Article Text

Abstract
Objective: The appropriate management of unruptured intracranial aneurysms depends on a complete understanding of their natural history and on the risks and efficacy of treatment options. There is little current data on the risks of endovascular therapy for these aneurysms. The aim of this study was to assess outcome of endovascular treatment of unruptured intracranial aneurysms.
Method: A retrospective analysis was performed on all unruptured aneurysms treated by Guglielmi detachable (GD) coils at this institution from 1994 to 2000.
Results: Seventy three unruptured aneurysms were treated in 62 patients. There were 52 female and 10 male patients, with a median age of 55.7 years. Clinical background was: subarachnoid haemorrhage due to rupture of an additional aneurysm (40), headache (4), third nerve palsy (four), familial (four), and incidental (10). There were 14 technical failures with no clinical sequelae. Four procedural complications occurred (5.5%, 95% confidence interval (95% CI) 0.3% to 10.9%). One patient had temporary clinical sequelae (1.4%, 95% CI 0% to 2.7%); 79% of treated aneurysms had stable occlusions at follow up, 10.5% showed improved occlusion grade, 10.5% showed some recurrence, and three patients have required retreatment.
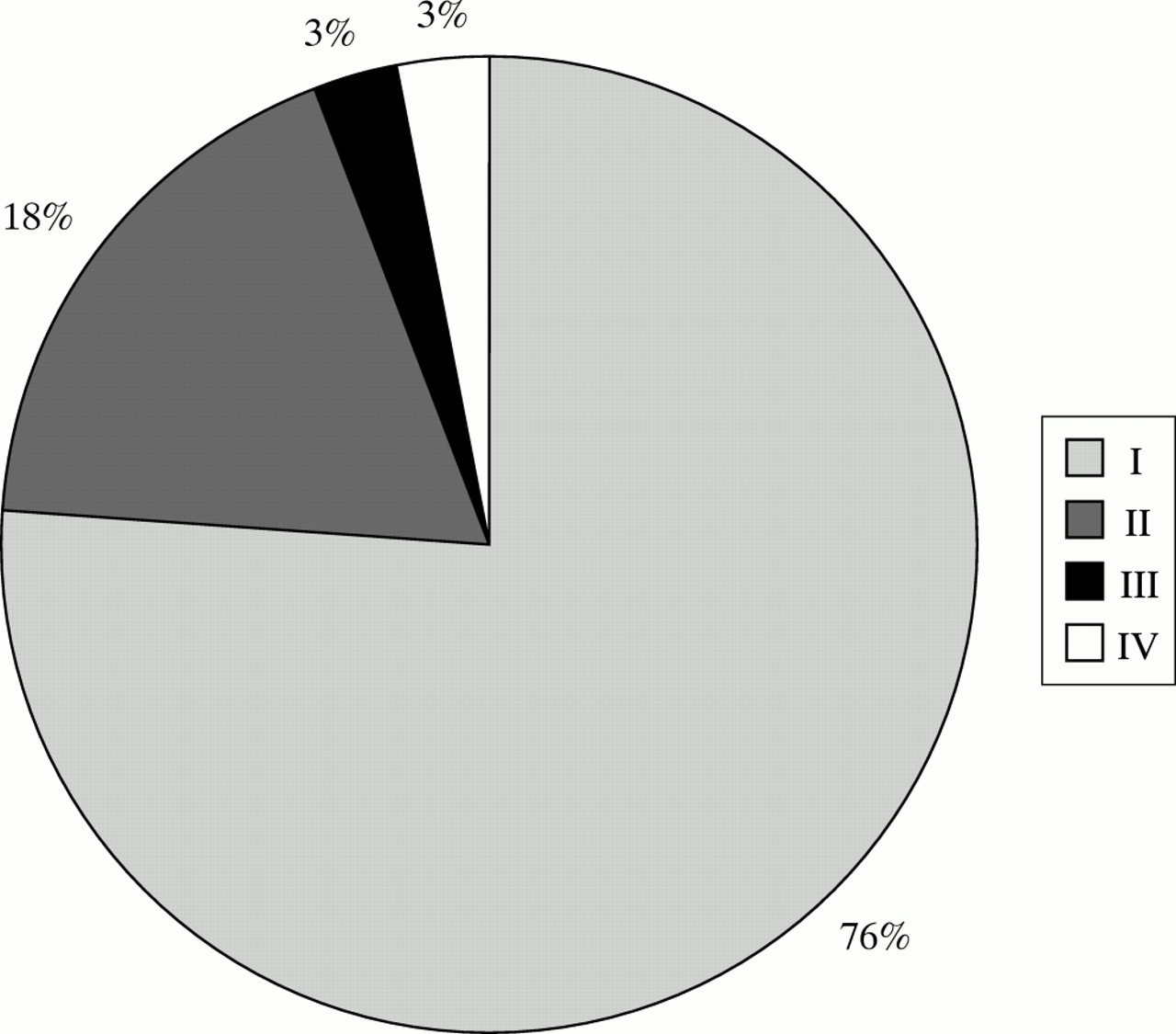
Follow up modified Glasgow outcome scores were grade 1, 71%; grade 2, 18%; grade 3, 3%; grade 4, 3%. There were no deaths or haemorrhages during the follow up period. Two patients died as a result of complications from subarachnoid haemorrhage.
Conclusion: The endovascular treatment of patients with unruptured aneurysms is safe with few clinical or procedural complications. Poor outcomes were only seen in those patients who presented with subarachnoid haemorrhage due to rupture of an aneurysm at another site.
- intracranial aneurysm
- unruptured
- embolisation
- GDC, Guglielmi detachable coil
- WFNS, World Federation of Neurological Surgeons
- GOS, Glasgow outcome score
- ISUIA, international study of unruptured intracranial aneurysms
- QALYs, quality adjusted life-years
- ISAT, International Subarachnoid Aneurysm Trial
Statistics from Altmetric.com
- GDC, Guglielmi detachable coil
- WFNS, World Federation of Neurological Surgeons
- GOS, Glasgow outcome score
- ISUIA, international study of unruptured intracranial aneurysms
