EG and WB were in charge of data collection, data analysis and interpretation, and in drafting the article. EC and GL critically reviewed the article. All authors approved the final version.
Competing interests GL is a consultant for Medtronic. All other authors have no competing interest to declare.
Provenance and peer review Not commissioned; externally peer reviewed.