Article Text

Abstract
Endovascular thrombectomy has revolutionized the management of acute ischemic stroke from emergent large vessel occlusion. Continued technological advancement in the field, as evidenced by successive introduction of large bore aspiration catheters with enhanced trackability and large inner diameter, has played a major role in achieving fast and robust recanalization and improved clinical outcome. Here, we present three patients with intraprocedural device malfunction related to the JET 7 XTRA Flex reperfusion catheter.
- thrombectomy
- catheter
- complication
- stroke
- device
Statistics from Altmetric.com
Introduction
Endovascular thrombectomy (EVT) has been established as standard of care for patients with acute ischemic stroke from emergent large vessel occlusion who meet other eligibility criteria.1 EVT using a stent retriever has been the dominant standard technique in major randomized clinical trials. However, the direct aspiration first pass technique has emerged as a comparably effective and safe thrombectomy technique in recent years.2 3
Successive introduction of new generations of the large bore aspiration catheters with improved navigability and larger inner diameter has revolutionized EVT by increasing efficacy and safety, shortening procedure times, and likely improving outcomes.4 The Penumbra (Penumbra, Alameda, California, USA) JET 7 XTRA Flex reperfusion catheter is the seventh generation reperfusion catheter from the Penumbra system which was approved for EVT in acute ischemic stroke from emergent large vessel occlusion by the Food and Drug Administration (FDA) in August 2018.5 Initial experience using the JET 7 XTRA Flex reperfusion catheter was promising, with a high rate of successful recanalization and low complications.6
We present three cases of intraprocedural JET 7 XTRA Flex reperfusion catheter malfunction, two associated with mortality. Of note, these procedures were performed by three independent surgeons in two different institutions.
Case descriptions
Patient No 1
A patient in their 70s presented with acute onset left sided weakness with a National Institutes of Health Stroke Scale (NIHSS) score of 14. CT angiography (CTA) of the head and neck revealed right internal carotid artery (ICA) terminus occlusion and a likely right ICA dissection. The patient was taken for emergent EVT.
A 6 F NeuronMax guide catheter (Penumbra) was advanced over a 5 F Selection catheter into the right ICA from a right radial artery access. An angiographic run of the right ICA revealed an ICA terminus occlusion. A JET 7 XTRA Flex reperfusion catheter was advanced over a Velocity microcatheter (Penumbra) and a Stroke Wire (Scientia Vascular LLC, West Valley City, Utah, USA) into the right ICA. The microcatheter and microwire advanced into the M2 segment of the right middle cerebral artery (MCA) and a 5×33 mm Embotrap stentriever (Cerenovus, Irvine, California, USA) was deployed within the clot. The microcatheter was removed and the JET 7 XTRA Flex catheter was further advanced to face the thrombus in the right ICA terminus. It was connected to the aspiration pump and the system removed. A follow-up angiographic run via the guide catheter revealed Thrombolysis in Cerebral Infarction (TICI) 3 recanalization.
The previously seen dissection in the cervical ICA was successfully treated by deploying a carotid WallStent (Boston Scientific, Marlborough, Massachusetts, USA). A follow-up angiographic run through the guide catheter revealed a sub-occlusive thrombus in the cervical ICA distal to the stent. The clot was successfully removed with single pass of aspiration using the JET 7 XTRA Flex reperfusion catheter.
When the JET 7 XTRA Flex catheter was removed following the final pass, it was brought to the back table to be flushed. On gentle injection of saline through the catheter, a small segment in the distal end of the catheter ballooned and expanded, as shown in figure 1. Throughout the procedure, contrast had never been injected through the JET 7 XTRA Flex catheter, and no abnormalities were noted while manipulating the catheter during the previous two passes. On close inspection of the saved images postprocedurally, a subtle defect was observed in the wall of the JET 7 (figure 1) which corresponded with the point at which ballooning occurred. This defect was present during the first pass; however, it did not result in obvious malfunction until after the procedure had concluded.
