Article Text

Abstract
Objectives: Despite the growing use of intraoperative functional mapping in supratentorial low grade glioma (LGG) surgery, few studies have compared series of patients operated on without and with direct electrical stimulation (DES) by the same team. The present study compared the rate of LGG surgery performed in eloquent areas, the rate of postoperative sequelae, and the quality of resection during two consecutive periods in the same department—the first without and the second with the use of intraoperative electrophysiology.
Methods: Between 1985 and 1996, 100 patients harbouring a supratentorial LGG underwent surgery with no functional mapping (S1). Between 1996 and 2003, 122 patients were operated on in the same department for a supratentorial LGG using intraoperative cortico-subcortical DES (S2).
Results: Comparison between the two series showed that 35% of LGGs were operated on in eloquent areas in S1 versus 62% in S2 (p<0.0001), with 17% severe permanent deficits in S1 versus 6.5% in S2 (p<0.019). On postoperative MRI, 37% of resections were subtotal and 6% total in S1 versus 50.8% and 25.4%, respectively, in S2 (p<0.001). In both groups, survival was significantly related to the quality of resection.
Conclusions: The results of the present study allow, for the first time, quantification of the contribution of intraoperative DES in LGG resection. Indeed, the use of this method leads to the extension of indications of LGG surgery within eloquent areas; to a decrease in the risk of sequelae; and to improvement of the quality of tumour resection, with an impact on survival.
- DES, direct electrical stimulation
- LGG, low grade glioma
- functional mapping
- intraoperative stimulations
- language
- low grade glioma
- sensorimotor
Statistics from Altmetric.com
In the past decade, a growing number of authors have investigated the use of intraoperative mapping with direct electrical stimulations (DES) during tumour surgery near or within eloquent areas. It has been claimed that this method allows minimising postoperative permanent deficit while maximising the quality of resection, particularly in infiltrative tumours such as low grade gliomas (LGGs).1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21 However, few comparative studies of two series of patients operated on without and with DES by the same team are available in the literature.22–24 Due to the parallel development of neurofunctional imaging techniques, the real role of intraoperative DES is still matter of debate, since this has not been statistically proven.25
In the present study, we compared three variables, the rate of LGG surgery performed in eloquent areas, the rate of postoperative sequelae, and quality of tumour resection, during two consecutive periods in the same department, the first without the use of intraoperative electrophysiology (1985–96) and the second with DES (1996–2003). The aim of our work was not to study the impact of surgery on the natural history of LGG, but to try to quantify the exact contribution of the DES in surgical resection of supratentorial LGGs.
PATIENTS AND METHODS
Patients
Between 1985 and 2003, 222 patients underwent surgical resection for a supratentorial LGG in our institution, without any previous therapy. Two consecutive periods were identified for the present study:
-
from 1985 to October 1996, during which 100 patients were operated on without intraoperative electrophysiological mapping (retrospective study—series 1 (S1))
-
from November 1996 to 2003, during which 122 patients were operated on with the use of DES (prospective study—series 2 (S2)).
A part of this experience has been described previously, with special attention to the detailed neurological outcome in series 2,26 but no comparison was made with a surgical series in which intraoperative functional mapping was not done.
Preoperative evaluation
For both S1 and S2, we reviewed the presenting symptoms and preoperative neurological examination. Patients were classified in two groups:
-
Group I: no or mild deficit, with Karnofsky Performance Status (KPS)27 score ranging between 80 and 100
-
Group II: a severe deficit, which led to deterioration in the quality of life, with the patient unable to carry out normal activities (that is, KPS of 70 or less).
In both series, we analysed the topography of the tumour on a preoperative magnetic resonance (MR) image (T1-weighted and/or spoiled gradient images before and after gadolinium enhancement in the three orthogonal planes and T2-weighted axial images. Fluid attenuated inversion recovery (FLAIR)-weighted axial images were taken in the last three years of series 2). The volume of the tumour was evaluated using the method proposed by Berger et al1—that is, the product of the three largest diameters (two measured in the axial plane, the third measured in the sagittal plane, as we have previously reported28) divided by 2. All tumours were graded functionally, relative to their location with respect to the eloquent brain, into two groups:
-
tumours involving functional regions, according to the definition previously proposed by us29—for example, motor cortex/supplementary motor area, somatosensory cortex, speech centres, visual cortex, insular lobe, internal capsule and deep grey nuclei
-
tumours near or remote from eloquent areas and not invading these areas.
