Article Text

Abstract
Objectives The natural course of idiopathic normal pressure hydrocephalus (iNPH) has not been thoroughly studied. The consequences of postponing shunt treatment are largely unknown. We aimed to describe the effects of waiting for more than 6 months before surgery and to compare the outcome with that seen in patients who waited for less than 3 months.
Methods 33 patients (iNPHDelayed) underwent an initial investigation (Pre-op 1), followed by re-examination, just prior to surgery, after waiting for at least 6 months (Pre-op 2). Outcome was evaluated after 3 months of treatment. 69 patients who were surgically treated within 3 months after Pre-op 1 and who were also evaluated after 3 months of treatment constituted a comparison group (iNPHEarly). Evaluations were done with the iNPH scale and the modified Rankin Scale (mRS). iNPHDelayed patients were prospectively studied with regard to outcome, whereas the comparison group iNPHEarly was defined and analysed retrospectively.
Results iNPHDelayed patients deteriorated significantly during their wait for surgery, with progression of symptom severity ranging from +7 to −47 on the iNPH scale, and from 0 to +3 on the mRS (both p<0.001). The magnitude of change after surgery was similar in the groups, but since the symptoms of iNPHDelayed patients had worsened while waiting, their final outcome was significantly poorer.
Conclusions The natural course of iNPH is symptom progression over time, with worsening in gait, balance and cognitive symptoms. This deterioration is only partially reversible. To maximise the benefits of shunt treatment, surgery should be performed soon after diagnosis.
- NEUROPSYCHOLOGY
- NEUROSURGERY
- CLINICAL NEUROLOGY
- DEMENTIA
- CSF DYNAMICS
Statistics from Altmetric.com
Introduction
Idiopathic normal pressure hydrocephalus (iNPH) afflicts 1%–3% of community dwelling elderly persons.1 ,2 The condition is underdiagnosed, and the majority of those who might benefit from treatment are never identified as iNPH patients.3–5 The clinical picture is dominated by cognitive decline, gait and balance impairment, and urinary incontinence. The condition has an insidious onset and a gradual progression. The symptoms are mitigated by shunt surgery with a positive response in as many as 84% of the cases in a recent multi-centre study,6 although they are only reversible to some extent. Hypothetically this indicates that the pathophysiology of iNPH gives rise to irreversible damage, and suggests that early detection followed by treatment with as little delay as possible may be important.
The natural course of iNPH has not been thoroughly studied. One single randomised controlled trial (RCT) of the effects of shunting versus postponed treatment (ligated shunts) in patients with probable iNPH who had negative findings on supplemental tests (Rout and cerebrospinal fluid (CSF) Tap) and extensive white matter lesions consistent with Binswanger's disease has unequivocally shown that shunting is beneficial, whereas non-shunting is not.7 Apart from this study, with less typical iNPH patients, no RCTs have been conducted.8 Most of those who work with iNPH patients feel no need for further evidence of the benefits of shunting, and would find themselves in an ethically awkward position asking patients if they would be willing to take a 50% risk of receiving the proper treatment later than possible for study purposes.
As a consequence, knowledge of the natural course of iNPH is imperfect. A review on the topic was published in 2011,9 including six studies with 102 patients altogether, ranging from n=9 to 26. Four of the studies required positive findings on supplemental tests such as measurements of intracranial pulse pressure amplitudes,10 continuous intracranial pressure (ICP) above specified level and registration of A- and B-waves,11 resistance to outflow and continuous ICP above specified level,12 and continuous intraventricular ICP or A- or B-waves and/or resistance to outflow above specified frequencies/levels13 in order for patients to be surgically treated. Patients who did not fulfil these supplemental criteria were followed and compared with the treated patients. However, such comparisons are biased due to the fact the groups differ along dimensions that are, at least in theory, characteristic and important in iNPH. There is also a risk that the patients who were not subjected to surgery might have been suffering from other, iNPH-mimicking, conditions. The two remaining studies followed patients selected for surgical treatment who either declined or were still on the waiting list for surgery. The first of these two studies followed nine patients every 6 months, describing worsening in cognitive impairment in eight at 12 months follow-up and deterioration in gait score in three.14 The second study re-examined 14 unshunted iNPH patients 3–4 months after diagnosis and found deterioration in global ratings and gait score in nine.15
Recently, the waiting time at our hospital (Sahlgrenska University Hospital in Gothenburg) for surgery for patients with a diagnosis of iNPH has been very long, in the worst cases 2 years. This situation was created by economic and administrative failure, causing a lack of accessible operation theatres, staff and ward capacity, forcing parts of non-acute surgery to be postponed.