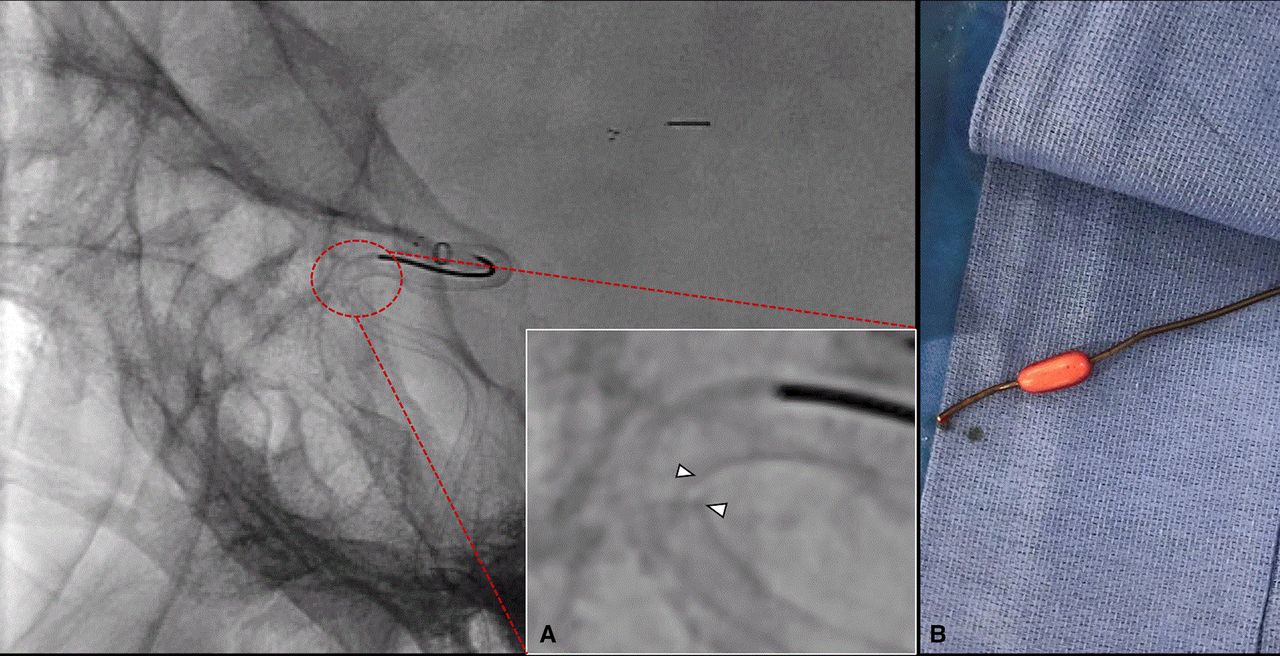
Lateral fluoroscopic view of the JET 7 XTRA Flex reperfusion catheter in the M1 segment of the right middle cerebral artery, with a fully expanded EmboTrap II stentriever. (A) Magnified view of the distal segment of the JET 7 catheter demonstrates a defect and tear in the wall of the catheter (arrowheads). (B) Expansion in the distal segment of the JET 7 XTRA Flex catheter with hand injection of heparinized saline.The site of expansion correlates with the area of wall defect.
Patient No 2
A patient in their 60s presented with altered mental status and left hemiplegia with an NIHSS score of 23. CTA showed right ICA terminus occlusion. The patient was outside the time window for intravenous recombinant tissue plasminogen activator. The patient was taken for emergent EVT.
An 8 F short sheath was placed and a Zoom 088 guide catheter (Imperative Care, Campbell, California, USA) was advanced over a 5 F VTK Selection catheter (Cook Medical, Bloomington, Indiana, USA) over a 038 glide wire (Terumo Medical Corp, Somerset, New Jersey, USA) into the thoracic descending aorta. The right ICA was selected, and the guide catheter was advanced into the cervical segment of the right ICA. The angiographic run through the guide catheter revealed a right ICA terminus occlusion.
The JET 7 XTRA Flex catheter over a Velocity microcatheter, over a Fathom 16 micro guidewire (Boston Scientific) was advanced into the guide catheter and further advanced until the JET 7 XTRA Flex reperfusion catheter faced the thrombus at the right ICA terminus. Using a combination of aspiration and stentretriever (4×30 mm Trevo, Stryker, Fremont, California, USA) techniques in three passes, the right MCA and its branches were recanalized but the A1 segment of the right anterior cerebral artery remained occluded.