Intraoperative technique
In both series, we used the same surgical equipment (ultrasonic aspirator, bipolar coagulation, ultrasonography, operative microscope), except for the intraoperative functional mapping methods, which were not used in series 1. In series 2, intraoperative real-time functional cortico-subcortical mapping was performed during all the surgical procedures (motor mapping in 49 patients under general anaesthesia; sensorimotor and language mappings in 73 patients under local anaesthesia), using the technique of DES. We have described this technique in detail in previous reports,26,30,31 and it is based on the methodology described by Berger and Ojemann.32,33 Our aim was first to track and preserve the eloquent structures at each moment and each site of resection to avoid postoperative sequelae, and second to continue LGG removal until functional areas were encountered so as not to interrupt the surgery prematurely, thus optimising the quality of resection.
Briefly, a 5 mm spaced tips bipolar electrode delivering a biphasic current (pulse frequency 60 Hz, single pulse phase duration 1 ms, amplitude from 6 to 18 mA under general anaesthesia and from 2 to 6 mA under local anaesthesia; Ojemann Cortical Stimulator 1, Radionics Inc, Burlington, MA) was applied on the brain. First, we performed electrical mapping at the cortical level before tumour removal to identify the essential eloquent sites that must be avoided and thus defined the superficial boundaries of the resection according to functional data. In addition to sensorimotor mapping, language tasks included systematic counting, naming, and reading. We also included a calculation task for lesions in the left angular and supramarginalis gyri, and repetition and/or semantic tasks for tumours within the left mid-posterior temporal lobe. Second, direct stimulations, with the same electrical parameters as those used at the cortical level, were continuously applied during glioma removal at the subcortical level to detect sensorimotor and/or language pathways, which represent the deep functional limits of resection.
It is important to note that even in series 2, we did not use an intraoperative neuronavigation system with incorporation of preoperative functional neuroimaging data. We preferred to use a real-time ultrasonography system, not only to delineate the tumour before its removal but also to control the residual amount during the resection.
Postoperative evaluation
Similar to the preoperative evaluation, postoperative neurological examination and KPS scoring were reviewed in both series after the third month following the surgery. We also performed at least one postoperative magnetic resonance imaging (MRI) scan in all patients to evaluate the quality of glioma removal. The classification reported by Berger et al1 was used (for example, “total” resection in case of no residual signal abnormality, “subtotal” resection in case of less than 10 ml residue, and “partial” resection in case of more than 10 ml residue). The volume of the residue was calculated with the same methods used preoperatively. Finally, mortality was evaluated in relation to the quality of resection in both groups.
Statistics
We used χ2 and Fisher’s exact tests, except for the comparison of preoperative volumes of tumours: this analysis was performed using the non-parametric statistical tests, Wilcoxon’s and Kruskal–Wallis.
RESULTS
The clinical, radiological, and surgical data of both series are summarised in table 1.
Clinical, radiological, and surgical characteristics of 222 patients operated on for a low grade glioma (LGG) without (series 1) and with (series 2) intraoperative direct electrical stimulation (DES)
Clinical and radiological findings
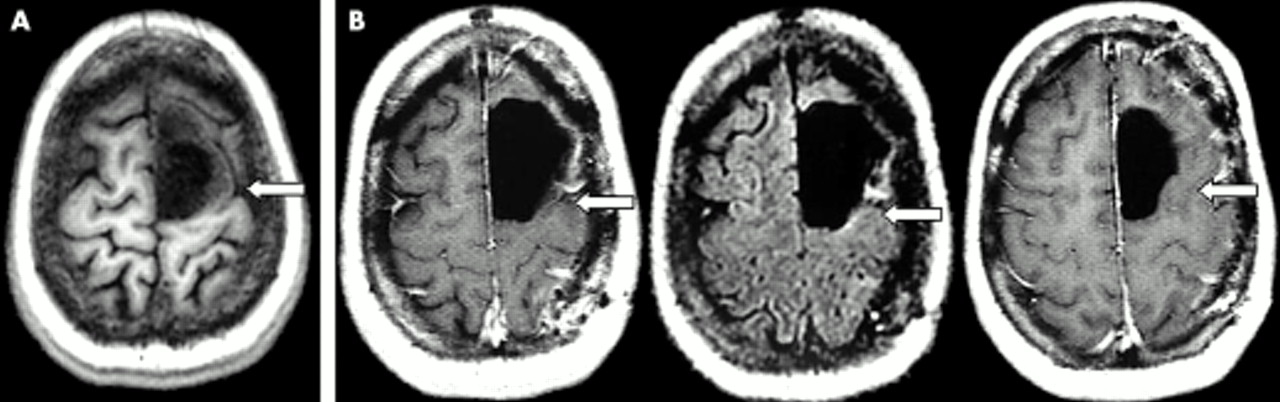
Seizures were the presenting symptoms in 95% of patients in both series. Clinically, the neurological examination was normal in 94 patients in S1 and 112 patients in S2. However, on the basis of the KPS scores, all patients from S1 and S2 were classed into group I—that is, with KPS between 80 and 100. In S1, 35 tumours involved functional areas (table 1 and fig 1A) whereas in S2, 76 tumours were located within eloquent regions (table l and fig 2A) (p<0.0001).
