Article Text

Abstract
Background Collateral flow (CF) is an effective predictor of outcome in acute ischemic stroke (AIS) with potential to sustain the ischemic penumbra. However, the clinical prognostic value of CF in patients with AIS undergoing mechanical thrombectomy has not been clearly established. We evaluated the relationship of CF with clinical outcomes in patients with large artery anterior circulation AIS treated with mechanical thrombectomy.
Methods Baseline collaterals of patients with AIS (n=135) undergoing mechanical thrombectomy were independently evaluated by CT angiography (CTA) and conventional angiography and dichotomized into poor and good CF. Multivariable analyses were performed to evaluate the predictive effect of CF on outcome and the effect of time to reperfusion on outcome based on adequacy of the collaterals.
Results Evaluation of CF was consistent by both CTA and conventional angiography (p<0.0001). A higher rate of patients with good collaterals had good functional outcome at 3-month follow-up compared with those with poor collaterals (modified Rankin Scale (mRS) 0–2: 60% vs 10%, p=0.0001). Patients with poor collaterals had a significantly higher mortality rate (mRS 6: 45% vs 8%, p=0.0001). Multivariable analyses showed that CF was the strongest predictor of outcome. Time to reperfusion had a clear effect on favorable outcome (mRS ≤2) in patients with good collaterals; in patients with poor collaterals this effect was only seen when mRS ≤3 was considered an acceptable outcome.
Conclusions CTA is a valid tool for assessing the ability of CF to predict clinical outcome in patients with AIS treated with mechanical thrombectomy. Limiting time to reperfusion is of definite value in patients with good collaterals and also to some extent in those with poor collaterals.
- Stroke
- Thrombectomy
- CT Angiography
Statistics from Altmetric.com
Introduction
The efficiency of collateral circulation downstream of an arterial occlusion has been shown to be a major determinant of clinical outcome in patients with acute ischemic stroke (AIS).1–3 The severity of ischemia could be offset by collateral circulation with consequent limitation of tissue injury and clinical impairment.2 High rates of recanalization achieved by endovascular treatment (ET) do not unequivocally translate into favorable clinical outcomes, especially when collaterals are poor.3 In view of this, careful patient selection for ET is desirable and should focus on multimodal neuroimaging in addition to onset time and severity of stroke.4 This concept has been successfully adopted in recent randomized clinical trials of ET such as ESCAPE5 and EXTEND-IA.6
Different grading systems based on different imaging methods have been used to score the adequacy of intracranial collateral flow (CF).7 Despite this heterogeneity, conventional angiography (CA) still represents the gold standard for evaluation of collaterals due to its maximal temporal and spatial resolution.7 However, CA is invasive and is not yet widespread. CT angiography (CTA) offers a valid and feasible tool for the assessment of collaterals since its predictive value has been confirmed with different scoring systems.8 As a consequence, in high-volume stroke centers it is increasingly becoming the earliest examination for the assessment of angiographic status in patients with AIS. Our aim was to evaluate concordance between CTA and CA in the evaluation of collaterals and to determine the relationship with clinical outcomes.
Methods
We evaluated baseline non-contrast CT (NCT) of the head, CTA of the head and neck, and CA of extracranial and intracranial arteries of patients with M1 segment middle cerebral artery (MCA) occlusion with or without internal carotid artery (ICA) occlusion. Based on a predefined treatment algorithm, patients were treated by thrombectomy preceded or not by IV thrombolysis (IVT) at full standard dose (ie, 0.9 mg/kg) of alteplase.9 CF was independently evaluated by CTA and CA. For assessment of collateral status on CTA we adopted a scale from 0 to 3 derived from the Prolyse in Acute Cerebral Thromboembolism (PROACT) II trial10 (0: no collaterals; 1: collaterals to the periphery of ischemia; 2: collaterals filling 50–100% of ischemic area; 3: collaterals filling 100% of ischemic area). For assessment of CF on CA we used the grading system proposed by Christoforidis et al11 based on five decreasing levels of retrograde contrast opacification of vessels within the occluded territory on delayed angiograms. Since CA is currently considered the gold standard for assessment of collaterals,12 patients were dichotomized into poor3–5 and good1 ,2 based on the CA collateral score. Stroke severity was assessed by the National Institutes of Health Stroke Scale (NIHSS) at baseline and 24 hours after onset. Functional outcome at 3 months was evaluated by the modified Rankin Scale (mRS) score, with mRS ≤2 considered a favorable outcome. The Thrombolysis in Cerebral Ischemia (TICI) score was used for angiographic outcome, with successful reperfusion defined as TICI ≥2b on the final angiogram. Intracranial hemorrhage was defined as symptomatic intracranial hemorrhage (sICH) in cases with a 4-point increase in the NIHSS score.13 The study was approved by the local ethical committee and informed consent was obtained from all patients or their relatives.