An attempt was made to perform an angiographic run in preparation for thrombectomy of the right A1 occlusion. However, after hand injection of contrast via a 10 mL syringe through the JET 7 XTRA Flex catheter, expansion and forward jump of the distal segment of the catheter was noted, associated with supraclinoid ICA rupture and contrast extravasation into subarachnoid space (online supplemental video 1) (figure 2). A 7×7 mm Transform balloon was immediately prepared and advanced into the JET 7 XTRA Flex catheter to be inflated in the supraclinoid ICA to stop the bleeding. However, the distal end of the catheter was occluded and prevented advancing the Transform balloon catheter beyond the distal segment of the JET 7 catheter. Therefore, the decision was made to remove the JET 7 catheter but the distal end of the catheter was engaged and stuck outside the tip of the guide catheter, preventing catheter removal. The guide catheter and JET 7 aspiration catheter were removed together, and a new guide catheter was used to selectively catheterize the right ICA. Once done, an angiographic run was performed which showed complete occlusion of the distal right ICA without further contrast extravasation. Meanwhile, an external ventricular drainage was placed, and CT scan of the head revealed diffuse subarachnoid hemorrhage. The patient remained in a poor clinical condition with limited neurological examination for 3 days until the family made the decision to withdraw care.
Supplementary video
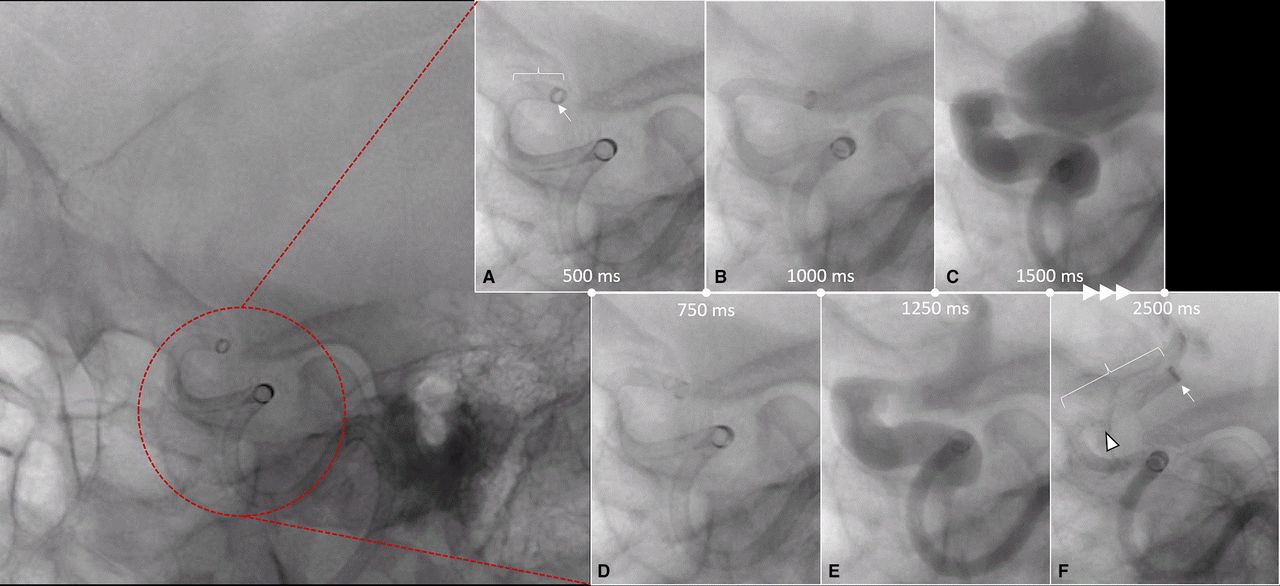
Lateral fluoroscopic view of the JET 7 XTRA Flex reperfusion catheter within the Zoom 88 guide catheter prior to hand injection of contrast. (A) Beginning of hand injection to (F) termination of the injection, demonstrates how the tip of the JET 7 catheter (arrow) moved forward during the injection. The brackets highlight elongation of the distal segment of the catheter during the injection, and the arrowhead shows the area of wall defect and irregularity in the JET 7 catheter.
Patient No 3
A patient in their 60 s presented with acute onset left sided hemiplegia and facial droop, with an NIHSS score of 18. The patient’s CT scan of head revealed an Alberta Stroke Program Early CT score of 7, and CTA showed a right M1 occlusion. The patient received intravenous recombinant tissue plasminogen activator and was taken for emergent EVT.
Right common femoral artery access was obtained, and an 8 F sheath was placed. A 6 F 90 cm Ballast guide sheath (Balt USA LCC, Irvine, California, USA) which was then navigated into the cervical pre-petrous right ICA. A JET 7 XTRA Flex reperfusion catheter with a Headway 021 microcatheter (MicroVention, Aliso Viejo, California, USA) and a Chikai 014 microwire (Asahi Inteco, Aichi, Japan) were then navigated coaxially through the Ballast catheter.
