Article Text

Abstract
OBJECTIVE White matter lesions are often seen on MR scans of elderly non-demented and demented people. They are attributed to degenerative changes of small vessels and are implicated in the pathogenesis of cognitive decline and dementia. There is evidence that especially periventricular white matter lesions are related to cognitive decline, whereas subcortical white matter lesions may be related to late onset depression. The frequency distribution of subcortical and periventricular white matter lesions according to age and sex reported.
METHODS A total of 1077 subjects aged between 60–90 years were randomly sampled from the general population. All subjects underwent 1.5T MR scanning; white matter lesions were rated separately for the subcortical region and the periventricular region.
RESULTS Of all subjects 8% were completely free of subcortical white matter lesions, 20% had no periventricular white matter lesions, and 5% had no white matter lesions in either of these locations. The proportion with white matter lesions increased with age, similarly for men and women. Women tended to have more subcortical white matter lesions than men (total volume 1.45 ml v 1.29 ml; p=0.33), mainly caused by marked differences in the frontal white matter lesion volume (0.89 ml v 0.70 ml; p=0.08). Periventricular white matter lesions were also more frequent among women than men (mean grade 2.5 v 2.3; p=0.07). Also severe degrees of subcortical white matter lesions were more common in women than in men (OR 1.1; 95% confidence interval (95% CI) 0.8–1.5) and periventricular white matter lesions (OR 1.2; 95% CI 0.9–1.7), albeit that none of these findings were statistically significant.
CONCLUSIONS The prevalence and the degree of cerebral white matter lesions increased with age. Women tended to have a higher degree of white matter lesions than men. This may underlie the finding of a higher incidence of dementia in women than in men, particularly at later age.
- white matter lesions
- prevalence
- magnetic resonance imaging
- population based
Statistics from Altmetric.com
White matter lesions are often found on MR scans of elderly people, they are attributed to degenerative changes of long penetrating arteries.1-6 Reported prevalence ranges from 5% to 90%, depending on study design, study population, and rating scales.1-3 7-10 There is evidence that periventricular white matter lesions are especially related to cognitive decline,11 whereas subcortical white matter lesions may be related to late onset depression.12 White matter lesions can be divided into those in the subcortical and those in the periventricular region. Only a few studies considered lesions in these regions separately,13-15 but some based their analysis on a summary score of subcortical and periventricular white matter lesions,15 as in other studies.1-3Although it is well established that the prevalence of white matter lesions increases with age, little is known about site specific frequency, including possible differences between the subcortical and periventricular region and the lobar location of the lesions. This distinction may be of potential interest as the subcortical and periventricular white matter lesions might have a different pathogenesis and may result in different cognitive or motor consequences. Some studies reported a higher prevalence of white matter lesions among women then men.1-3 The differences were, however, not statistically significant, and were only reported for total white matter lesions.
From a population based sample of subjects over 60 years of age, we report the age and sex specific frequency distribution of either type of white matter lesions by lobar location.
Methods
STUDY POPULATION
The Rotterdam Scan Study was designed to study determinants and cognitive consequences of age related brain abnormalities in elderly people. In 1995–6, 1904 normal healthy subjects aged between 60–90 years were randomly selected in strata of age (5 years) and sex from two large ongoing prospective follow up cohort studies, the Zoetermeer Study and the Rotterdam Study. Both studies have been described in detail elsewhere.16 17 In short, the Zoetermeer Study is a prospective population based study among 10 361 subjects, aged between 5–91 years at baseline, which studies determinants of chronic diseases. The Rotterdam Study is a population based prospective cohort study, among 7983 elderly subjects aged 55 years and over, which studies determinants of neurological, cardiovascular, locomotor, and ophthalmological diseases in elderly people.
For the Rotterdam Scan Study subjects were invited by a letter, and subsequently contacted by telephone. On agreement to participate a list of contraindications was reviewed to assess eligibility (dementia; blindness; or presence of standard MRI contraindications). From 1904 invited subjects 1717 were eligible. Complete information was obtained, including a cerebral MR scan, from 1077 persons (response rate 63%; 563 from the Rotterdam Study and 514 from the Zoetermeer Study). Each participant signed an informed consent form. The study was approved by the medical ethics committee of Erasmus University Rotterdam, The Netherlands.