- QALYs, quality adjusted life-years
- ISAT, International Subarachnoid Aneurysm Trial
Despite advances in treatment and supportive therapy, subarachnoid haemorrhage remains a condition with a significant morbidity and mortality. Between 40% and 50% of patients will die as a result of their haemorrhage.1 Whereas the incidence of subarachnoid haemorrhage remains static, the incidence of unruptured intracranial aneurysms detected in life is increasing on account of increased sophistication, accessibility, and use of invasive and non-invasive imaging techniques for neurological symptoms that may or may not be related to their presence.2, 3
The finding of unruptured aneurysms in a patient allows the opportunity of providing preventive treatment. However, the treatment is only justified if the morbidity and mortality is less than the risk that the untreated aneurysm poses to the patient.
Aneurysm size is considered to be a significant risk factor for rupture.4–8 However, within a given aneurysm size population, there is considerable heterogeneity in rupture rates. Rupture rates for small (<10 mm) coincidental aneurysms in patients who have had subarachnoid haemorrhage from an additional aneurysm range from 0.5% a year4 to 1%,9 but has been reported as high as 3.2%.10 The International Study of Unruptured Intracranial Aneurysms (ISUIA) also demonstrated rupture risk for aneurysms less than 10 mm in those without prior subarachnoid haemorrhage to be 0.05% a year.4 Some studies have reported no critical size cut off for the risk of rupture.10, 11
Numerous studies have confirmed that the risk of rupture of an unruptured aneurysm is influenced also by aneurysm location (increased rates in the posterior circulation),4, 8, 12 multiplicity,10 morphology,12 smoking history,5 history of previous aneurysm rupture,4, 5, 13 family history, patient age (inversely),5, 14 symptoms related to the aneurysm,8 patient sex (higher rupture rates in women),8 and the presence of underlying vasculopathy.8
Aneurysms over 10 mm have rupture rates of 0.5%–1% a year.4 Tsutsumi et al calculated a cumulative rupture risk of aneurysms greater than 10 mm of 55.9% over 10 years.7 Giant aneurysms have rupture rates of 6% in the first year.4 Again, it is clear that size, although it increases the risk, is not the only important factor.