Using a combination of the Headway 021 microcatheter and a Chikai 014 microwire, the JET 7 XTRA Flex reperfusion catheter and Headway microcatheter were then navigated into the right M1–2 junction. The Headway 021 microcatheter was further advanced with a Chikai 014 wire into the right superior division of the M3, and a microcatheter angiogram was performed.
An Embotrap 5×33 stentriever (Neuravi/Cerenovus) was then loaded into the Headway microcatheter and deployed from the M2 to the M1 segment, and aspiration was applied to the JET 7 XTRA Flex reperfusion catheter at the M1 distal segment. After 3 min, the combination of the Embotrap stentriever and JET 7 XTRA Flex catheter was withdrawn to the right cavernous carotid artery, and then the Embotrap was completely removed through the JET 7 XTRA Flex catheter.
A follow-up angiographic run via the guide catheter showed partial filling of the M1 bifurcation with occlusion of the M2 (figure 3B). The Headway 021 microcatheter was then navigated into the superior division right M2 and the Embotrap 5×33 stentriever was deployed into the superior division of M2 to the M1 segment, followed by repeat aspiration via the JET 7 catheter in the M1 segment.
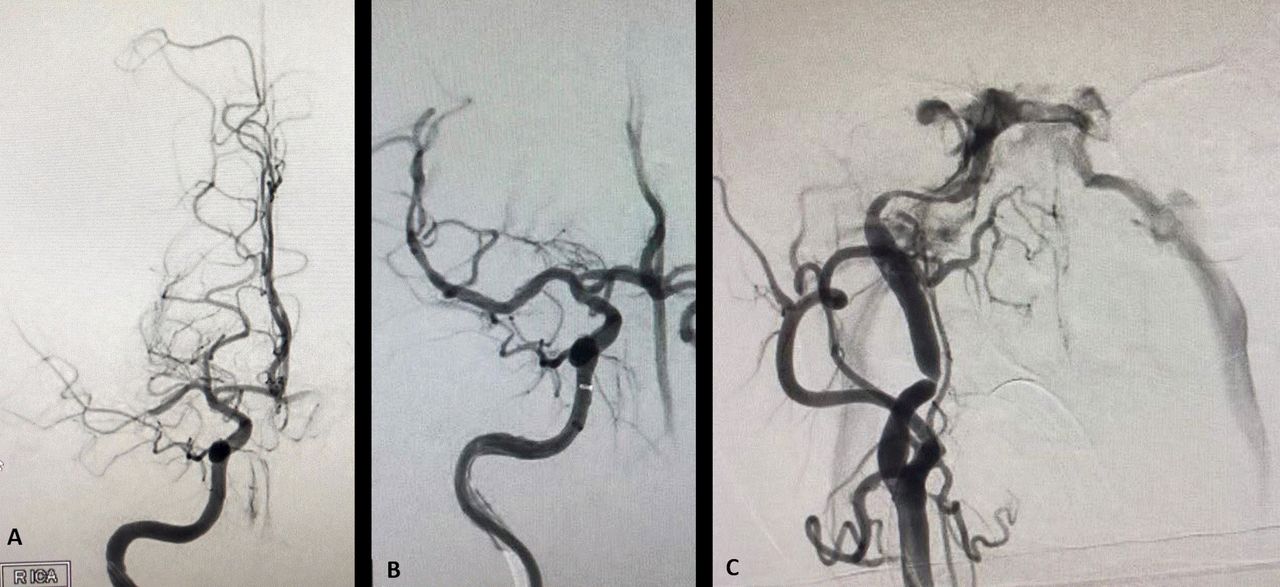
(A) Initial angiographic run demonstrates occlusion of the distal M1 segment of the right middle cerebral artery. (B) Post-thrombectomy angiographic run demonstrating complete recanalization of the M1 segment of the right middle cerebral artery. (C) Final angiographic run shows high flow carotid–cavernous fistula and no intracranial flow from the right internal carotid artery.
The combination was then withdrawn back into the JET 7 XTRA Flex reperfusion catheter in the M1 segment, and the JET 7 catheter was withdrawn back into the cavernous carotid artery where spontaneous flow occurred. The stentriever was removed and a follow-up angiographic run was performed via the JET 7 XTRA Flex catheter which initially demonstrated TICI 3 flow. The views were then magnified and collimated showing a high flow carotid–cavernous fistula and non-filling of the intracranial circulation (figure 3C).
