Article Text

Abstract
Background COVID-19 infections have been shown to be associated with a range of thromboembolic disease.
Objective To describe our endovascular experience in a consecutive series of patients with COVID-19 who presented with large vessel occlusions, and to describe unique findings in this population.
Methods Mechanical thrombectomy was performed on five consecutive patients with COVID-19 with large vessel occlusions. A retrospective study of these patients was performed. Patient demographics, laboratory values, mechanical thrombectomy technique, and clinical and angiographic outcomes were reviewed.
Results Four patients with COVID-19 presented with anterior circulation occlusions and one patient with COVID-19 presented with both anterior and posterior circulation occlusions. All patients had coagulation abnormalities. Mean patient age was 52.8 years. Three patients presented with an intracranial internal carotid artery occlusion. Two patients presented with an intracranial occlusion and a tandem thrombus in the carotid bulb. One patient presented with an occlusion in both the internal carotid and basilar arteries. Clot fragmentation and distal emboli to a new vascular territory were seen in two of five (40%) patients, and downstream emboli were seen in all five (100%) patients. Patient clinical outcome was generally poor in this series of patients with COVID-19 large vessel occlusion.
Conclusion Our series of patients with COVID-19 demonstrated coagulation abnormalities, and compared with our previous experience with mechanical thrombectomy in large vessel occlusion, this group of patients were younger, had tandem or multiple territory occlusions, a large clot burden, and a propensity for clot fragmentation. These patients present unique challenges that make successful revascularization difficult.
- embolic
- infection
- stroke
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The COVID-19 virus has been shown to be associated with thromboembolic disease through mechanisms of hypoxia, inflammation, and diffuse intravascular coagulation.1 In a recent Dutch study, there was a 31% incidence of thrombotic complications in patients with COVID-19 admitted to the intensive care unit (ICU), largely consisting of acute pulmonary embolism, deep vein thrombosis, ischemic stroke, myocardial infarction, and systemic arterial embolism.1 A few reports have described the invasive nature of COVID-19 for the central nervous system. Mao et al reported a 24.8% incidence of neurological manifestations among 214 patients with COVID-19 in Wuhan, China.2 Specifically, 2.8% of these patients presented with acute cerebrovascular disease.2
The tendency of patients with COVID-19 to manifest with prothrombotic disease has implications for the neuroendovascular management of large vessel occlusions (LVOs).3 We discuss five consecutive COVID-19 positive patients who presented to our institution with anterior and posterior circulation LVO. Our observations in this series of five COVID-19 positive patients with stroke who underwent thrombectomy aims to identify patient demographic and technical features that may be unique to patients with this infection. Patient demographics, procedural details, and outcomes are discussed.
Methods
We report a case series of five consecutive COVID-19 positive patients in whom endovascular thrombectomy (EVT) was performed to treat LVO. Institutional review board approval was obtained. COVID-19 testing was performed using a nasal swab. Additional radiological imaging was obtained, usually in the form of a chest X-ray examination or CT of the chest, corroborating the infection. In all cases, CT angiography demonstrating the location of the occlusion was performed prior to thrombectomy. All cases were performed under general endotracheal anesthesia using a stent-aspiration combination as primary thrombectomy technique. Intravenous heparin was administered when a balloon guide catheter was used for proximal flow arrest. The technical details of each case and the angiographic outcome are described below. All patients recovered in the neurological ICU. Routine laboratory tests, including D-dimer, platelet count, coagulation panel (activated partial thromboplastin time (aPTT), international normalized ratio), interleukin-6 (IL-6), erythrocyte sedimentation rate, and C-reactive protein, were evaluated in all patients. Rotational thromboelastography (ROTEM) (ROTEM; TEM International, Munich, Germany) was performed on the patients’ blood samples to assess real-time clot formation/dissolution properties (figure 1).

Rotational thromboelastography (ROTEM) results of a patient with COVID-19 undergoing thrombectomy. Important ROTEM parameters of maximum clot firmness (MCF) and clot formation time (CFT) in both the intrinsic and extrinsic coagulation pathways are represented by the graphs. MCF represents the maximum strength of the clot. CFT represents the time needed for first clot to form. This patient has a characteristic profile of a procoagulant patient with elevated MCF and reduced CFT.
