Article Text

Abstract
A young woman with pre-eclampsia became unresponsive shortly after delivery. Examination revealed extensive brain stem dysfunction with absent pupillary light reflexes and decerebrate posturing. Computed tomography showed hypodensity throughout the brain stem, and it was initially thought that she had suffered catastrophic brain stem infarction. However, magnetic resonance diffusion imaging and apparent diffusion coefficient mapping showed that she had brain stem vasogenic oedema (posterior reversible encephalopathy syndrome, PRES), rather than cytotoxic oedema. With antihypertensive and supportive treatment, she recovered rapidly, and had no abnormalities on repeat imaging.
- posterior reversible encephalopathy syndrome
- diffusion weighted MRI
- eclampsia, hypertensive encephalopathy
Statistics from Altmetric.com
- posterior reversible encephalopathy syndrome
- diffusion weighted MRI
- eclampsia, hypertensive encephalopathy
CASE REPORT
A 20 year old pregnant woman presented at 27 weeks gestation with a two week history of headache and lower extremity swelling. Her blood pressure was 160/100 mm Hg and there was periorbital and lower extremity oedema. Urinalysis revealed 4+ proteinuria. She was admitted with a diagnosis of pre-eclampsia.
Soon after admission, she began to complain of epigastric pain, nausea, and vomiting, and despite antihypertensive treatment her blood pressure rose to 179/104 mm Hg. Owing to concerns about worsening pre-eclampsia, labour was induced with dinoprostone, and a magnesium sulphate infusion was begun. During labour, she became increasingly somnolent, and following the delivery of a live preterm infant she became comatose.
Examination revealed no response to painful stimuli, fixed mid-position pupils, complete ophthalmoplegia, and extensor posturing in all four limbs. Laboratory investigations showed raised aspartate transaminase and alanine transaminase (881 and 395 IU/l, respectively), low platelets (99 000/mm3), and a packed cell volume of 30 g/dl, consistent with HELLP syndrome (haemolysis, elevated liver enzymes, low platelets).
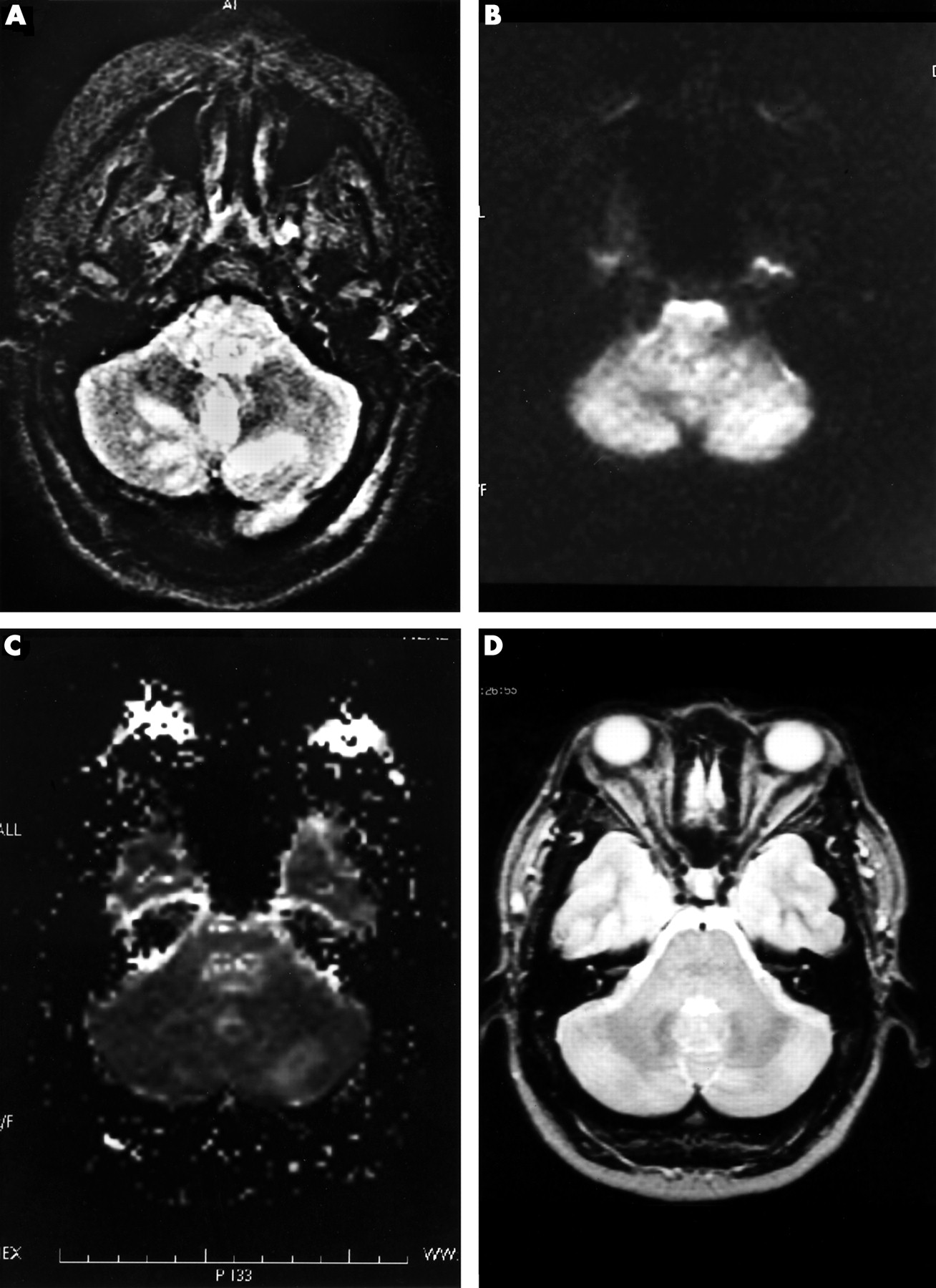
Computed tomography of the head revealed diffuse cerebral oedema and hypodensity of the midbrain, pons, and bilateral thalami. Magnetic resonance imaging (MRI) of the brain (fig 1A) showed T2 signal hyperintensity in the medulla, pons, midbrain, thalami, anterior and posterior limbs of the internal capsules, the external capsules, the caudate nuclei, and the occipital lobes bilaterally. The perimesencephalic cisterns and superficial cortical sulci were effaced. Diffusion weighted imaging (fig 1B) and apparent diffusion coefficient (ADC) mapping (fig 1C) suggested that the areas of hyperintensity were caused by vasogenic oedema rather than infarction. Cerebral transcranial Doppler ultrasound scans, magnetic resonance angiography, and magnetic resonance venography were all normal.