As a consequence of their wait, several patients who had already undergone preoperative investigations had to be re-examined for the later evaluations of treatment effects to be just. Thus, for regrettable reasons, we have been provided with an opportunity to learn more about the natural course of iNPH.
The aim of this study was to describe if, how much and in which symptom domains patients with iNPH change during a waiting time of 6–24 months. We also wished to compare the postoperative results of waiting patients with iNPH patients who had shunt surgery performed within 3 months from diagnosis.
Patients and methods
All 35 iNPH patients scheduled for shunt surgery between the 5 March 2011 and the 31 December 2011 who had been on the waiting list for more than 6 months were evaluated. Two could not be scheduled for re-examinations prior to surgery, which is why 33 were included in the study, constituting the group referred to as iNPHDelayed.
The waiting list for elective surgery is primarily based on the dates of referrals and/or preoperative investigations. The queue order may be changed if patients are differently prioritised. Among iNPH patients such changes may be based, for instance, on information about frequent falls.
All patients were informed about their right to turn to other neurosurgical clinics for treatment. They were also offered assistance in their contacts with other hospitals. However, during this period there was limited neurosurgical capacity in other hospitals also and only five patients were treated elsewhere. In 2011, measures were taken to diminish the queues for surgery, which explains the higher frequency of surgery during this year.
All patients referred to our NPH unit for investigation of suspected iNPH are, if they accept, included in a local hydrocephalus register. To form a contrast group to iNPHDelayed, we wanted to find patients with a reasonable waiting time, defined as less than 3 months. We extracted data from the local hydrocephalus register for all patients who were diagnosed with iNPH between 15 October 2004 and 6 November 2012. There were 178 patients. Out of these, we selected all patients who had shunt surgery within 3 months from diagnosis (n=69), from here on referred to as iNPHEarly.
Among the remaining 109 patients, 93 had waited for more than 3 months before surgery (including the 35 mentioned above), 14 patients had not undergone shunt surgery (five newly diagnosed patients awaiting surgery, four patients who had declined and five patients who died before surgery) and, finally, two patients had not yet been evaluated postoperatively.
The diagnosis of iNPH (for all patients in both groups) was based on clinical and radiological (MRI or CT) findings compatible with possible or probable iNPH.16
They were examined by a neurologist, a neuropsychologist and a physiotherapist. These examinations were made preoperatively at time for diagnosis (Pre-op 1), and 3 months after surgery (Post-op) for both groups. In addition to this, the iNPHDelayed patients were re-examined just prior to surgery (Pre-op 2).
Symptom severity was assessed with the recently published iNPH scale.17 The iNPH scale score is the weighted mean score of assessments in the four domains of gait, neuropsychology, balance (static) and continence. The gait and neuropsychology domain scores represent the mean of converted scores on three and four separate tasks, whereas the balance and continence domains are covered by ordinal scales. The iNPH scale at large, referred to as total iNPH scale score, and the separate domain scores all have a minimum–maximum range from 0 to 100, where 100 represents normal performance among healthy individuals in an iNPH typical age range of 70–74 years. A significant change in the total iNPH scale score is defined as >5 points.