The early and late outcomes after surgery for unruptured aneurysms are well documented in the literature.4, 15–21 Surgery related morbidity between 1.9% and 18.5%, and mortality between 0.8% and 9.6% have been reported. Few studies have been published on the results and risks of endovascular therapy for unruptured aneurysms. Morbidity between 0% and 4.3% and mortality of 0% represent formidable results in 120 embolised unruptured aneurysms reported by Murayama et al.22
The successful management of unruptured aneurysms in an individual patient is highly complex and dependent on a full understanding of the expected natural history of their aneurysm, a full assessment of the patient (including life expectancy and their wishes), and an assessment of the risks and efficacy of interventions to prevent aneurysm rupture.
PATIENTS AND METHODS
A retrospective analysis was performed of the angiograms and case notes of all patients identified who had unruptured aneurysms treated at our unit. Only patients treated with Guglielmi detachable coils (GDCs) were included to ensure consistency of both short and long term results. The study period was from January 1994 to November 2000. A total of 62 patients were identified who had 73 unruptured aneurysms. Patients treated successfully, and those in whom treatment was abandoned were included in the study to provide an accurate picture of the overall risks of attempted and successful treatment. There were 52 female and 10 male patients. Median age was 55.7 years.
Clinical presentation was as follows: 40 patients (64.5%) presented with subarachnoid haemorrhage due to aneurysmal rupture at another site. Angiography demonstrated multiple aneurysms. In this group, the ruptured aneurysm was clipped in 19 cases and coiled in 19 cases. The selection of treatment of the ruptured aneurysm is primarily made on morphological grounds and aneurysm location. There was no difference in clinical grade between those patients who received endovascular or surgical therapy. In one case the ruptured aneurysm was initially subtotally coiled, then subsequently clipped. One patient had a small posterior inferior cerebellar artery aneurysm wrapped.
Three patients had cerebral angiography as a screening procedure on account of their family history. All of these patients were asymptomatic and had at least two first degree relatives who had proved aneurysmal intracranial haemorrhage. Four patients presented with painful third cranial nerve palsy due to an ipsilateral posterior communicating artery aneurysm. Four patients presented with chronic headache that precipitated cranial CT and/or MRI. Subarachnoid haemorrhage was not suspected in any of these patients. Imaging noted or suspected the presence of aneurysms and cerebral angiography was subsequently performed to confirm this and to plan for treatment. All of the aneurysms in these patients were less than 1 cm in size and considered too small to contribute to the patients' symptoms.
One patient presented with visual failure due to the mass effect of a giant ipsilateral carotid ophthalmic artery aneurysm.
One patient presented with seizures. Brain MRI and subsequent angiography demonstrated a cerebellar arteriovenous malformation and an unruptured basilar tip aneurysm.
Nine patients presented with various conditions including facial nerve palsy, transient ischaemic attacks, and tinnitus. Brain MRI was performed on all these patients before angiography. In this group, the aneurysm was considered to be truly incidental to the patient's presenting clinical complaint on account of their small size or a lack of anatomical correlation with symptoms.
To assess the clinical outcomes more meaningfully, the patients were divided into three groups.
Group1
This group comprised patients who presented with subarachnoid haemorrhage who underwent embolisation of their unruptured aneurysm(s) within 1 week of presentation. Included in this group are those patients who presented with aneurysmal mass effect (for example, third nerve palsy), as these patients are managed acutely because of the risk of imminent rupture or permanent neurological deficit (22 patients).
Group 2
These were patients with electively treated coincidental aneurysms who had previously had a ruptured aneurysm treated (23 patients).
Group 3
These were patients with truly incidental aneurysms (17 patients).