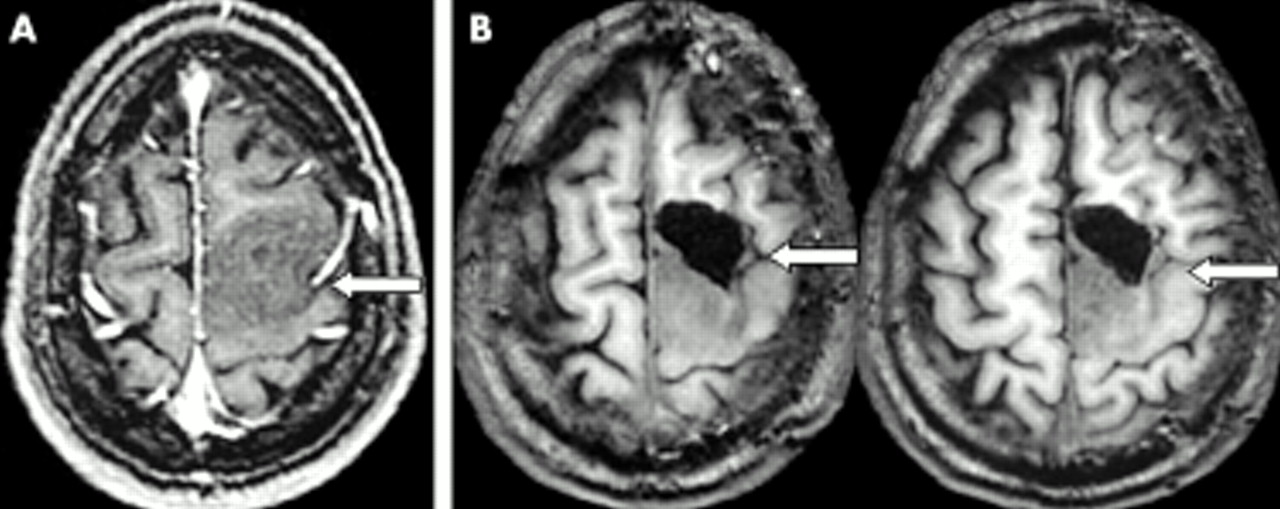
(A) Preoperative axial T1-weighted magnetic resonance imaging (MRI) scan, showing a left precentral low grade glioma invading the dominant superior frontal gyrus (series 1). (B) Postoperative axial T1-weighted MRI, after a surgery performed without intraoperative electrical mapping, showing the resection of the anterior part of the tumour, with a residue in contact with the primary motor area posteriorly. Arrow: precentral sulcus.

{kind=link}
{kind=link}
(A) Preoperative axial T1-weighted magnetic resonance imaging (MRI) scan, showing a similar left precentral low grade glioma invading the dominant superior frontal sulcus (series 2). (B) Postoperative axial T1-weighted and fluid attenuated inversion recovery (FLAIR)-weighted MRI, after a surgery performed with intraoperative electrical mapping, showing total resection of the tumour—the cavity coming into contact with the primary motor area posteriorly, identified by stimulations. Arrow: precentral sulcus.
Of the tumours not invading eloquent areas, 29% were near functional regions in S1 versus 32.7% in S2 (not significant), whereas 36% were remote from eloquent areas in S1 versus 5% in S2 (p<0.0001). There was no significant difference between the groups with regard to preoperative tumour volumes (p = 0.09) (see table 1 for details).