Our primary outcome measures were the total iNPH scale score and the modified Rankin Scale (mRS).18 ,19 Secondary outcome measures were the domain scores (gait, neuropsychology, balance, continence) of the iNPH scale and the Mini-Mental State Examination (MMSE).20
Risk factors for cerebrovascular disease (hypertension, cardiovascular disease and diabetes) were registered.
Pre-op 1 data of the two patient groups are presented in table 1.
Demography and clinical findings at Pre-op 1 for iNPH patients who subsequently waited for surgery for more than 6 months (iNPHDelayed) and for patients waiting less than 3 months (iNPHEarly)
The study was approved by the Regional Ethical Review Board in Gothenburg (Dnr 009-13).
Statistics
Non-parametric statistical methods were used in all analyses. The Wilcoxon signed ranks test was used for within-group comparisons and the Mann–Whitney U test for comparisons between groups. The χ2 test (or Fisher's exact test when more appropriate) was used for comparing proportions. The Spearman rank correlation coefficient (r) was used to estimate associations between variables. Statistical analyses were performed with IBM SPSS V.20.0 for Windows.
Results
Pre-op 1
The median waiting time before surgery was 13.2 months for iNPHDelayed patients and 6 days for iNPHEarly. iNPHDelayed patients were older (p<0.05) and had a larger proportion of patients with hypertension (p=0.014). Apart from this, there were no statistically significant differences between the groups on the variables presented in table 1, that is, symptom severity was equal across the groups.
Changes between Pre-op 1 and 2
The iNPHDelayed patients deteriorated in median 8 points (23%) on the iNPH scale during the waiting period (p<0.001). For 55% of the patients, the total score on the iNPH scale decreased ≥5 points. The deterioration in the domains is shown in table 2 along with changes in mRS and MMSE.
Results from preoperative and postoperative examinations and comparisons across assessments and across groups. iNPHDelayed (n=33) waited for surgery for more than 6 months and therefore had two preoperative examinations (Pre-op 1 and Pre-op 2), whereas iNPHEarly (n=69) had shunt surgery within 3 months following the initial assessment (Pre-op 1)
The magnitude of change on the total iNPH scale score ranged from an improvement of 7 points to a decrement of 47 points during the waiting time. There were no significant correlations between the changes and age, sex, comorbidity or waiting time. There was no significant relationship between entrance scores and the magnitude of decline; that is, splitting the iNPHDelayed group at the median value for magnitude of decline created two halves that were not significantly different from each other with regard to scores in the separate domains at Pre-op 1. The individual trajectories are presented in figure 1.

Individual changes on the iNPH scale total score in the iNPHDelayed group (n=33) during the waiting time before surgery (median 13 months). The bold line represents median values iNPH, idiopathic normal pressure hydrocephalus.
Median mRS changed from 2 to 3 (p<0.001) during the waiting period. In all, 55% were able to live independently (mRS 0-2) at Pre-op 1 in comparison with 39% at Pre-op 2 (p<0.001). Five patients became severely disabled while waiting for surgery.
The median performance on the MMSE decreased from 25 at Pre-op 1 to 22 points at Pre-op 2 (p<0.01).
Postoperative follow-up in iNPHEarly
In the iNPHEarly group, two patients died before follow-up and two were lost to follow-up, leaving 65 patients for evaluation.
A total of 54 patients improved ≥5 points following surgery: an improvement rate of 78% according to an intention-to-treat analysis (ITT) and 83% when evaluated per protocol (PP). The PP median improvement was 12 points (25%; p<0.001).
The patients were significantly improved in mRS scores (p<0.001). The proportion of patients able to live independently (mRS 0–2) increased from 59% to 80%. The median results on the MMSE increased from 25 to 27 (p<0.001).
Comparisons between Pre-op 2 and Post-op in iNPHDelayed
In the iNPHDelayed group, one patient died before surgery, four died after the operation but before the 3-month evaluation and one was lost to follow-up, leaving 27 for postoperative evaluation.
The ITT improvement rate was 48% (59% PP) with a PP median improvement of 11 points (26%) on the iNPH scale (p<0.001).