Aneurysm morphology and case selection
Aneurysms selected for treatment were encountered in the following locations: anterior communicating artery 10 (13.7%); posterior communicating artery 18 (24.6%); middle cerebral artery 12 (16.4%); internal carotid artery 21 (28.8%); basilar artery 10 (13.7%); superior cerebellar artery one (1.4%), and pericallosal artery one (1.4%).
Most aneurysms were less than 10 mm in size, with a neck less than 4 mm in width (table 1). There were an additional 30 aneurysms found in this patient cohort that were not suitable for endovascular therapy; 18 were too small (1–2 mm), four had necks that were considered too wide to retain a coil, seven aneurysms were not suitable both in terms of size and neck width, and one aneurysm could not be accessed due to arterial spasm.
Morphology of aneurysms
Group 1 patients who presented with subarachnoid haemorrhage (17) were treated at the same time as the definitive treatment of the ruptured aneurysm, which was coiling in 13/17 (76%), and clipping in 4/17 (24%) cases. World Federation of Neurological Surgeons (WFNS) clinical grade at the time of treatment in these cases was grade 1 in 10, grade 2 in six, and grade five in one patient. The last patient had severe acute hydrocephalus at presentation responsible for the poor clinical grade. External ventricular drainage was started, which was followed by aneurysm rebleeding. Angiography and embolisation of ruptured and unruptured aneurysms was performed as an emergency procedure. The four cases with third nerve palsy due to posterior communicating artery aneurysm and the patient with visual failure due to internal carotid artery aneurysm were all well (WFNS grade 0) at the time of treatment.
Group 2 patients were treated between 2 months and 2 years 4 months (median 8 months) after the initial haemorrhage. All of these patients had made a full recovery from their subarachnoid haemorrhage and were either WFNS grade I (18 patients; 78%) or WFNS grade II (five patients; 22%). Their functional outcomes were good also; all patients were assessed as grade 1 on the Modified Glasgow outcome score (GOS) at the time of treatment (fully recovered and independent). All group 3 patients were well at the time of treatment.
Technical and radiographic results
Treatment was attempted in all 73 aneurysms.
Technical failures
In 13/73 (17.8%) cases we were not able to successfully coil the aneurysm. In four patients this was due to vessel tortuosity. All these cases occurred before 1998. The introduction of more advanced braided catheter technology in the past 2 years has resulted in a major improvement in the success rate of treatment. In one case, failure to gain access was due to severe vasospasm secondary to subarachnoid haemorrhage. Another case was abandoned as the guidewire perforated a small vessel on attempting to catheterise the aneurysm. In the remaining seven cases, the aneurysm was not able to retain the coil ball on account of the morphology of the neck and aneurysm size.
Of the 12 patients who remained well, five had their unruptured aneurysm subsequently clipped, seven had no further interventions for their aneurysms.
Technical successes
In the remaining 60 aneurysms, treatment was successfully completed in a standard manner. The patients were placed under general anaesthesia and the aneurysm sac embolised with GD coils under full systemic heparinisation.
Assessment of the technical results is principally based on a visual judgement of the coil density and volume of aneurysm occlusion at the end of the procedure.
Although clearly subjective, the simple grading system we have used is reproducible and is adapted from methods used by Zubillaga et al.23 Where there is doubt or disagreement regarding the occlusion grade, it is downgraded.
Grade I was a totally occluded aneurysm with no lumen or neck remnant visible. Grade II was 90% to 99% (subtotal) obliteration of the aneurysm lumen. Grade III was less than 90% (incomplete) obliteration of the aneurysm.
Aneurysms less than 10 mm in size were 90% obliterated or more in 83% of cases. Aneurysms 10–25 mm in size were 90% obliterated or more in 83% of cases. As expected, results for the two giant aneurysms (>25 mm) were less impressive, with one being incompletely occluded, and one subtotally occluded (table 2).
Technical results
Postprocedure clinical results
Group 1 patients had GOS scores of 1 in 19/22 (86%) patients, grade 2 in one (persistent third nerve palsy), and grade 5 in two. These two patients died from complications of their haemorrhage: one who presented in WFNS grade 5 due to hydrocephalus and rerupture and one patient in whom embolisation had to be abandoned due to vasospasm secondary to subarachnoid haemorrhage. The patient in whom treatment was abandoned due to vessel perforation eventually made a full recovery after a prolonged stay in hospital.