Results
Four patients had anterior circulation large vessel occlusion and one patient had both anterior and posterior circulation occlusions. Mean age was 52.8 years and four patients were male. Thrombolysis in cerebral infarction (TICI) 3 revascularization was achieved in one patient, TICI 2b in two patients, and TICI 2a in two patients (table 1). All patients presented with elevated D-dimer levels, which are suggestive of a hypercoagulable state. After thrombectomy ROTEM analysis in all patients supported the hypercoagulable state in these patients with COVID-19 (figure 1). Additionally, erythrocyte sedimentation rate, C-reactive protein, and IL-6 levels were elevated, suggestive of active viral infection. Coagulation laboratory tests, including PTT, and international normalized ratio, were also elevated.
Details of mechanical thrombectomy performed in five consecutive COVID-19 positive patients with large vessel occlusion
Patient 1
A patient in their 50s with coronary artery disease and partial lung lobectomy presented with a left inferior middle cerebral artery branch occlusion and tandem thrombus in the left carotid bulb (figure 2). The internal carotid artery (ICA) had a partial thrombus and so both the cervical ICA thrombus and the intracranial occlusion were visualized. Patient was last known normal 2 hours prior to presentation, with a National Institutes of Health Stroke Scale (NIHSS) score of 27, and received intravenous tissue plasminogen activator (IV-tPA) en route to the angiosuite. A 6F Neuron Max catheter (Penumbra Inc., Alameda, California, USA) was first used for suction aspiration alone on the carotid bulb thrombus. This resulted in clot fragmentation and distal emboli into the supraclinoid ICA. A Solitaire (Medtronic, Minneapolis, Minnesota, USA) 6×40 mm stent was deployed across the occlusion and in combination with suction aspiration through a 6F Sophia Plus intermediate catheter (Microvention, Mission Viejo, California, USA). Three attempts were performed for clot retrieval. Each attempt resulted in distal clot fragmentation and eventual downstream migration into a M3 branch. TICI 2a revascularization was achieved in the end. The patient had a prolonged ICU course including worsening cardiopulmonary function and ultimately died of COVID-19 related complications.
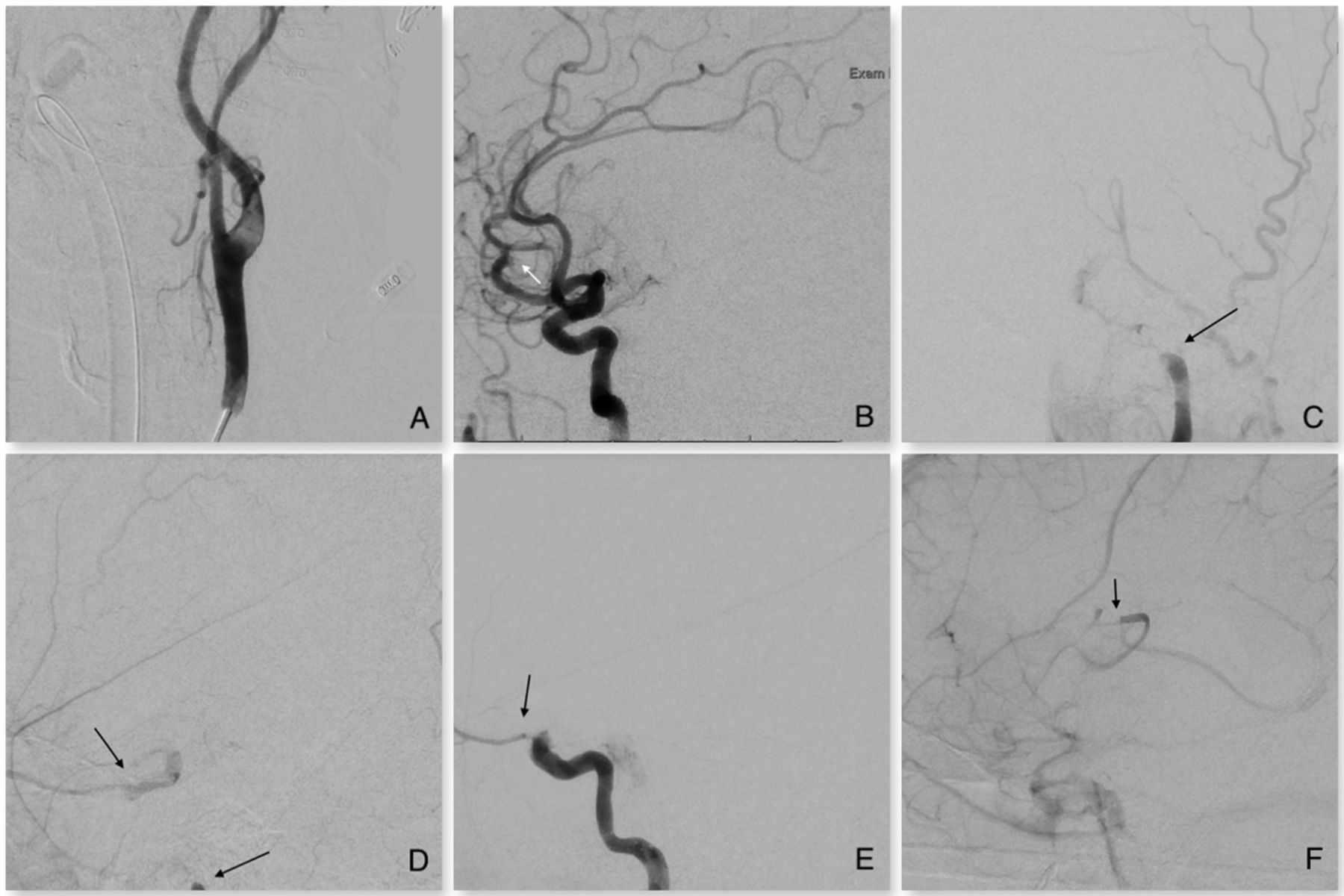
Patient No 1 in their 50s with a National Institutes of Health Stroke Scale score of 27 presents with a proximal left inferior M2 occlusion and proximal thrombus within the left carotid bulb (A, B). Suction thrombectomy of the proximal carotid bulb thrombus resulted in clot fragmentation and distal Internal carotid artery (ICA) occlusion with retrograde filling of the supraclinoid ICA from the ophthalmic artery (C, D). Solitaire stent thrombectomy with aspiration propagated the clot distally into the supraclinoid ICA (E). Two additional stent passes fragmented the clot with distal propagation into a M3 branch (F). Arrows indicate site of occlusion.
Patient 2
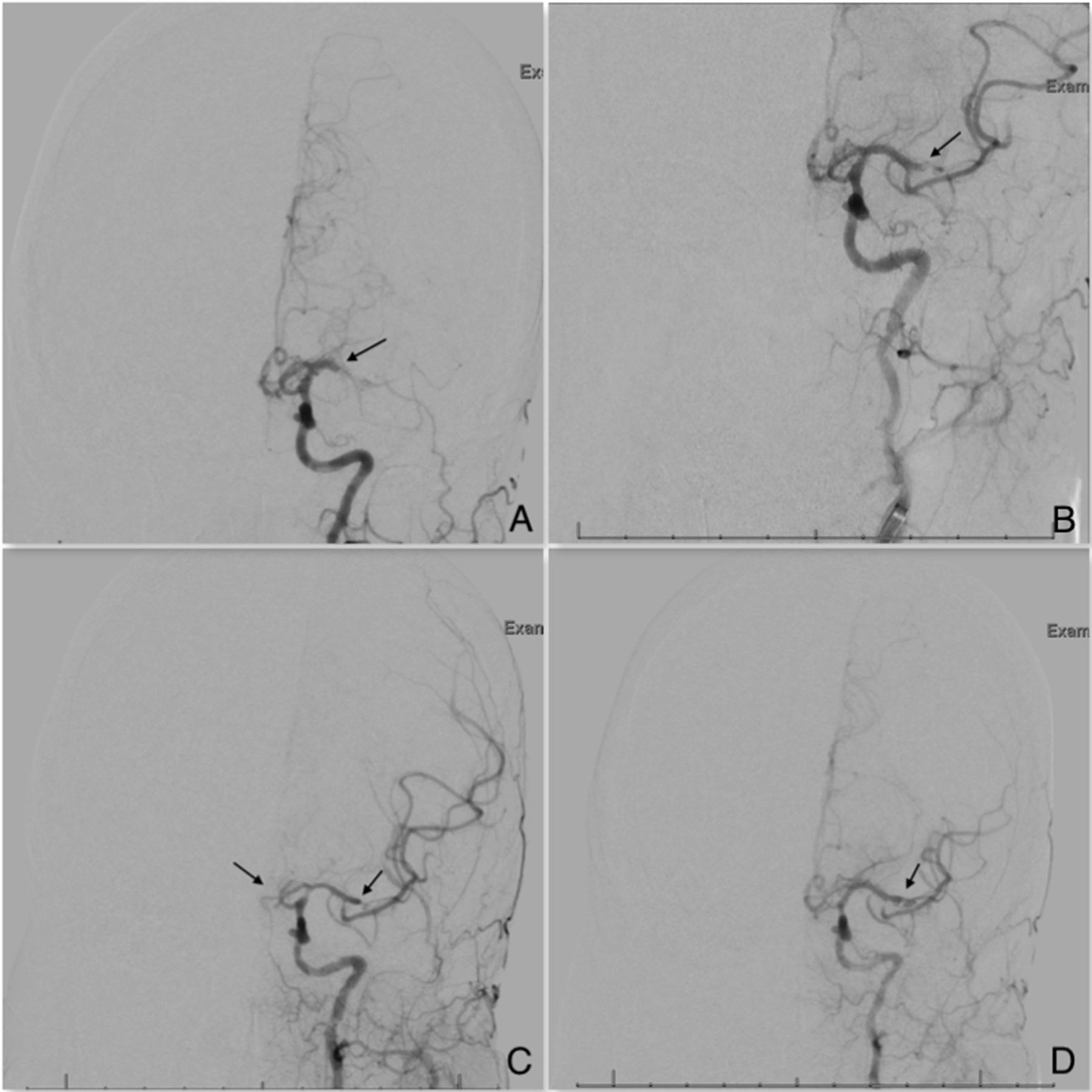
A patient in their 60s with no underlying medical risk factors presented with a left ICA terminus occlusion in conjunction with a left pulmonary artery embolus (figure 3). The patient was last known normal 2 hours prior to presentation, had a NIHSS score of 29 and received IV-tPA en route to the angiosuite. Stent-aspiration combination therapy was attempted using a Jet 7 (Penumbra Inc., Alameda, California, USA) aspiration catheter and a Solitaire 