CONFOUNDING VARIABLES
Blood pressure was measured twice on the right arm in a sitting position, by means of a random zero sphygmomanometer. The average of these two measurements was used. Hypertension was defined as a systolic blood pressure of ⩾160 mm Hg and/or a diastolic blood pressure of ⩾95 mm Hg or the self reported use of blood pressure lowering drugs. The ankle to brachial index was used as an indicator of atherosclerosis and was assessed by taking the ratio of the systolic blood pressure measured at the tibial artery to the systolic blood pressure measured at the right arm with a random zero sphygmomanometer, in a sitting position. Information on diabetes mellitus was obtained with the use of a standardised questionnaire, which was checked by a physician during the interview. Diabetes mellitus was considered present if the participant was taking oral antidiabetics or insulin.
MR SCANNING PROTOCOL
In all participants an axial T1, T2, and proton density (PD) weighted cerebral MR scan was made on a 1.5T MR scan. Subjects recruited from the Zoetermeer Study were scanned with a 1.5T MR Gyroscan (Philips, Best, The Netherlands) and participants from the Rotterdam Study were scanned with a 1.5T MR VISION (Siemens, Erlangen, Germany). To provide comparability the following pulse sequences were applied: at the Gyroscan T1 (TR 485 ms, TE 14 ms), T2 (TR 2236, TE 90 ms) and PD (TR 2236 ms, TE 20 ms); and at the VISION: T1 (TR 700 ms, TE 14 ms), T2 (TR 2200 ms, TE 80 ms) and PD (TR 2200 ms, TE 20 ms) Slice thickness was 6 mm and 5 mm respectively, with an interslice gap of 20.0%. The images were printed on hard copy with a reduction factor of 2.7.
WHITE MATTER LESIONS RATING SCALE
White matter lesions were considered present if these were hyperintense on both PD and T2 weighted images and not hypointense on T1 weighted images. White matter lesions were classified into those in the subcortical and periventricular region.11 The number and size of subcortical white matter lesions was rated on hard copy according to the largest diameter of one lesion within all slices in which the lesion could be seen in categories of small (<3 mm), medium (3–10 mm), or large lesions (>10 mm). To calculate the volume of subcortical white matter lesions on hard copy, they were considered to be spherical with a fixed diameter per size category (range 0–29.5 ml). Periventricular white matter lesions were rated semiquantitatively per region: adjacent to frontal horn (frontal capping), adjacent to lateral wall of lateral ventricles (bands), and adjacent to occipital horn (occipital capping) on a scale of 0 (no white matter lesions), 1 (pencil thin periventricular lining), 2 (smooth halo or thick lining), or 3 (large confluent white matter lesions). This was done for both hemispheres simultaneously. The overall degree of periventricular white matter lesions was calculated by adding up the scores for the three separate categories (range 0–9). White matter lesions could be rated for all subjects except in two in whom the quality of the MR scan did not allow reliable rating of the subcortical white matter lesions. All MR scans were examined by two raters who were blinded to age, sex, and other risk factors for white lesions. In case of a disagreement of more than one point, a consensus reading was held; in all other cases the readings of both readers were averaged. The interrater and intrarater studies showed a good to excellent agreement. For grading the periventricular white matter κ values were calculated by taking into account the difference between the scores of the two raters. These so called weighted κ values were between 0.79–0.90. For total subcortical white matter volume the interrater and intrarater intraclass correlation coefficient was 0.88 and 0.95, respectively.
STATISTICAL ANALYSIS
The prevalence of white matter lesions was defined as the presence of any white matter lesion (regardless of size or location) in the brain. The relation between the prevalence of white matter lesions and age was assessed by means of age and sex adjusted linear regression analyses. The frequency distribution of either type of white matter lesions was calculated by 10 years age strata (60–70, 70–80, and 80–90 years). The relation between sex and white matter lesions was assessed by means of age adjusted linear regression with white matter lesions as the dependent variable. Analysis of covariance (ANCOVA) was performed to obtain sex specific mean volume of subcortical white matter lesions per 10 year age stratum or the mean grade of the periventricular white matter lesions. Sex differences for each category (0, 1, 2, and 3) of periventricular white matter lesions per region, were analyzed with the χ2 test. There is increasing evidence that there exists a dose dependent relation between severity of white matter lesions and cognitive consequences.1 2and that especially the presence of severe white matter lesions is associated with a reduced cognitive function.11 18 We therefore separately analyzed severe subcortical and periventricular white matter lesions for each sex by means of an age adjusted logistic regression model. White matter lesions were dichotomised at the upper quintile of their distribution, which reflects severe white matter lesions. The associations are presented as odds ratios with a 95% confidence interval (OR; 95%CI).