All group 2 patients had excellent outcome (GOS 1) after treatment. There was no additional morbidity attributable to patient age in our group.
Group 3 patients were all clinically well at the time of treatment. On discharge, all patients were GOS grade 1.
There were no clinical complications in 12/13 (92%) patients in whom coiling was attempted and failed. One patient who had severe vasospasm at the time of attempted coiling eventually died as a result of a subarachnoid haemorrhage. Overall, the early treatment related mortality was 0%, and treatment related morbidity was 1.4% (95% confidence interval (95% CI) 0.35 to 2.7%).
Patient follow up
Radiological results
Angiographic and clinical follow up was available in 39/51 (76.5%) patients who were treated. Follow up is not available in the following: one patient who died; five patients recently treated where follow up is not yet available; five elderly patients in whom no follow up has been arranged as it was considered appropriate to offer no further treatment, regardless of the angiographic appearances. One patient was lost to follow up. Of the thirteen patients in whom treatment failed, clinical follow up was available for the patient in whom a vessel was perforated. No patients died during the follow up period of rehaemorrhage. Follow up was available in 48/74 aneurysms in total and 48/60 (80%) of aneurysms treated. Time between treatment and latest follow up ranged from 2 months to 2 years 4 months, median 8 months.
Angiographic occlusion grades are shown in table 3. Thirty eight of 48 (79%) aneurysms were stable at follow up. Five aneurysms (10.5% of those followed up) showed improved occlusion grades. This was due, in all cases, to residual lumen or distal aneurysm locule undergoing subsequent thrombosis.
Angiographic follow up
A further five aneurysms (10.5%) showed recurrence at follow up. All of these showed some neck enlargement within the first 6 months to 1 year after treatment. One patient required two repeat endovascular procedures for a wide necked carotid termination aneurysm. A second patient showed grade I to III recurrence at follow up and subsequently the aneurysm was clipped. The third patient had a further embolisation after grade I to II recurrence. All the patients remain well, and the two aneurysms requiring additional endovascular treatment remain under surveillance.
Clinical follow up
Thirty nine patients were followed up clinically. All of these patients are reviewed by the neurosurgical team and have a full neurological examination. In addition, the patient completes a standardised form including information on psychological profile, level of functional independence, and symptomatology—for example, headache and sleep disturbance. The clinical condition of those patients who were followed up, and those who succumbed to their subarachnoid haemorrhage, is summarised and presented in figure 1. Thity seven of 39 (95%) patients remain well and were at or close to their premorbid state.
{kind=link}
Modified Glasgow outcome scores at clinical follow up.
Group 1—Fourteen of 22 (63.5%) patients were followed up. Five of 14 were GOS grade II, seven grade II, one grade III, and one grade IV. These figures represent our poorest outcomes and arose due to the complications of their subarachnoid haemorrhage. Two patients who had early aggressive management of all their aneurysms were dependent or vegetative despite good initial clinical response. The deterioration in these patients was attributable to in one case, multiple shunt infections, and in the other to vasospasm.
Group 2—Thirteen of 23 (56.5%) patients were followed up and all remain well.
Group 3—Twelve of 17 (70%) patients were followed up. All of these patients were completely well (GOS 1). The high follow up rate of these patients considered to have truly incidental aneurysms is due mainly to large aneurysm size and the young age of most of this group.
Technical and procedural complications
There were four procedural complications in the 73 aneurysms where treatment was attempted (5.5%: 95% CI 0.3% to 10.9%).
One patient had a 2 cm, wide necked internal carotid aneurysm treated at the same time as their ruptured aneurysm. The coil ball prolapsed into the internal carotid bifurcation occluding the A1 segment and reducing flow in the middle cerebral artery. A non-detachable silicone balloon was used to displace the coil ball and improved flow in middle and anterior cerebral arteries. The patient remained asymptomatic and follow up angiography 3 years later shows both anterior and middle cerebral arteries filling well.