Surgical findings
In S2, intraoperative electrical mapping was used for the removal of all tumours located within and near eloquent areas (95% of cases). Only six resections were performed without stimulation in this series. In all 116 surgeries with mapping, the stimulations allowed detection of the eloquent cortico-subcortical areas, systematically used as boundaries of the resection. However, the mean duration of surgery was longer in S2 (five v three hours in S1) and the incidence of bone flap infection was 0.86% (1/116) in S2.
Postoperative neurological results
In S1, mortality was 2%, and 17% with a severe permanent deficit were in group II (see table 1). In S2, there were no deaths, and 6.5% of patients with severe sequelae were in group II (p<0.019, two tailed test) (figs 1B and 2B).
Postoperative radiological results
The difference between the quality of resections as evaluated on the postoperative control MRI in SI and S2 (see table 1) was statistically significant (p<0.001).
Histological results
On histopathological examination, a low grade glioma (WHO grade II) was diagnosed in all patients in both series.
Survival
Based on the quality of resection, mortality in the two series was as follows.
-
Series 1 (p = 0.04)
– Partial resections: 30/57 (52.6%), median follow up 72 months
– Subtotal resections: 13/37 (35%), median follow up 87 months
– Complete resections: 0/6 (0%), median follow up 75 months
-
Series 2 (p = 0.02)
– Partial resections: 6/29 (20.6%), median follow up 49 months
– Subtotal resections: 5/62 (8%), median follow up 45 months
– Complete resections: 0/31 (0%) median follow up 48 months
DISCUSSION
Recent literature reveals a more frequent use of intraoperative electrostimulation mapping during tumour surgery in eloquent brain areas, in particular for poorly demarcated lesions such as infiltrative LGGs.1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21 However, this method still remains controversial25 first, because of the alternative use of intraoperative electrophysiological monitoring techniques (evoked potentials) proposed by several authors24,34; second, since it is necessary to perform the surgery under local anaesthesia to allow language mapping; and third, because of the recent development of neurofunctional imaging, which can be integrated into a neuronavigation system.35
We believe that none of these criticisms is really well founded, since (a) evoked potentials do not allow the mapping of language and other cognitive functions, (b) good tolerance of awake craniotomies has been well demonstrated,36–39 (c) neurofunctional imaging still lacks reliability, especially with regard to language mapping.40,41 In fact, the real problem seems to be that only few studies have compared the results of surgery without and with the use of DES to evaluate the exact contribution of intraoperative electrostimulation.23,24 Moreover, in these rare reports, the impact of DES and other methods, such as somatosensory evoked potentials and/or neuronavigation, has been evaluated together,23,24 so it is difficult to assess the exact role of sole DES. Also, in these studies, intraoperative motor mapping was done only during tumour surgery within the central region and language mapping was not reported (except in rare series of dominant temporal lobectomies in epilepsy surgery,22 which present not exactly the same problem as in surgery for infiltrative cortico-subcortical gliomas). Finally, the tumours operated on have not all been the same, since the recent series of Reithmeier et al23 included not only low and high grade gliomas but also metastasis and meningiomas.
In the present study, we included a uniform consecutive sample to try to quantify the impact of DES during surgery of supratentorial LGGs, whatever their location, on (a) surgical indications, (b) functional results, and (c) quality of tumour resection.
Extension of surgical indications
Although surgery for infiltrating LGGs has been the subject of much controversy in the literature,42 a growing number of recent series have provided evidence for the favourable impact of resection on the natural history of this kind of lesion.43–45 Consequently, a patient who is not selected for resective surgery for technical reasons (for example, the location of the lesion) by a team which performs surgical resection for LGGs, if the tumour is in fact “operable”, could potentially lose the chance of a favourable outcome.
In our experience, the definition of “operability” significantly changed between the first and the second series, since 62% of LGGs resected in S2 were located within eloquent areas, whereas only 35% of LGGs involved functional regions in S1. Indeed, during the earlier period, there were patients in whom surgical resection was not considered an option: this was typically the case for insular LGGs, which were almost never removed in S1, being documented as “inoperable”. However, we must point out the fact that the extension of surgical indications in S2 was partly due to the following confounding factors:
-
evolution of the management of LGGs in the last decade, favouring aggressive treatment rather than a “wait and see” attitude, due to a better knowledge of the natural history—in particular with regard to the high risk of anaplastic transformation leading to death43–45
-
development of preoperative neurofunctional imaging techniques, which allow better prediction of the individual functional surgical risk and improved surgical planning46
-
improvement of the surgeon’s experience, with a tendency towards “hyper-specialisation” in the second period, and thus a slight modification of the population of patients treated at our institution in S2 as reflected in the lower rate of LGG surgeries remote from eloquent regions.