Results
The overall response rate was 63%; it decreased with age from 73% in subjects aged between 60–70 years to 48% in participants aged between 80–90 years. Responders were therefore significantly younger than non-responders (mean age 72.4 yearsv 75.9 years, p<0.001), whereas there was no sex difference.
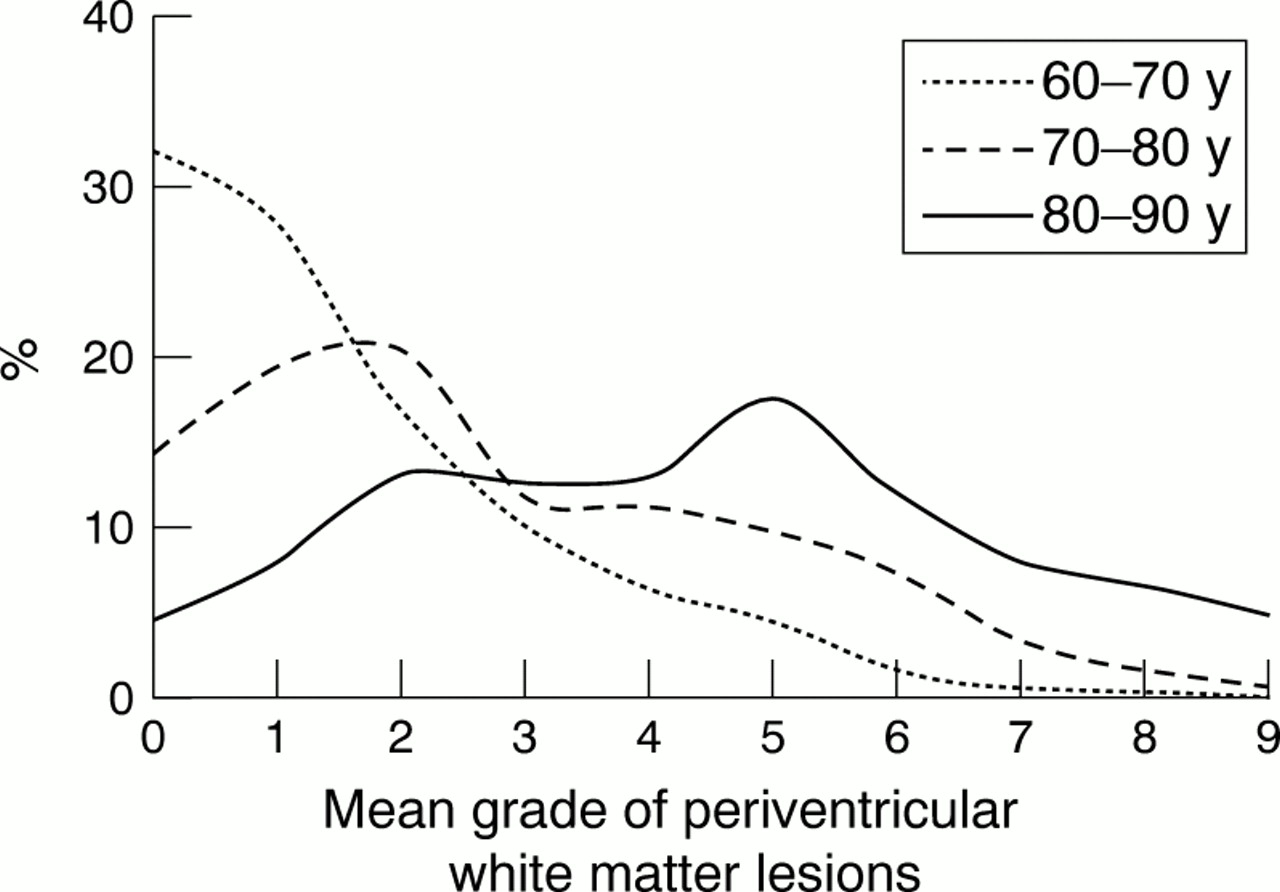
In our study 8% of all subjects were completely free of subcortical white matter lesions, 20% had no periventricular white matter lesions and 5% had no white matter lesions in either of these locations. Frequency distribution of white matter lesions at both locations strongly depended on age (figs 1 and 2). Of subjects aged between 60–70 years, about 13% were completely free of subcortical white matter lesions and 32% were free of periventricular matter lesions, whereas for subjects aged between 80–90 years these percentages were 0 and 5, respectively. The relation between age and the prevalence of white matter lesions was similar for men and women. The prevalence of subcortical and periventricular white matter lesions significantly increased, by 0.2% and 0.4% per year, respectively. Possible confounding variables including hypertension, diabetes, and indicators of atherosclerosis were equally distributed between men and women. Adjustment for these factors did not alter the magnitude of the associations presented below.