A second patient had presented with subarachnoid haemorrhage due to rupture of a right middle cerebral artery aneurysm. An attempt was made to embolise an unruptured left anterior communicating artery aneurysm. During manipulation of the guidewire in the distal left internal carotid artery, a small vessel was perforated and subsequent vasospasm precluded further intervention. There were no significant clinical sequelae but a prolonged stay in hospital was required to manage the vasospasm. The patient made a full recovery, and both the unruptured anterior communicating artery and middle cerebral artery aneurysms were clipped. Angiography 3 years after initial presentation showed normal vascular appearances.
A third patient developed severe vasospasm around the guiding catheter tip. Although this is not an unusual complication, there was significant flow restriction and papaverine infusion (100 mg) was required to alleviate the spasm. Embolisation proceeded uneventfully. The patient remained well, and at follow up, the carotid artery was morphologically normal.
In the final case, a small internal carotid artery dissection occurred during catheter exchange over a long wire. This was not flow restricting and the patient remained well without additional therapeutic measures.
DISCUSSION
The management of unruptured aneurysms remains controversial and depends on a full understanding of their natural history balanced against the risks of treatment and long term protection afforded.
Aneurysm prevalence in the general population shows wide variation. Prevalences in the general population between 0.5% and 6.8% have been reported.11, 24–28 In those with a family history of subarachnoid haemorrhage, the prevalence of unruptured aneurysms has been reported at 10%-13.9%.28, 29 The prevalence in women is higher than in men: 2.4 times higher in the study by Iwamoto et al, a consecutive necropsy series in Japan.27 This study, and the review by Rinkel et al8 also confirmed a higher prevalence of aneurysms in elderly people.
There is some evidence that the detection of aneurysms during life is increasing due to increased use of accurate imaging methods and due to screening programmes introduced in Japan (“No Dokku” or brain check).2, 3 In one Japanese study by Kojima et al, the prevalence of aneurysms detected by MRI was as high as 8.5%.28
Variations in the prevalence of aneurysms in different populations probably reflect genuine racial/genetic influences in aneurysm aetiology and may not pertain to a given population. Study design also seems to influence the recorded prevalence. A systematic review by Rinkel et al showed prevalence to vary between 0.4% in retrospective necropsy series to 6% in prospective angiography series.8 However, it is clear that in a particular population, the number of unruptured aneurysms far outweighs those that have ruptured. Therefore, unruptured aneurysms will be identified with regularity in most units involved in neuroimaging and the management conundrum of these patients is a universal problem.
Unruptured aneurysms are undoubtedly a heterogeneous entity, both in terms of morphology and behaviour. This is reflected in the wide variation in reported rupture risks in the literature between 0.05% and 5% a year (a 100-fold difference),4–6, 9–11, 13, 14, 30 up to 55.9% over 10 years for giant aneurysms.7
Aneurysm size is considered to be the most important factor in predicting risk of rupture; however, considerable variation in rupture rates exist for aneurysms of a given size. The ISUIA is the largest study to date on the natural history of unruptured aneurysms. This showed that aneurysms less than 10 mm in patients without a history of subarachnoid haemorrhage ruptured at a rate of 0.05% a year and those with prior subarachnoid haemorrhage had a rupture rate of 0.5% a year. Aneurysms larger than 10 mm had an annual rupture risk of 0.5–1%.4
Other studies have found the incidence of rupture of all coincidental aneurysms to be between 1%9 and 3.2% a year,10 with hypertension9 and aneurysm multiplicity10 being specific risk factors. Juvela et al followed up 181 aneurysms in 142 patients for a median of 19.7 years. They showed an average annual rupture rate of 1.3%. The relative risk was calculated at 1.11/mm aneurysm diameter, and a strong correlation between smoking history and rupture (relative risk 3.04), and an inverse age correlation with rupture risk (relative risk 0.97 a year) were found.5 Other specific risk factors for rupture include: aneurysm morphology (multilobular)12; posterior location4, 8, 12; symptoms related to mass effect,8 and female sex.8
However a study by Rosenorn et al failed to find a critical size of aneurysm that predicted rupture. Indeed, in all studies, a specific aneurysm size that could predict rupture has proved elusive, although increasing size presents increased risk.11 A retrospective, observational study conducted in Japan by Yasui et al showed that aneurysms less than 5 mm in size at discovery could rupture at follow up and most had increased in size over the observation period.30
The distribution of unruptured aneurysms in our population shows a predominance of carotid-ophthalmic and terminal carotid aneurysms. There was an underrepresentation of anterior communicating artery aneurysms, and this was also the case in the ISUIA study. The possible explanation for this is that anterior communicating artery aneurysms have a different natural history; they may form and subsequently rupture rapidly so that the opportunity to detect these as unruptured lesions is limited.