6×40 mm stent. After the first attempt, the ICA was initially recanalized but then quickly re-occluded within a few minutes without intervening intervention. No underlying ICA stenosis was seen. Three attempts were made, and clot fragmentation with distal emboli into a new territory, the anterior cerebral artery territory (ACA), and into downstream middle cerebral artery branches was seen. TICI 2b revascularization was achieved in the end. The patient had a prolonged ICU course including worsening cardiopulmonary function and ultimately died of COVID-19 related complications.

Patient No 2 in their 60s with a National Institutes of Health Stroke Scale score of 29 presents with a left internal carotid artery terminus occlusion and acute left pulmonary artery embolus (A, B). After the initial pass with a Solitaire stent under aspiration, the occlusion was partially opened with distal clot migration into the left M1 and A1 (C). Second pass stent-aspiration combination thrombectomy resulted in clot migration into the A2 branch and M2 branch (D). The final result after a third pass of the stent resulted in thrombolysis in cerebral infarction 2b revascularization with occlusion of the A2 segment and M3 branch (E, F). Arrows indicate site of occlusion.
Patient 3
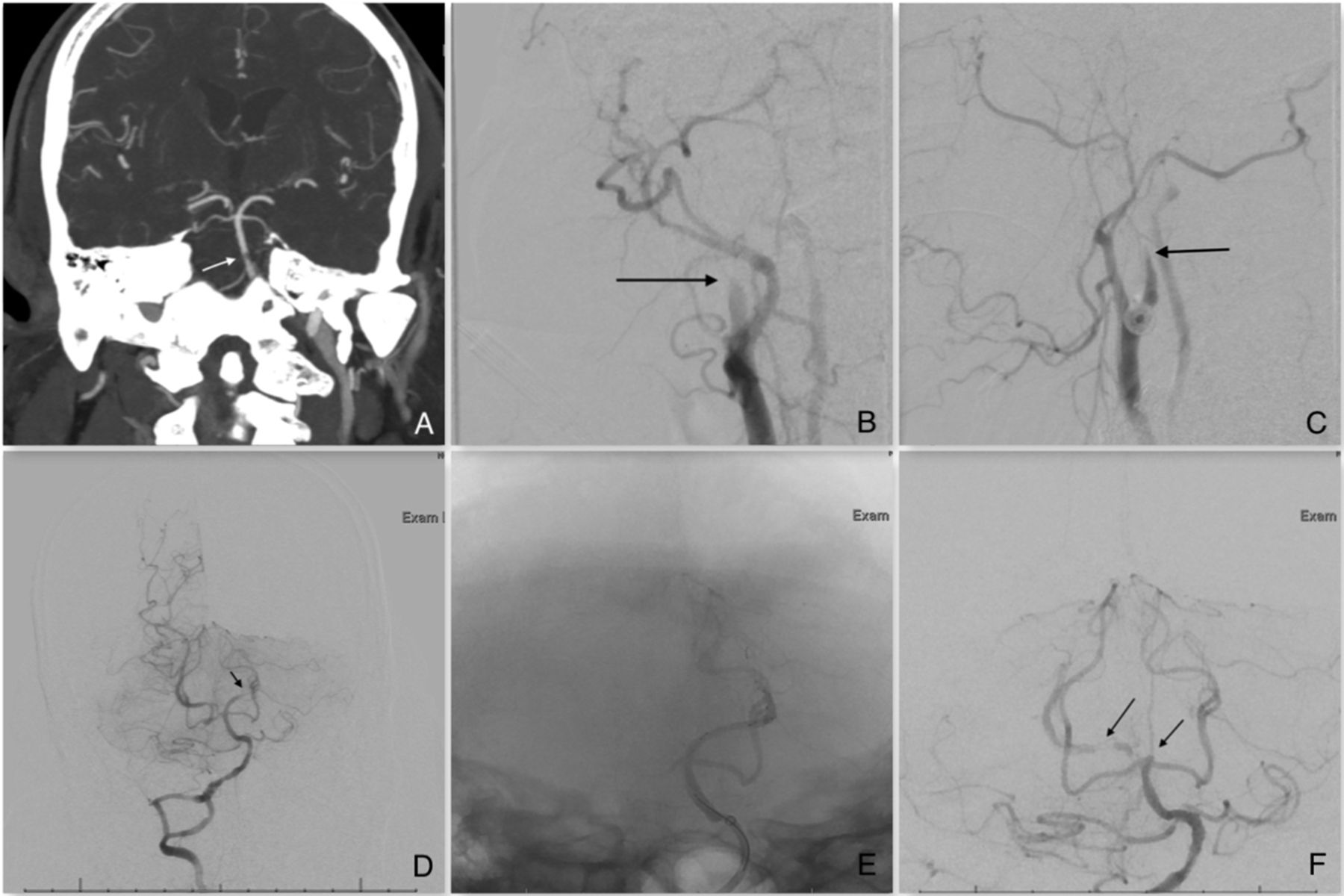
A patient in their 50s with coronary artery disease presented with a basilar artery occlusion (figure 4). The patient was last known normal 1 hour prior to presentation, had a NIHSS score of 28 and received IV-tPA. Initial injections of the innominate artery demonstrated slow arterial flow in the right common carotid artery and further investigation revealed a right proximal ICA occlusion in conjunction with the basilar occlusion. After 