Imaging acquisition
NCT and CTA were acquired using a standardized protocol. Axial CT was performed on a multislice scanner (GE Medical Systems) using 120 Kv, 170 mAs with 5 mm slice thickness. Continuous axial slices parallel to the orbitomeatal line were obtained from the skull base to the vertex. CTA was then performed using a 64-row detector. Acquisitions were obtained after a single bolus IV contrast injection of 90–120 mL non-ionic contrast media into an antecubital vein at 3–5 mL/s. Source images were reconstructed at 1.25 mm thickness in axial planes at half-thickness intervals. Before thrombectomy, in order to evaluate collaterals, an ipsilateral angiogram was acquired in case of ICA patency whereas a contralateral angiogram was performed in case of ICA occlusion. NCT was repeated 24 hours after stroke onset.
NCT, CTA, and CA scans were independently reviewed by a neuroradiologist (DK) and a stroke neurologist (GK) who were blinded to the patients' symptoms but aware of acute non-lacunar stroke. NCT was screened for Alberta Stroke Program in Early CT Score (ASPECTS) before treatment and 24 hours after stroke onset.14
Statistical analysis
Descriptive statistics consisted of means±SD or medians with IQR for parameters with Gaussian distributions (after confirmation with histograms and the Kolmogorov-Smirnov test) or frequencies (%) as appropriate. Inter-rater reliability was calculated using the interclass correlation coefficient (ICC) (two-way, single measures, absolute agreement). Comparison of continuous variables was performed by means of a Student's t-test or Mann-Whitney U test. Comparison of categorical variables was performed with a Fisher's exact test.
Spearman correlation analysis was performed for the evaluation of consistency between scores obtained by different methods (CTA and CA). Multivariable regression analysis was performed to identify the effect of CF status on predicting a good outcome after adjustment for age, baseline NIHSS score, presence of ICA-M1 tandem occlusion, time to reperfusion, and post-treatment reperfusion grade (TICI ≥2b). Moreover, distinct logistic regression analyses were performed to evaluate the effect of time to reperfusion on the probability of a favorable outcome separately in patients with poor collaterals (P-CF) and those with good collaterals (G-CF). A p value of <0.05 was considered statistically significant.
Results
The inter-rater reliability was 0.71 for CTA and 0.76 for CA collateral status, indicating a good inter-rater agreement for the two methods. Among 162 patients with anterior circulation stroke treated between February 2010 and October 2015, 135 had complete CA, CTA, and clinical data and were included in the final analysis. After CF status dichotomization based on CA results, there were 75/135 (55%) patients in the G-CF group and 60/135 (45%) in the P-CF group. Successful recanalization was achieved in 88/135 (65.1%) and good clinical outcome in 51/135 (37.7%). Patients in the G-CF group had lower NIHSS, higher NCT ASPECTS at baseline, and a lower rate of tandem occlusion than those in the P-CF group (table 1).