The patients were significantly improved in mRS scores (p<0.05). The proportion of patients able to live independently (mRS 0–2) increased from 39% to 48%. The median results on the MMSE increased from 22 to 25 (p<0.01).
Comparisons between treatment effects in the two groups
The magnitude of score improvements (from Pre-op 1 in iNPHEarly and from Pre-op 2 in iNPHDelayed) did not differ significantly between the two groups, neither when expressed as raw scores nor as percentages. The ITT improvement rate in the iNPHEarly group was significantly higher than among iNPHDelayed patients (p<0.05), whereas the difference between the PP improvement rates was not statistically significant (p=0.082).
At follow-up, the iNPHEarly patients had less severe symptoms than iNPHDelayed according to the total score on the iNPH scale (medians 67 and 55; p=0.01). The groups also differed with regard to three of the separate domains (Gait: p=0.006, Neuropsychology: p=0.03, Balance: p=0.048, but Continence p=0.176).
Comparisons between Pre-op 1 and Post-op in iNPHDelayed
Fourteen of the patients in the iNPHDelayed group improved ≥5 points on the iNPH scale compared with Pre-op 1, corresponding to an ITT improvement rate of 42% (PP 52%). The PP median increase on the iNPH scale of 6 points (11%) was not statistically significant, nor were there significant changes on mRS or MMSE. The proportion of patients able to live independently (mRS 0–2) decreased from 55% to 48%.
The magnitude of improvement was significantly smaller in iNPHDelayed (from Pre-op 1 to Post-op) compared with iNPHEarly with regard to the iNPH scale total score, and mRS (p<0.01) but not the MMSE. The improvement rates (ITT as well as PP) were also significantly smaller in iNPHDelayed patients (p<0.001 and p=0.002).
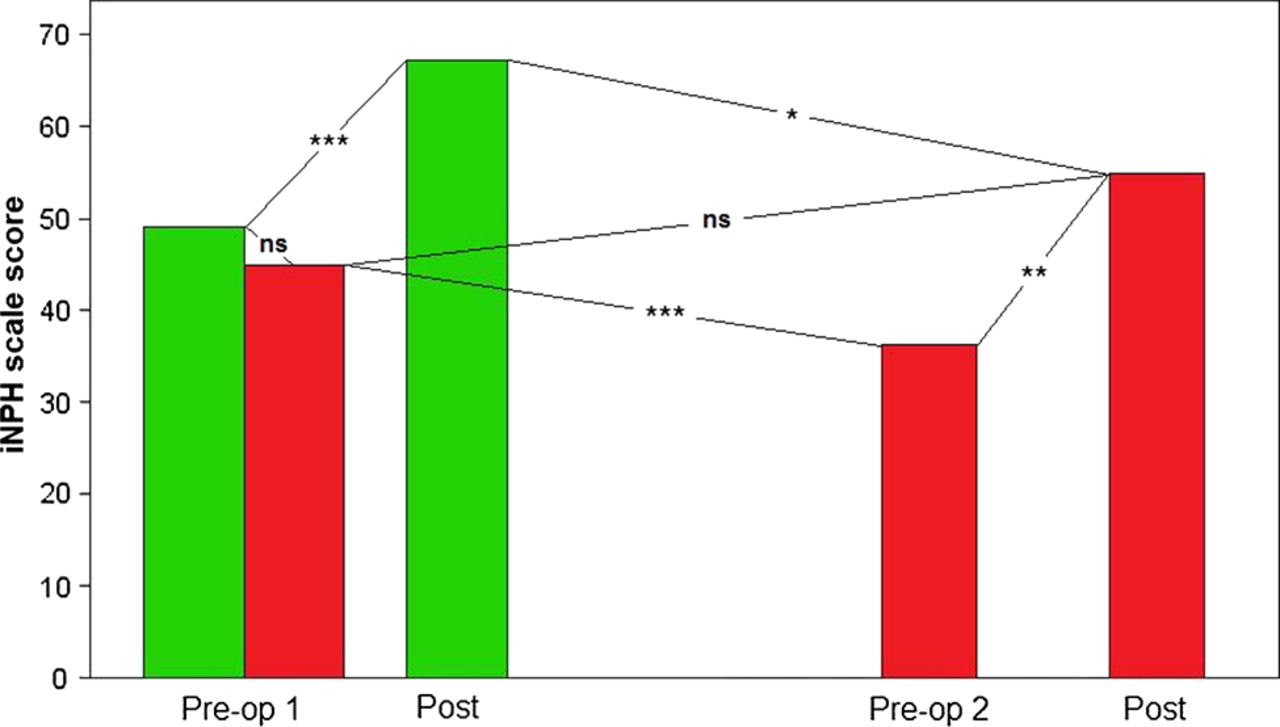
Results from the different assessments and comparisons between them are presented in table 2, and the iNPH scale results and changes found in the study are graphically summarised in figure 2.