2000 units of intravenous heparin were administered, a 9F Cello balloon guide catheter (Medtronic, Minneapolis, Minnesota, USA) was used for proximal flow arrest in the right common carotid artery. A combination of stent-aspiration thrombectomy was performed using a Solitaire 6×40 mm stent and a Penumbra ACE 68 aspiration catheter. The carotid artery was completely open and TICI 3 revascularization was achieved in the anterior circulation stroke. The 9F Cello was then placed in the mid cervical right vertebral artery and the Solitaire 6×40 mm and ACE 68 were used for thrombectomy of the basilar artery. After two attempts, the basilar artery was opened; however, clot fragmentation and distal emboli to bilateral posterior cerebral arteries was seen. TICI 2b revascularization of the basilar occlusion was achieved in the end. The patient had a prolonged ICU course including worsening cardiopulmonary function and ultimately died of COVID-19 related complications.

Patient No 3 in their 50s with a National Institutes of Health Stroke Scale score of 28 presents with a partial basilar artery occlusion on CT angiogram (A). Cerebral angiography revealed a basilar thrombus and concomitant left cervical internal carotid artery (ICA) occlusion (B, C). The ICA occlusion was opened with stent-aspiration combination. The basilar occlusion was opened with stent-aspiration combination under balloon guide proximal flow arrest in the right vertebral artery (D). Distal clot migration into the the left P1 segment is seen after first pass of the stent (D). Two additional attempts were made to revascularize the P1 segment, without success, with partial thrombus within the right posterior cerebral artery as well (E, F). Arrows indicate site of occlusion.