Baseline characteristics of patients stratified by collaterals on CA (n=135)
Spearman coefficient correlation (r) between CTA and CA in the assessment of CF was 0.60 (p<0.0001), indicating high consistency between the two methods. mRS scores at 3 months were significantly correlated with CF grade evaluated by both CTA (r=0.50, p<0.0001) and CA (r=0.51, p<0.0001). Multivariable-adjusted analysis including CF status, age, baseline NIHSS score, presence of ICA-M1 tandem occlusion, time to reperfusion, and post-treatment reperfusion grade (TICI ≥2b) revealed an association between functional outcome (mRS ≤2) and efficiency of CF (OR 2.13; 95% CI 1.44 to 3.15; p<0.001) as well as time to reperfusion (OR 1.008; 95% CI 1.00 to 1.01; p=0.013) and patient age (OR 1.04; 95% CI 1.00 to 1.09; p=0.014) (see online supplementary file 1).
supplementary file 1
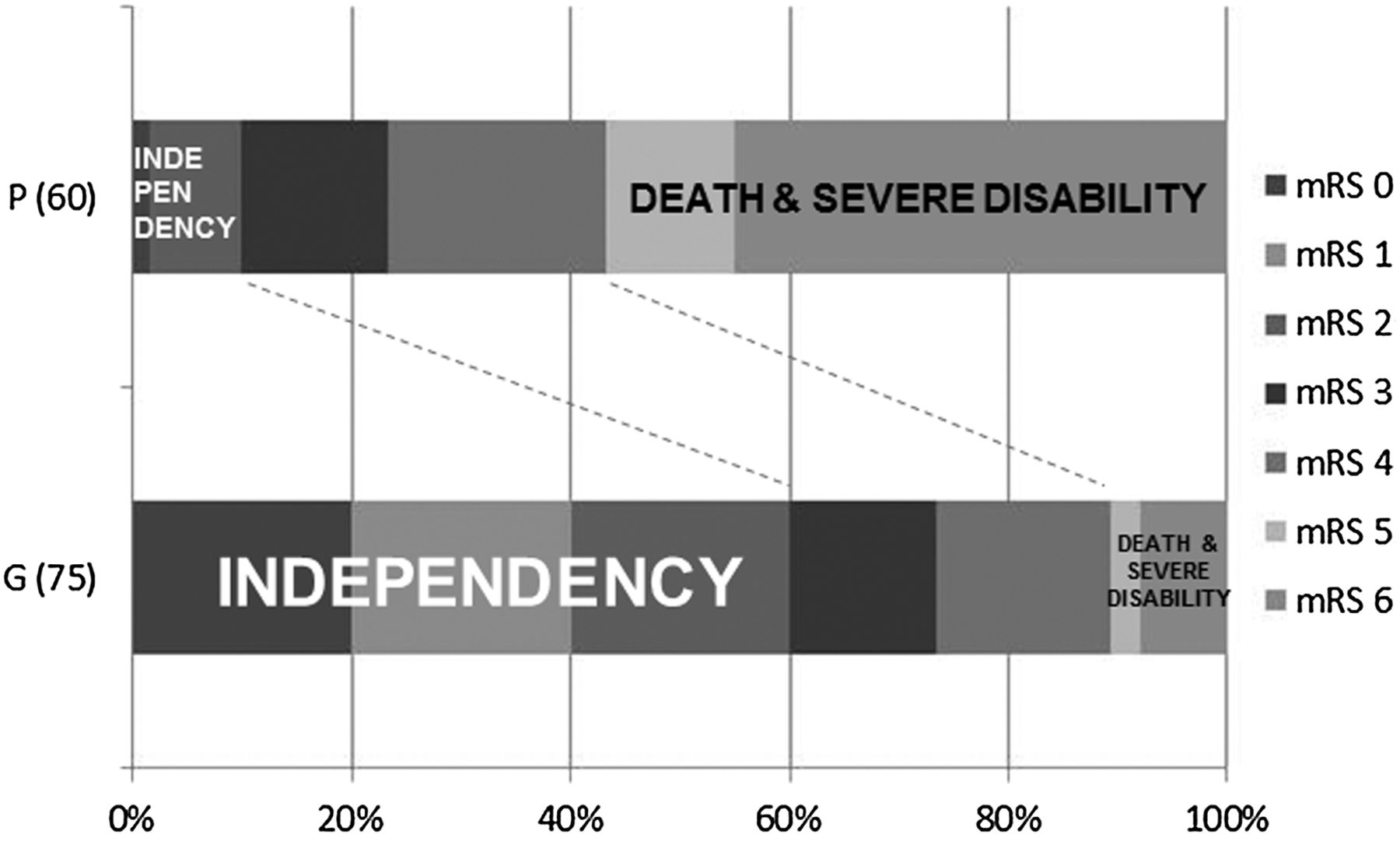
Patients in the G-CF group had a higher rate of good functional outcome at 3-month follow-up than those in the P-CF group (mRS 0–2: 60.1% vs 10.2%, p=0.0001; mRS 0–3: 73.3% vs 23.3%; p=0.0001). Patients in the P-CF group had a higher mortality rate than those in the G-CF group (mRS 6: 8% vs 45%, p=0.0001) and, even when considering the rate of combined outcome of death plus severe disability (mRS 5 and 6), a higher rate of patients was found in the P-CF group than in the G-CF group (10.6% vs 56.6%, p=0.0001). All the above mentioned data are shown in figure 1. Patients in the G-CF group had a lower rate of sICH (6.6% vs 36.6%; p=0.0001), higher 24-hour ASPECTS (5.2±2.5 vs 1.6±1.7; p=0.0001), a higher rate of 24-hour NIHSS 4-point improvement (69.3% vs 15%; p=0.0001) with a higher median 24-hour difference in NIHSS (−6 (IQR −12 to −2) vs 2 (IQR 0–5.75); p=0.0001), a higher rate of successful recanalization (73.3% vs 55%; p=0.03), and a lower median number of device passages during the endovascular procedure (2 (IQR 1–3) vs 3 (IQR 1–4); p=0.03) (see online supplementary file 2).