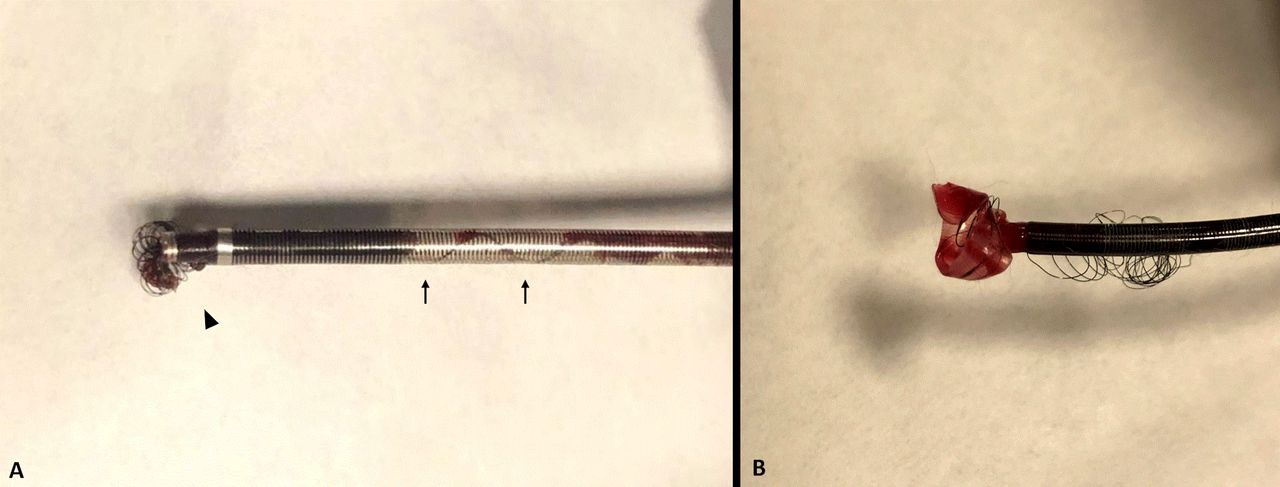
The JET 7 XTRA Flex catheter was then withdrawn into the Ballast guide catheter. However, under fluoroscopy, there appeared to be a retained tip of the JET 7 XTRA Flex catheter in the Ballast guide catheter. The combined Ballast and JET 7 XTRA Flex catheters were removed together. Catheter inspection demonstrated a breakdown of the distal assembly of the JET 7 XTRA Flex catheter with shearing of its tip, which was retained in the Ballast guide catheter (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Direct visualization of the JET 7 XTRA Flex reperfusion catheter. (A) The JET 7 catheter within the Ballast guide catheter; the arrowhead demonstrates the distorted distal tip of the catheter and the arrows show how the JET 7 catheter had stretched within the guide catheter. (B) Unwound, delaminated, and prolapsed distal tip of the JET 7 catheter outside the tip of the Ballast guide catheter.
Repeat access to the right common carotid artery and right ICA were then performed with a 4 F H1 catheter. There was evidence of a high flow right carotid–cavernous fistula and what appeared to be a subintimal dissection involving the petrous ICA. There was lack of flow through the right MCA branches due to the high flow fistula on a right sided injection. Selective catheterizations of the left common carotid artery and the left ICA were then performed with the 4 F H1 catheter. Cross filling was noted via the anterior communicating artery to the right MCA branches with partial filling of less than 50% of the right MCA branches, as well as retrograde filling through the anterior communicating artery to the distal MCA branches. The procedure was terminated without further intervention.
Postprocedurally, the patient remained intubated and sedated, and was transferred to the neurointensive care unit. One day later, the patient’s neurologic status deteriorated to an examination consistent with brain death, and care was withdrawn.
Discussion
EVT has revolutionized the management and outcome of acute ischemic stroke from emergent large vessel occlusion.7 Fast and complete reperfusion is the key for an optimal clinical outcome.8In recent years, successive introduction of large bore aspiration catheters has led to faster and robust reperfusion with improved outcome.4 These catheters offer a larger inner diameter and higher aspiration force and can be used in conjunction with stentriever or for direct aspiration.