Nevertheless, it seems that the use of intraoperative DES itself has had an actual impact on the modulation of our criteria of “operability”. First, these methods of intraoperative mapping permit identification and preservation of the functional areas at each moment and each site of the resection. Thus, surgery within the eloquent area is not much more difficult than in “non-eloquent” regions, since the boundaries of the resection are defined in real time using objective and not subjective individual functional data. Second, DES has allowed us to understand better the pathophysiology of eloquent areas in which surgery was rare until recently—despite the fact that LGGs are often located in these areas, such as the insular lobe.47,48 Indeed, an increase in the knowledge of the functional role of the critical brain regions using DES has permitted us to perform surgery in these structures with minimal risk.49–51 Third, DES allows the study of individual plasticity,52,53 a brain potential often described in functional compensation in patients harbouring an LGG, thus leading to an extension of the limits of resection in eloquent areas without induction of permanent deficit.29,54
Improvement of postoperative functional results
Taking into account the fact that an LGG is usually revealed by seizures, in young patients leading an active social–professional life with a normal neurological examination or only a slight deficit, surgery should be considered on the sole condition that the risk of inducing a permanent deficit is low.
Clearly, in our experience, DES has significantly decreased the rate of sequelae (6.5% in S2 v 17% in S1), despite a higher number of surgeries performed within eloquent areas in S2. Indeed, the rest of the surgical methodology was the same in both series, and we did not use neurofunctional imaging data intraoperatively, integrated into an image-guided surgery system, even in S2.
Interestingly, our results are similar to those reported in the literature. In series where intraoperative electrical mapping was not used, the rate of sequelae ranged from 13% to 27.5%, with a mean of 19%,55–62 which is comparable to the results of our S1. In contrast, the rate of postoperative severe permanent deficit reported in the many studies describing the use of DES during surgery of LGG was quite similar at around 4%, again close to our experience (S2). These comparisons are important since they show that DES represents a reliable and reproducible technique with consistent good results—whichever surgical team performs the resection (even in different countries). Our review covers 834 patients operated on for a glioma, including 358 LGGs, in 21 different neurosurgical departments distributed in nine countries (table 2).1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21
Permanent neurological deficit reported in the literature following surgery of gliomas performed using intraoperative electrical mapping
Furthermore, intraoperative electrical mapping excludes neither simultaneous electrophysiological monitoring by evoked potentials nor integration of preoperative neurofunctional imaging data in an image-guided system.15,23 On the contrary, cortical DES may allow validation of positron emission tomography (PET), magnetoencephalography (MEG), functional (f)MRI, and even the recent method of fibre tracking by diffusion tensor imaging.63
Improvement of the quality of resection
Since intraoperative DES allows individual identification of the cortical and subcortical eloquent structures, it seems logical to perform a resection according to functional boundaries. Indeed, we suggest continuing the resection until after the functional structures are detected by DES, and not stopping before, in order to optimise the quality of resection without increasing the risk of inducing postoperative permanent deficit.
This surgical strategy based on the extensive use of DES during the resection, in our experience has significantly improved the quality of LGG removal. Only 37% of resections were defined as subtotal and 6% as total on postoperative MRI in series 1, whereas 50.8% of resections were subtotal and 25.4% total in series 2—despite a higher number of surgeries within the critical areas—with a parallel decrease of the rate of sequelae.
Moreover, whereas extensive surgery is still controversial in LGG, the series’ supporting the positive impact of such a surgical strategy argue that this benefit seems directly related to the quality of resection.1,43,45 Our present oncological results provide the basis for strong arguments in this direction, since the rate of deaths was significantly decreased in cases of subtotal and total glioma removal, in comparison with partial removal. Interestingly, this observation was true for both our series (median follow up: S1 77 and S2 47 months) even though there were more patients with a complete or subtotal resection in S2.
CONCLUSIONS
The present work allows for the first time quantification of the contribution of intraoperative DES during LGG resection. Indeed, our results show that the use of this method leads to:
-
extension of indications of LGG surgery within eloquent areas
-
decrease of the risk of sequelae
-
increase of the quality of tumour resection itself, with an impact on survival.
Thus, DES seems to represent a valuable adjunct to LGG surgery based on the premise that only radiologically total or subtotal resection has a positive impact on the natural history of these tumours.
REFERENCES
Footnotes
-
Competing interests: none declared