Patient 4
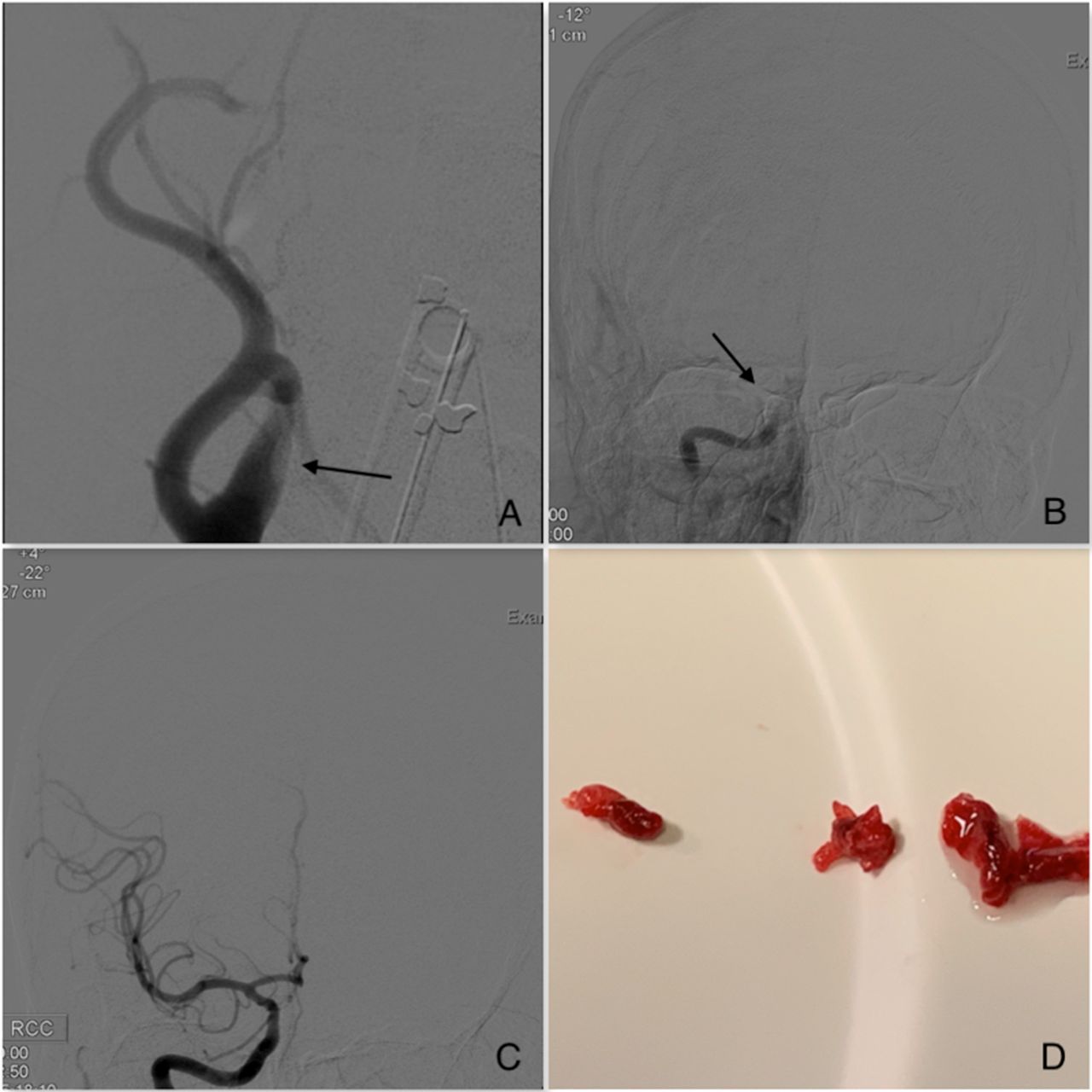
A patient in their 30s with hypertension morbid obesity, and diabetes presented with a right ICA occlusion just distal to the ophthalmic artery, and a partially occlusive thrombus in the right carotid bulb (figure 5). The patient was last known normal 2.5 hours prior to presentation, had a NIHSS score of 10 and received IV-tPA. A 6F Neuron Max was placed in the common carotid artery and initial Solitaire stent retrieval with a contact aspiration catheter was unsuccessful. Primary suction aspiration was then performed with a Penumbra Jet 7 catheter. TICI 3 revascularization was achieved. Clot specimen visualization showed a predominantly reddish composition with minimal white clot, suggesting a mix clot composition and potential fragility to manipulation. Patient was discharged from the hospital with a NIHSS score of 1.

Patient No 4 in their 30s with a National Institutes of Health Stroke Scale score of 10 presents with a right internal carotid artery terminus occlusion and thrombus in the right carotid bulb (A, B). initial Solitaire stent retrieval was unsuccessful. Primary suction aspiration was then performed, resulting in a thrombolysis in cerebral infarction 3 revascularization. A clot specimen showed a predominantly reddish clot with areas of white, suggesting a mixed clot composition (D).