The Penumbra JET 7 XTRA Flex reperfusion catheter, which was approved to be used for revascularization by the FDA in 2018, has a working length of 132 and distal inner diameter of 0.072 inches. Its 20 points of transitions from the proximal shaft to the distal tip and progressive distal coil wind provides enhanced trackability and flexibility. Initial experiences using this catheter for direct aspiration and in conjunction with stentrievers have been promising, with reports of shortened procedure times, high reperfusion rates, and a safety profile comparable with other devices.6 This is also similar to early observations in our institutions. However, with continued use of the catheter, a growing number of JET 7 XTRA Flex catheter malfunctions were observed. These malfunctions include break and tear in the distal segment of the catheter, ballooning of the distal segment of the catheter, and stretching of the tip of the catheter within the guide catheter while attempting to pull the catheter out. Most of these incidents were inconsequential, with no adverse impact on the patient’s outcome, similar to our patient No 1 reported here.
The cases presented in this report were from two independent high volume comprehensive stroke centers with more than 250 annual thrombectomy procedures. The cases were performed by two senior and one junior neurointerventional surgeons between 2018 and early 2020. The exact mechanism of these malfunctions is unclear. However, progressive coil wind in the distal portion of the catheter which enhances its flexibility could potentially account for easier expansion, tear, or rupture in this position of the catheter. In a recent report from Singapore, Pearly Ti et al 9 described two cases of JET 7 XTRA Flex catheter distal tip ballooning and malfunction following thrombectomy passes. In both cases, a stentriever was used in conjunction with the JET 7 catheter. However, in only case was the unsheathed stentriever pulled into the JET 7 catheter. This observation suggests that mechanisms other than direct damage to the wall of the catheter from friction between an expanded stentriever and the inner wall of the catheter must be involved in damaging the JET 7 catheter tip. We postulate that a disproportionately increased inner diameter of the catheter compared with its outer diameter has resulted in softer coating of the distal portion of the catheter, which is vulnerable to tear, stretch, and accordioning. This can occur from friction between the stentriever, microcatheter, or microwire and the JET 7 catheter inner wall or navigating and pulling catheter in a tortuous anatomy. The teared and stretched segment of the catheter will be ballooning and expanded if contrast/heparinized saline is injected through the catheter.
Similar combinations of guide catheters, microcatheters, and microwires with numerous other aspiration catheters, including the Penumbra ACE 68 reperfusion catheter, have been routinely used in our institutions but we have not observed this malfunction with other aspiration catheters. Review of the United States FDA Manufacturer and User Facility Device Experience (MAUDE) database10 revealed 218 discreet incidents of JET 7 XTRA Flex reperfusion catheter malfunction, not including the cases mentioned in this report. Twelve of these malfunctions resulted in significant intracranial vessel injury and/or patient death, and all 12 cases involved fracture, delamination, and/or ballooning/expansion of the JET 7 distal catheter tip.
Following a growing number of reports on the adverse events and device malfunctions related to the JET 7 XTRA Flex reperfusion catheter, the Penumbra released a statement in July 2020, cautioning against direct contrast injection into the catheter during the procedure.11 The notification warns against contrast injection through the JET 7 XTRA Flex catheter either using manual syringe injection or automated high pressure injection due to the risk of expansion or rupture of the distal end of the catheter which can potentially result in vessel wall injury. The statement highlights that the safety and compatibility of using the JET 7 XTRA Flex catheter in combination with thrombectomy devices from other manufacturers has not been tested. As newer generations of stroke intervention devices are being consecutively introduced to the market, they should be vigorously checked for safety by neurointerventional surgeons in different situations as they are being used in various thrombectomy techniques and in combination with devices sometimes from different manufacturers. We specifically recommend checking the integrity and functionality of the aspiration catheters after each thrombectomy pass before deciding on reintroducing them into the patient’s body. It is also our responsibility to ascertain that the devices are being used in accordance with the manufacturer’s recommendations and warning reflected on the device indication for use.
Endovascular thrombectomy devices are being rapidly evolved and refined, which has resulted in continued improvement in achieving fast and robust reperfusion and better clinical outcome. However, it is our responsibility, as the neurointerventional community, to be vigilant in identifying patient harm events, reporting them, and taking action to prevent future adverse events. This will provide the device manufacturers with essential feedback in implementing relevant modifications in their products to enhance the safety while maintaining high efficacy.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @rdeleacymd
Contributors All authors contributed to the conception and drafting of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.