Scores on the modified Rankin Scale (mRS) at 3 months in good (G) and poor (P) collateral flow groups stratified on conventional angiography.
supplementary file
In a further analysis we evaluated the relationship between time to reperfusion and clinical outcome stratified by CF status. The probability of an unfavorable outcome (mRS >2) increased with every minute increase of time to reperfusion in the G-CF group (OR 1.01; 95% CI 1.00 to 1.01; p=0.017). In particular, the probability of an unfavorable outcome (mRS >2) was 51% for a time to reperfusion of 360 min, falling to 28% for a time of 240 min (figure 2A). The effect of time on the probability of a favorable outcome in the P-CF group was not statistically significant (OR 1.02; 95% CI 0.99 to 1.04; p=0.082); however, the probability of a poor outcome fell from 98% for a time to reperfusion of 360 min to 85% for a time of 240 min, still emphasizing the importance of speeding up the time to reperfusion (figure 2B). Even after adjustment for age, post-treatment reperfusion grade (TICI ≥2b) and baseline NIHSS, time to reperfusion still remained a significant predictor of good outcome (mRS ≤2) in the G-CF group (OR 1.00; 95% CI 1.00 to 1.01; p=0.022) but not in the P-CF group (OR 1.01; 95% CI 0.99 to 1.03; p=0.128). However, when we analyzed the probability of a favorable outcome considered up to slight disability (mRS ≤3) in the P-CF group, we found that time to reperfusion was associated with functional outcome at equal values of age, baseline NIHSS, and reperfusion grade (TICI ≥2b) (see online supplementary file 3).