Patient 5
A patient in their 40s with no underlying medical comorbidities presented with a left M1 occlusion (figure 6). The patient was last known normal 1.5 hours prior to presentation, had a NIHSS score of 20, and received IV-tPA. Stent-aspiration combination therapy was attempted using a Jet 7 aspiration catheter and a Solitaire 4×20 mm stent. After the first pass with the stent, the clot migrated distally into the superior M2 division. After the second pass of the stent in the superior M2 division, distal emboli to the A1 segment and persistent M2 occlusion was seen. After a third pass of the stent in the M2 occlusion, the M2 division continued to be occluded but partial flow was re-established in the ACA. Patient on last clinical follow-up had a NIHSS score of 15.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Patient in their 40s with a National Institutes of Health Stroke Scale score of 20 presents with a left M1 occlusion (A). Stent-aspiration combination therapy was attempted using a Jet 7 aspiration catheter and a Solitaire 4×20 mm stent. After the first pass with the stent, the clot migrated distally into the superior M2 division (B). After the second pass, distal emboli to the A1 segment were seen (C). After three stent passes, partial flow was re-established in the anterior cerebral artery but distal emboli persisted in the M2 branch (D).
Discussion
We report a series of patients with COVID-19 undergoing EVT for LVO and highlight the technical challenges encountered in these patients. While EVT has proved to be effective in LVO, our experience shows that patients with COVID-19 are more likely to have worse radiographic and clinical outcomes after EVT, associated with clot in multiple locations, clot fragility, and extensive clot burden.
From a patient demographic perspective, our group of patients were on average younger and presented with a higher NIHSS score than patients enrolled in MR CLEAN, EXTEND IA, ESCAPE, SWIFT-PRIME, REVASCAT.4–8 In our cohort, patients were on average 52.8 years old and presented with a median NIHSS score of 27 compared with a mean age of 65–69 years and median NIHSS score of 17 in the five landmark EVT trials.4–8 Similarly, another institution’s recent experience with five patients with COVID-19 presenting with LVO demonstrated an average age of 40.4 years and average NIHSS score of 16.8 in their patient cohort.9
The higher NIHSS scores in our cohort can be understood when taking the location of the occlusion into consideration. All our patients had proximal occlusions. Three patients presented with intracranial ICA occlusions. Two patients presented with a tandem carotid bulb thrombus in conjunction with an intracranial vessel occlusion. One patient had an ICA terminus occlusion with a concomitant basilar occlusion. In a meta-analysis of the patient data from the five randomized trials, the HERMES collaborators showed that location of the occlusion was most commonly in the M1 segment (69% of patients) followed by the ICA (21% of patients) and then the M2 segment (8% of patients).10
We observed two noteworthy findings in our patients. First, the most common occlusion in our patients was an intracranial ICA occlusion with a tandem partial thrombus within the carotid bulb (patients 1 and 4). We believe this finding may be explained by the significant systemic hypercoagulability seen in our patients. All patients had elevated D-dimer and IL-6 levels on admission. IL-6 is a powerful proinflammatory cytokine, which induces fibrinogen synthesis and is a marker of the 'cytokine storm' seen in patients with COVID-19. The high levels of IL-6 in our patients suggest that our patients with stroke had active infection at the time of LVO detection. ROTEM evaluation demonstrated that all five patients were in a hypercoagulable state (figure 1). In addition, one of our patients also had an acute pulmonary embolus on presentation as captured on CT angiography of the neck (Patient 2, figure 3). Patient 3, who initially was found to have only a partial basilar occlusion on CT angiography of the head was found to have a full basilar occlusion and new thrombus formation within the right proximal cervical ICA on angiography within 30 min of obtaining non-invasive vessel imaging (figure 4). Ranucci et al reported their observations of the hypercoagulability of patients with COVID-19 admitted to the ICU. In their cohort of 16 patients, many patients demonstrated prolonged aPTT, D-dimer, and IL-6 levels and ROTEM results with hypercoagulability profiles.3 Second, the intravascular clots in all our patients were prone to fragment and migrate into both new vascular territories and into distal downstream vasculature. Distal emboli into a different territory (ACA occlusion) was seen in two of our five patients (40%) and distal emboli in a downstream territory were seen in all five patients (100%). In comparison, Jovin et al in the REVASCAT trial only demonstrated a 4.9% rate of distal embolization in a different territory.8 For our patients, an average of 2.7 stent-retriever passes was needed to achieve a final TICI revascularization of 2b or better. In two patients, only TICI 2a was achieved. Additionally, in two patients we encountered re-occlusion of the vessel within minutes of recanalization with a stent retriever. We believe this event is a secondary sequela of the patient’s systemic hypercoagulability. Examination of the clot after retrieval demonstrated a predominantly reddish clot suggestive of high red blood cell content.