Distribution of subcortical white matter lesions by 10 year age category.
{kind=link}
{kind=link}
Distribution of periventricular white matter lesions by 10 year age category.
Table 1 shows the volume of subcortical white matter lesions/10 year age stratum by sex. The mean volume of subcortical white matter lesions was highest in the frontal lobe, followed by the parietal, occipital, and temporal lobes. This applied to both sexes and all age groups. The mean volume of subcortical white matter lesions increased from 0.6 ml (SE 0.1) for subjects between 60–70 years of age to 3.2 ml (SE 0.4) for subjects aged between 80–90 years (p<0.01). Women had greater volumes of subcortical white matter lesions than men (total volume 1.45 ml v 1.29), mainly caused by differences in the volume of frontal white matter lesions (0.89 mlv 0.70), but these differences were not significant (p=0.33 and p=0.08, respectively).
Mean volume (ml) of subcortical white matter lesions/lobar location/10 y age stratum1-151
Table 2 shows sex specific mean grades of periventricular white matter lesions/10 year category. The mean grade of periventricular white matter lesions increased from 1.5 (SE 0.1) for subjects between 60–70 years of age to 2.4 (SE 0.1) for subjects aged between 80–90 years (p<0.01). The mean grade of the total periventricular white matter lesions was non-significantly higher among women than men (2.5 (SE 0.1)v 2.3 (SE 0.1); p=0.07), mainly caused by the significant difference in severity of frontal capping between men and women in all age categories.
Sex specific mean grade of periventricular white matter lesions/ region/10 y age stratum2-151
Table 3 shows the proportion of subjects with different degrees of periventricular white matter lesions for each of the three different locations per 10 year age stratum. For all age categories and at every location, proportionally more women than men had the most severe periventricular white matter lesions.
Sex specific frequency distribution of periventricular white matter lesions grades/ region/10 y age stratum
Women had more severe periventricular (OR 1.2; 95% CI 0.9–1.7) and subcortical white matter lesions (OR 1.1; 95% CI 0.8–1.5) than men, especially in the frontal region (OR 1.6; 95% CI 1.2–2.1 and OR 1.6; 95% CI 1.2–2.2, for severe frontal periventricular and subcortical white matter lesions, respectively).
Discussion
Our study shows that the severity of subcortical and periventricular white matter lesions is dependent on age and sex. We confirmed the significant association between severity of white matter lesions and age. In addition we found that women tended to more often have white matter lesions of both kinds, especially in the frontal region.
The strength of this study is its large number of elderly people, including persons in institutions. Another important feature of our study is the distinction between white matter lesions in the subcortical and the periventricular region, and according to lobe.
However, some potential methodological shortcomings need to be considered. Our study had a response rate of 73% in subjects aged 60–70 years decreasing to 48% in participants aged between 80–90 years. This may lead to selection bias, especially in the oldest age category. We consider it likely that if participation in our study were related to the degree of white matter lesions, this would probably have resulted in persons with more severe white matter lesions participating less. Therefore the mean volume of subcortical white matter lesions and the mean grade of periventricular white matter lesions has probably been underestimated. This particularly applies to the oldest participants, among whom the response was lowest. However, we consider it unlikely that the sex difference for white matter lesions has been influenced by selection bias, as the response rate was similar for men and women in any age category.