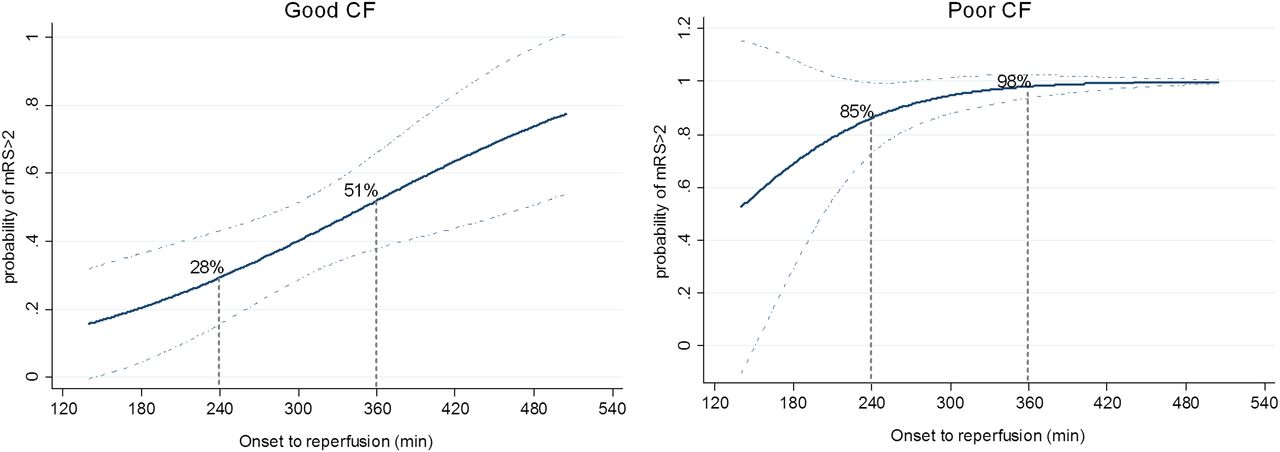
Unadjusted predicted probability of 3-month poor outcome (modified Rankin Scale (mRS) >2) by time to reperfusion. Solid lines represent the probability of an unfavorable outcome over onset to reperfusion time in (A) the good collateral flow group and (B) the poor collateral flow group. Dashed lines show the 95% CI.
supplementary file
As shown in figure 3, the probability of an unfavorable outcome (mRS >3) at 3 months was 88% for a time to reperfusion of 360 min, falling to 68% for a time of 240 min, confirming the relevance of speeding up the diagnostic and therapeutic processes even in a condition of poor sustenance of ischemic penumbra.

{kind=link}
{kind=link}
{kind=link}
Unadjusted predicted probability of 3-month poor outcome (modified Rankin Scale (mRS) >3) by time to reperfusion in the poor collateral flow group. The solid line shows the probability of an unfavorable outcome over onset to reperfusion time in the poor collateral flow group.
Discussion
Currently, selection of the ideal candidate for reperfusion therapy represents one of the most debated issues in endovascular stroke treatment research. Beyond symptom onset time, neuroimaging seems to be the key to better define prognosis and offer useful information in the very early stage of AIS.5 ,6 The EXTEND-IA and ESCAPE trials selected patients for ET based on CT perfusion and CTA evaluation of collaterals, respectively. However, these strict criteria entail exclusion of a large proportion of patients with unfavorable imaging traits presenting in the therapeutic time window. As a consequence, most of the conclusions from these trials are not relevant to clinical practice where onset to presentation time still plays (or should play) a pivotal role. Compared with other neuroimaging parameters such as ischemic penumbra, collaterals are easy to detect and are directly related to perfusion status in patients with AIS.15 It has already been shown that good collaterals are related to larger areas of benign oligemia whereas poor collaterals are related to larger areas of mismatch.15 In line with this ability in the sustenance of penumbral tissue, previous studies have shown that collaterals allow extension of the therapeutic time window with a favorable outcome being strictly related to adequacy of the collaterals in a time-dependent manner.16
Although CA remains the gold standard for the assessment of collaterals, our study demonstrates that CTA has a strong ability in reliably defining CF adequacy, with a strong correlation with CA findings and outcome at 3 months. This confirms the recent results from the ESCAPE trial.5 Compared with CA, CTA has some advantages including being performed as the first examination in the very early phase of the acute incident prior to IVT, having a short acquisition time, giving simultaneous information about all four vessels, and having an established ability to provide information on tissue level perfusion and the prediction of final infarct size using the CTA source images (CTA-SI).17 ,18 For all these characteristics and for the findings of our study, we propose CTA as the ideal tool in the acute setting for the assessment of CF. As in previous studies, we have shown that, regardless of angiographic results after ET, G-CF is a strong predictor of independence and slight disability at 3-month follow-up and P-CF is a strong predictor of death and severe disability. It is worth drawing attention to the high rate of sICH in our P-CF group (36%). This is in line with a previous report suggesting an association between ASPECTS and the risk of sICH.19 However, in a similar sample of patients with stroke treated with ET stratified by collaterals, Bang et al20 found a rate of sICH of 30% in patients with poor collaterals. Furthermore, compared with the abovementioned study, the baseline NIHSS of our P-CF group was higher and the use of IVT before mechanical thrombectomy almost double, suggesting a higher risk of ICH in our population study.