The early and late outcomes after surgery of these lesions is well documented in the literature.3, 4, 15–20 A meta-analysis by Raaymakers et al of 61 studies of surgical results on 2460 patients with 2568 operated aneurysms showed a permanent morbidity of 10.9% and mortality of 2.6%, with the best results in small and anterior circulation aneurysms.17 Deruty et al identified other specific risk factors for increased surgical morbity-mortality as cerebral ischaemia and the presence of atheroma related to the internal carotid artery or aneurysm.19
A study by Johnston et al 16 compared the clinical outcomes of patients who had unruptured aneurysms treated by surgery and embolisation. Morbidity was significantly higher in the surgical group (18.5%) than the endovascular group (10.6%). Mortality was also higher in the surgical group (2.3% compared with 0.4%), but this was not statistically significant. Hospital stay was also longer for the surgical group and this has important resource implications. A further study by the same authors on 68 surgically treated and 62 endovascularly treated patients with unruptured aneurysms showed improved clinical outcomes, shorter hospital stay, shorter recovery period, reduced costs and reduced long term symptoms in those patients treated by coil embolisation.20
The largest study of the embolisation of unruptured aneurysms reported in the literature is by Murayama et al and includes results on 115 patients with 120 aneurysms.22 Total or subtotal occlusion was achieved in 91% of cases. The clinical complication rate was 4.3% in the first 50 patients treated, and 0% in the last 65 treated. Late rupture occurred in one patient with a subtotally occluded aneurysm. Our results compare very favourably with these and the surgical series above, and to date we have had no aneurysm rupture.
Two studies, by Raymond et al and Bavinski et al, reported results of the embolisation of basilar artery aneurysms. Their data included a total of 18 unruptured cases. Clinical complications were not encountered in these groups and there were no haemorrhages at follow up. However, only aneurysms with a narrow neck remained stable at follow up angiography.21, 32 In the retrospective study by Pierot et al permanent neurological deficit occurred in 6.5% of patients, and one rebleed in an incompletely treated aneurysm. There were no deaths reported in their series.33
Cost-benefit analyses have been calculated for surgery of unruptured aneurysms. Using a mathematical model, Chang and Kirito demonstrated a maximum expected gain in life expectancy of 3.9 years for a patient aged 40, assuming an operative mortality of 1% and an annual rupture rate of 1%.34 Not surprisingly, the gain in life expectancy decreases with increasing age, increased operative mortality, and lower assumed rupture risk. There seems to be no benefit in treating patients over 70, even with an operative mortality of 0% unless the risk of aneurysm rupture is at least 1.5% a year. Johnston et al 35 showed a loss of quality adjusted life-years (QALYs) for surgery and embolisation of incidental, unruptured, small (<10 mm) aneurysms. A gain in QALYs was calculated for surgery of aneurysms greater than 10 mm, coincidental, and symptomatic aneurysms. Endovascular therapy was marginally more cost effective than surgery in their model.