{kind=link}
{kind=link}
Light grey bars represent median iNPH scale results of patients who were examined and diagnosed (at Pre-op 1), treated within 3 months, and subsequently followed-up after 3 months of shunt treatment (at Post-op) (iNPHEarly; n=69). Dark grey bars represent patients who waited for surgery for more than 6 months after the initial examination (again at Pre-op 1) and who were therefore re-examined before the operation (at Pre-op 2) and subsequently followed-up after 3 months (extreme right Post-op) (iNPHDelayed; n=33). *p<0.05, ** p<0.01, ***p<0.001. iNPH, idiopathic normal pressure hydrocephalus.
Discussion
This study shows that symptoms progress over time in unshunted iNPH patients. During a median of 13 months the 33 iNPH patients deteriorated 23% on the total iNPH scale score, with significant decline in gait, balance and cognitive abilities.
Our results are in agreement with earlier studies by Razay et al,15 showing moderate or marked worsening at 3 months’ follow-up in 14 unshunted patients, and Scollato et al,14 finding deterioration in gait, cognition and bladder continence in nine patients. Out of the six studies reviewed by Toma et al9 concerning the clinical course for unshunted possible iNPH patients, four had confounding factors, as stated already in Introduction section.10–13 Of the 23 patients in the remaining two studies, there were 19 who refused shunt surgery.14 ,15 With this approach there might also be confounders, such as comorbid conditions, which would make patients less willing to take the risk of surgery. Our study group is unique since it includes only patients who were selected for, and accepted, shunt treatment, but also because most of our patients subsequently received treatment and benefitted from it.
The large variability of symptom progression during waiting time — from slight improvement to a marked decline in abilities (iNPH scale score dropping at worst from 51 to 5 points) — was less expected. Theoretically, such variations may be presumed to be due to day-by-day fluctuations, measurement error, differences in waiting time, differences in progression rates caused by the characteristics of the iNPH itself or presence of comorbidity. Analyses did not show any significant associations between progression rate and waiting time, nor between progression rate and sex or age. Thus, there is no question that iNPH patients as a group worsen over time regarding iNPH symptoms if not treated, but what sets the pace for individual patients is uncertain.
This study rests on a set of data created by unwanted circumstances that we hope will never occur again. All patients referred for surgery were placed on the waiting list and subsequently treated. Hence, we consider the group of iNPHDelayed to be representative for iNPH patients and the description of their disease progression, the natural course, to be valid beyond this sample.
Except for the analysis of the natural course of iNPH in untreated patients, we also aimed to compare their outcome after surgery to that of patients who received their treatment without delay. Retrospectively defining an early operated reference group, we realised that it was not possible to match retrospective controls regarding age from our database. Therefore, to be as accurate as possible given the situation, we chose instead to include all patients with a normal waiting time. The control group was examined according to the same protocol as the iNPHDelayed patients. The groups were similar with regard to symptom severity at Pre-op 1 and most of the background data, except for age and frequency of hypertension (see table 1). We consider these two inequalities the major limitations of the study. The reason why the average age is higher in iNPHDelayed is unclear. It has never been the intention of the hospital or the research team to prioritise younger patients, but it could be that younger patients and their relatives have been more eager to report signs of progression and to stress the risks associated with further delay, thereby influencing the surgery schedule.