Another point of concern is the validity of the white matter lesion rating scale, as there is potential for measurement error in this procedure. Although we chose anatomical landmarks to separate the lobes we cannot exclude the possibility that some misclassification occurred. As it is unlikely that this misclassification would be different for the sexes or age categories, the resulting bias will be non-differential. When subcortical and periventricular white matter lesions are both abundantly present, it may sometimes be difficult to distinguish between the two. However, our intrarater and interrater studies showed an excellent to high reliability, suggesting that this was not a major problem in our study.
An important aspect of our rating scale is that it distinguishes between subcortical and periventricular white matter lesions while their severity was also recorded. This will allow us to evaluate whether white matter lesions in these two regions have a different pathogenetic background and different clinical correlates.
Our study showed that subcortical white matter lesion volume was highest in the frontal and parietal lobes, 20 and 100 times higher than in the occipital and temporal lobes, respectively. Although the frontal and parietal lobes are larger than the occipital and the temporal lobes, this difference cannot explain the vast difference in white matter lesion volume. Scheltens et al found in a study of 24 “normal” elderly subjects (mean age 68.0 years) that the severity of white matter lesions was highest in the frontal lobe.19 This finding was even more marked in subjects with Alzheimer's disease. They explained this finding by overrepresentation of the frontal and parietal lobe compared with the occipital and the temporal lobe axial slices.19 We cannot exclude the possibility that we have relatively overestimated the frontal or parietal lobes, but again the magnitude of the difference in the volume of white matter lesions seems out of proportion to this. We are not aware of any difference in vascularisation between the lobes that might explain the large interlobe difference in the prevalence of white matter lesions.
Our study confirms previous findings of a relatively high prevalence and severity of white matter lesions among women.1 This was also found in the Cardiovascular Health Study and the Atherosclerosis Risk in Communities Study.2 3 This could be mainly attributed to the significant differences for the subcortical and periventricular white matter lesions in the frontal region. The higher prevalence of white matter lesions among women was in accordance with magnetic resonance spectroscopy studies that were done in the Rotterdam Study part of our study population. We found an increased variance in the ratio between choline, creatinine, and N-acetyl aspartate concentrations in the frontal periventricular region, and concentrations of those metabolites in the whole brain in women compared with men, which may be compatible with the finding of an increased prevalence of white matter lesions in women.20 It is unclear how these sex differences must be explained. One possibility is an increased susceptibility for ischaemia of the brain secondary to the reduction in estrogen concentrations after menopause plays a part. The occurrence of hypoxia or ischaemia in the cerebral white matter is commonly considered as an intermediate factor in the pathogenesis of white matter lesions.6Estrogens have important functions in the brain, including an increase in cerebral blood flow, protection against oxidative stress, stimulation of synaptogenesis, and prevention of neuronal atrophy.21-23 The postmenopausal estrogen reduction might make the female brain more vulnerable by reduction of cerebral blood flow (ischaemia) and impairment of neuronal repair mechanisms. This hypothesis is supported by in vitro studies, which showed protective effects of estrogens on menopause related cerebral damage by excitotoxicity and the action of free radicals, as occurs during cerebral ischaemia.24-28 As there is a morphological and epidemiological overlap between vascular dementia and Alzheimer's disease, the increased prevalence of cerebral white matter lesions in women could underlie the higher incidence of Alzheimer's disease among women, even after adjustment for prolonged life expectancy, especially at high ages.29 This hypothesis, which we did not attempt to test in this study, about the possible role of estrogens is supported by the finding of a significantly increased incidence of Alzheimer's disease among women who did not use estrogen replacement therapy.30 31
In conclusion, prevalence of cerebral white matter lesions increased with age. Women tended to have more often severe white matter lesions compared with men, especially in the frontal region. Large prospective population based studies are needed to investigate what underlies these differences and in particular to which factors play a part in the presence and development of white matter lesions and the attendant cognitive decline.
Acknowledgments
This study was supported by a grant from the Netherlands Organization for Scientific Research (NWO) and the Netherlands Health Research and Development Council (ZON). MMBB is a fellow of the Royal Netherlands Academy of Arts and Sciences. We thank Bart Schraa and Deni Kraus from the Daniel den Hoed Cancer Clinic, Erasmus Medical Center Rotterdam, The Netherlands and technicians from the Department of Radiology, University Hospital Utrecht, The Netherlands for their skilled experience in making the MR scans.