Aoki et al, using a Markovian decision analysis model, showed that a treatment policy is justified if the rupture rate is 0.9% a year or higher.36 Kallmes et al have also shown that the cut off point for cost-effectiveness for GDC treatment of unruptured aneurysms also occurs at a rupture rate of 1% a year and that this was the most significant variable.37 Yoshimoto and Wakai, also using a Markovian model, found that the most significant variable affecting cost-effectiveness of screening and treating unruptured aneurysms was the annual rupture rate.3 Assuming a rupture risk of 0.05% for truly incidental aneurysms, screening and treating unruptured aneurysms is not justified.
Yundt et al reported a study on the resource costs of surgical treatment of ruptured and unruptured aneurysms. The most important factor influencing treatment costs for these patients was intensive care usage and this accounted for the relatively low treatment costs for unruptured aneurysms.38 King et al calculated a gain in 0.88 QALYs for unruptured aneurysm treatment in a 50 year old man compared with a non-treatment policy, with a cost of $24 200 per QALY. This compares well with other medical interventions in this age group such as total knee replacement and antihypertensive therapy.39
In our unit unruptured aneurysms are encountered with increasing regularity and until recently we have successfully treated these lesions. Our results compare very favourably with the above studies and add to the growing body of evidence that in selected cases, endovascular treatment is both safe and effective for these lesions. Our procedure related mortality was zero, and long term morbidity was also zero, despite technical complications that could clearly have had adverse outcomes. Our poorest results occurred in those patients who had subarachnoid haemorrhage and received early treatment of unruptured aneurysms. The early treatment of unruptured, coincidental aneurysms is probably not justified. Our approach now is to consider treating the unruptured aneurysm electively in patients who have made a meaningful recovery from their initial haemorrhage. The patient can then decide if they wish to pursue treatment for the remaining aneurysm(s) having been made fully aware of the risks, uncertainties, and controversies involved.
If the risk of rupture from an unruptured aneurysm is at least 1% (taking into account aneurysm morphology, patient age, sex, smoking history, symptoms etc) and treatment related mortality remains low, then treatment can be justified by endovascular or surgical means. The lower costs of endovascular therapy may favour this method on purely economical grounds.
In our series, we have accrued a total of 83 years of follow up (an average of 2.2 years fore each patient, 1.7 years for each aneurysm). Ninety per cent of aneurysms either improved or remained stable at follow up with greater than 90% occlusion. All aneurysm recurrences occurred within the first year after treatment. Therefore, close angiographic follow up during this period is advocated to identify patients who will need either retreatment or continued surveillance.
Incompletely coiled aneurysms are known to rupture and it is assumed, although with no long term data as yet, that completely coiled aneurysms do not rupture. No patient currently under surveillance has had an intracranial haemorrhage.
The long term protection of patients is a vital component of effective treatment. Further follow up of this cohort of patients and the results of the International Subarachnoid Aneurysm Trial (ISAT) will be critical to the future justification of embolisation as a valid treatment method.
Our treatment policy for unruptured aneurysms has been influenced by the results of the ISUIA study, despite our good results. We will rarely treat unruptured aneurysms unless they are symptomatic, have a risk of rupture of at least 1% a year, or the patient requests treatment. In this case, our study will provide a useful guide to expected procedure related morbidity and mortality in our unit. If a decision is taken not to treat a given aneurysm, follow up with angiography or high quality non-invasive imaging is advocated to assess changes that will influence the future risk of rupture.
The management policy now pursued is in line with the recommendations recently published by the American Heart Association40 on the management of patients with unruptured aneurysms. In any given case, the decision making process will also be affected by coexisting medical conditions, individually assessed treatment risk, and patient wishes.
CONCLUSIONS
There will remain continuing controversy regarding the optimal management of unruptured aneurysms. However, we think that treatment of these lesions is justified if the following conditions are met.
That treatment related mortality and morbidity remains low.
The patient is young with a reasonable life expectancy.
The annual rupture risk of unruptured aneurysms is at least 1%.
An increasing body of evidence in the literature supports the clinical safety of endovascular aneurysm therapy. However, the ultimate goal of endovascular treatment of both ruptured and unruptured aneurysms is to provide lifelong protection. Continuing clinical and radiological follow up of these patients and the results of the ISAT trial will be crucial factors in justifying this approach to treatment in the future.