{kind=link}
(A) T2 axial magnetic resonance imaging (MRI) of the brain, showing signal hyperintensity throughout the pons with discrete hyperintense areas within the cerebellum. (B) Diffusion weighted MRI brain sequence showing no significant signal abnormality. (C) Apparent diffusion coefficient (ADC) map showing bright signal (increased apparent diffusion coefficient) in pons and cerebellum. (D) T2 axial MRI of brain two weeks later, revealing complete resolution of pontine and cerebellar hyperintensity.
The patient was intubated and ventilated, and a subarachnoid bolt was placed, which showed a raised intracranial pressure of 32 cm H2O. With appropriate blood pressure control and supportive care, her examination and abnormal laboratory indices improved markedly, so that by hospital day 5, she was discharged home, walking out of the hospital with no neurological deficit. A repeat MRI of the brain two weeks later (fig 1D) revealed no abnormalities.
DISCUSSION
A posterior reversible encephalopathy syndrome (PRES) may occur in various conditions, including hypertensive encephalopathy, pre-eclampsia/eclampsia, treatment with immunosuppressive agents (for example, cyclosporin A, FK-506), and uraemia.1–4 The clinical findings are those of encephalopathy (headache, altered conscious level, vomiting, seizures) and abnormalities of visual perception. The radiological findings are of oedema involving the white matter in the posterior portions of the cerebral hemispheres, especially bilaterally in the parieto-occipital regions. Less commonly, the frontal lobes, brain stem, cerebellum, and basal ganglia are involved.5,6 As the grey matter is often involved in addition to white matter, the term “PRES” is now preferred by some investigators to the original name—“reversible posterior leucoencephalopathy syndrome”—described by Hinchey et al in 1996.1,7 Indeed, when fluid attenuated inversion recovery (FLAIR) imaging is used rather than conventional T2 weighted imaging, cortical oedema is seen in 94% of cases.8 Characteristically, the clinical signs and imaging abnormalities are reversible with appropriate treatment, such as controlling blood pressure and discontinuing the offending immunosuppressive agent.
The pathophysiology of PRES is thought to be a “leaky” blood–brain barrier.9 In the hypertensive encephalopathies, this may result from the systemic blood pressure exceeding the autoregulatory capacity of the cerebral vasculature, with subsequent transudation of fluid across the blood–brain barrier. Direct endothelial cell dysfunction with a resulting increase in barrier permeability is also thought to play a role, particularly in the cases of PRES that are not associated with hypertension (for example, the haemolytic–uraemic syndrome, some cases of FK506, and cyclosporin A induced encephalopathy). Why the anterior cerebral circulation territories are relatively spared poses an interesting question. It is known that the anterior cerebral circulation is richly innervated by sympathetic nerves from the superior cervical ganglion, in contrast to the vertobrobasilar vessels which are relatively devoid of sympathetic innervation.10 Perhaps sympathetically mediated vasoconstriction protects the anterior circulation from overperfusion in acute hypertension.
Our case illustrates the value of diffusion weighted MRI with ADC mapping in distinguishing between cytotoxic and vasogenic cerebral oedema, which can both occur in eclampsia.2,11,12 In our patient, the lack of increased signal on diffusion weighted MRI accompanied by increased ADC values showed that the brain stem oedema was vasogenic and not cytotoxic. This suggested the diagnosis of PRES rather than brain stem infarction. This distinction was critical in that it obviated the need for intra-arterial thrombolysis for suspected basilar thrombosis, and resulted in appropriate antihypertensive treatment being initiated promptly, thus perhaps preventing a permanent neurological deficit from subsequent cerebral infarction.13 Indeed, if we had presumed that the diagnosis was ischaemic stroke, then the treatment guidelines would have dictated a less aggressive approach to controlling the hypertension,14 with the likelihood of a less favourable outcome. Finally, the distinction between PRES and extensive brain stem infarction in our comatose patient had obvious implications for the possible reversibility of the neurological deficit.