At our institution, we have three neurointerventionalists who use a combination of stent retriever with clot-contact suction aspiration as the mainstay technique for EVT. The general technique involves a non-balloon proximal guide catheter, integration of the stent and the thrombus, and intermediate suction catheter clot contact aspiration. As demonstrated in our cases, we found that use of a stent is associated with clot fragmentation and emboli into both new vascular territories and downstream distal vasculature. This event was seen in all our patients. It is unclear whether clot fragmentation was a result of the thrombectomy technique used or the consistency/composition of the clot or the administration of IV-tPA in COVID-19 infected patients; however, the rate of fragmentation and distal embolization far exceeds our usual experience. Given that distal emboli were encountered by all authors of this study, it suggests that the problem is due to clot composition rather than technique. Our two most successful revascularizations: TICI 3 in an intracranial ICA occlusion in patient 4 used primary suction aspiration, which resulted in a TICI 3 revascularization, and TICI 3 in patient 3, in whom a balloon-guide catheter was positioned and inflated in the common carotid artery prior to removal of a proximal ICA thrombus. However, the same approach was not successful with the posterior circulation thrombus. While we hesitate to speculate that any particular technique will prevent distal embolization, we feel it is important to document this embolic phenomenon in our COVID-19 positive patients with stroke.
We also feel it is important to document our anesthetic technique for these patients, as it was a deviation from our general practice. Many of our thrombectomies were performed with non-intubated monitored anesthesia care prior to the COVID-19 era. The preference of our neuro-anesthesia team is to perform general endotracheal anesthesia for COVID-19 positive and suspected patients. Because COVID-19 can persist in aerosols for hours, making aerosol transmission possible, the threshold for use of general anesthesia for endovascular thrombectomy may be reduced during the COVID-19 pandemic.11 Recommendations suggest that intubation and extubation of these patients should occur in a negative pressure room, that airborne precautions, including proper personal protective equipment (PPE), should be used for the intubation, and a high-efficiency particulate air (HEPA) filter should be placed directly on the tracheal tube immediately after intubation.11 Additionally, all personnel should wear PPE, including, surgical caps, goggles/face shield, N95 masks, gown/gloves, and boot-type show covers.12 In Europe, ESMINT has recommended that clinical management of patients with suspected or confirmed COVID-19 should be according to local hospital protocols. The European society highlight the importance of PPE use for essential staff and the efficient use of angiosuites and equipment to avoid cross-contamination.13 We do not feel that this has an effect on the success of our mechanical thrombectomies or clinical outcome, but variations in blood pressure and oxygenation may have an impact and should be considered when choosing anesthetic technique, while making every attempt to limit transmission of the infection to treating personnel.
The documented hypercoagulable state of these patients with COVID-19 requires significant future study. Anecdotal reports of systemic thrombolytic use for venous and arterial thrombotic events in other organ systems have been shared among physicians in New York treating COVID-19 positive patients. Future study is also needed of proper treatment of the infection itself with experimental agents such as hydroxychloroquine, azithromycin, and remdesivir. Many potential treatments exist for these thromboembolic complications of the COVID-19 disease such as thrombolytics, anticoagulants, anti-inflammatory agents, and antiplatelet agents.
Our study has limitations. This is a retrospective review of a small number of patients. Our goal is to document the unique presentation and technical findings of our early experience with patients with COVID-19 positive LVO in this rapidly evolving pandemic. We have an ongoing investigation of the histological and microbiological composition of the retrieved clot, which we hope will assist in the understanding of our findings. COVID-19 registries are also being developed, which will assist in our approach to these patients.
Conclusion
Our series of COVID-19 infected patients presenting with acute stroke and LVO have documented hypercoagulability, younger age, more severe strokes with larger clot burdens, tandem and multiple distribution occlusions, clot fragility, and distal migration during mechanical thrombectomy. Neurointerventionalists should be prepared for a deviation in the presentation of our patients with stroke, and in the technical aspects of mechanical thrombectomy during the COVID-19 pandemic.
Footnotes
Contributors AW made substantial contributions to the conception and design of the work; the acquisition, analysis, and interpretation of data for the work; and drafting the work for important intellectual content. GKM, PDY, PMM, SDL provided final approval of the version to be published, revised the scientific content and appraised it critically for important intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval We obtained ethics approval for this study from the Columbia University institutional review board (IRB). IRB protocol number is IRB-AAAT0153. Participants gave informed consent before taking part in this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. De-identified participant data.