Contrary to the findings of Hwang et al,21 we found a marked effect of time to reperfusion on the 3-month outcome in the G-CF group, with a relevant increase in the chance of a good outcome when the time to reperfusion was shortened from 6 to 4 hours. However, similar to their results, we also found an effect of time to reperfusion in the P-CF group, though to a lesser extent, with a reasonable increase in the chance of slight disability (mRS ≤3) for a time to reperfusion of 4 hours. Our results therefore suggest, on the one hand, the relevance of evaluating the adequacy of the collaterals before treatment and, on the other hand, the importance of limiting time to reperfusion also in patients with poor CF. In line with this and the concepts discussed above, CF adequacy reflects both infarct size (ASPECTS) and perfusion status, which are linked to the potential of therapeutic time window extension, the risk of hemorrhagic complications, and outcomes.15–18 CT perfusion imaging, which was not part of our study protocol, would have been critical to clarify these aspects.22
Our study has some limitations. ET included different approaches (eg, stentrievers, thromboaspiration devices) that were not balanced across the groups. Another limitation is the relatively small sample size. Despite these limitations, after dichotomization of CF the difference in favorable and unfavorable outcomes between the two groups was definitely considerable. Our recanalization rate of 65.1% could be considered low compared with current standards, affecting the rate of functional independence at 90 days. Some of the factors that could have influenced our rate of recanalization are the long study period analysed (more than 5 years) including also the use of first-generation thromboaspiration devices, and the high rate of tandem occlusion included in this analysis (43%), which is much higher than that of the MR CLEAN trial (29%).23 However, although the effect of reperfusion grade on outcome was not specifically the purpose of our study, it is important to emphasize that our recanalization rate was higher than that of the MR CLEAN trial21 and the Interventional Management of Stroke (IMS) III trial.24
Conclusions
Our study showed that (1) CTA correlates very well with CA in the assessment of CF; (2) patients with poor collaterals have a high mortality rate and a low rate of favorable outcome whereas those with good collaterals have a low mortality rate and a high rate of favorable outcome; (3) CF has been shown to be the strongest predictor of outcome; (4) shortening time to reperfusion is of significant value in G-CF patients and also, to a lesser extent, in P-CF patients. Therefore, in our view, insufficient CF is not a contraindication to ET if a reasonable time to reperfusion is achievable.
Overall, CTA-based CF together with time to reperfusion accurately predict outcome in patients with large artery occlusion of the anterior circulation.
References
Footnotes
Contributors FS: study concept/design; analysis/interpretation of data; acquisition of data; study supervision/coordination; obtaining funding; drafting/revising the manuscript for content. CM: analysis/interpretation of data; drafting/revising the manuscript for content; statistical analysis; obtaining funding; study supervision/coordination. SP: study concept/design; acquisition of data. MD: analysis/interpretation of data; drafting/revising the manuscript for content. AG: analysis/interpretation of data; acquisition of data. VCD: analysis/interpretation of data; acquisition of data. DS: analysis/interpretation of data; acquisition of data. SM: study concept/design; acquisition of data; analysis/interpretation of data. VS: statistical analysis; analysis/interpretation of data. JML: study concept/design; acquisition of data. DK: analysis/interpretation of data; acquisition of data. EP: analysis/interpretation of data; acquisition of data. RF: analysis/interpretation of data; drafting/revising the manuscript for content; study supervision/coordination. PS: study concept/design; drafting/revising the manuscript for content; obtaining funding. RG: analysis/interpretation of data; drafting/revising the manuscript for content, acquisition of data. GK: study concept/design; drafting/revising the manuscript for content; obtaining funding; study supervision/coordination; acquisition of data.
Funding This work was supported by Italian Ministry of Health grant number RF-2013–02358679.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Ethics approval was obtained from the local ethics committee.
Provenance and peer review Not commissioned; externally peer reviewed.