Importantly, however, age was in no instance associated with the magnitude of change in neither of the two groups, that is, age was not significantly correlated with the deterioration in iNPHDelayed between Pre-op 1 and 2, nor with the improvement from most recent examination to Post-op in any of the groups, when analysed separately or together.
Hypertension, which was more frequent in the iNPHDelayed group, is a risk factor for cerebrovascular comorbidity which, in turn, may aggravate the symptomatology of iNPH but also hamper the effect of shunt treatment. Neither could be shown to be the case in this study. There were no statistically significant differences between patients with or without hypertension in the comparisons of symptom severity at any of the examinations, or with regard to the magnitude of changes between the examinations.
All patients were examined according to protocols of routine care. This means that the examiners were not blind to the waiting time of patients, or to whether they had undergone surgery or not. It would not have been possible to do otherwise, partly because the whole group of iNPHEarly were identified retrospectively and partly since the iNPHDelayed patients were included during a limited time period. The intention of all investigations of these patients has been to provide as good care as possible, given the circumstances.
The magnitude of improvement after surgery did not differ between iNPHDelayed and iNPHEarly in a PP analysis, which shows that reversibility even late in the course is characteristic in iNPH.
Still, and more importantly, what is also shown is that the final outcome is strongly linked to the level of severity reached before surgery. First, there was a considerably larger improvement rate in the iNPHEarly group, when estimated by ITT analysis (78% vs 48%), which is mostly due to the fact that more iNPHDelayed patients died before follow-up. Our interpretation is that the waiting rendered these patients more fragile because of increasing age and disease progression (both iNPH and comorbid conditions). Second, the condition after 3 months after surgery is significantly worse when surgery is delayed. The implication of this is crucial; keeping iNPH patients on a waiting list for shunt surgery will allow further progression to set continuously harsher limits on the functional capacities that remain after surgery. The proportion of patients able to live independently, mRS 0–2, was considerably larger in the iNPHEarly group, 48% versus 80%. This should have a considerable impact on the lives of the patients and their families, and on societal costs.
Several authorities, including the Cochrane institute, have questioned the effect of shunting iNPH patients due to the lack of proper RCTs in the field. The NPH society has repeatedly discussed conducting an RCT on the effect of shunt surgery but many physicians have objected to this, referring to the obvious effect shown in many studies, for example, the previously mentioned study by Tisell et al7 and the recent European multi-centre study.6 Our study further substantiates this effect, besides confirming deterioration in unshunted patients.
This study confirms an improvement rate of around 80% after shunting (78% ITT; 83% PP) concerning the control group of early operated patients, as seen in the European study mentioned above.6
Conclusions
The natural course of iNPH is symptom progression over time, with worsening in gait, balance and cognitive symptoms. This deterioration is only partially reversible. To maximise the benefits of shunt treatment, surgery should be performed soon after diagnosis.
Acknowledgments
We wish to express our gratitude to the patients and staff at the Hydrocephalus Research Unit without whom this study would not have been possible. Special thanks go to Gunilla Ahl-Börjesson for assistance in extracting the data, and to Gudrun Barrows who coordinated supplementary examinations for long-waiting patients.
References
Footnotes
-
Contributors KA: design and conceptualisation of the study, compilation, analysis and interpretation of the data, drafting and revising the manuscript. CW: design and conceptualisation of the study, interpretation of the data, drafting and revising the manuscript. MT: design and conceptualisation of the study, interpretation of the data, revising the manuscript. PH: design and conceptualisation of the study, analysis and interpretation of the data, drafting and revising the manuscript, performed the statistical analyses.
-
Competing interests CW receives honorarium for lecturing and consulting by Codman, Johnson & Johnson and Likvor AB. The other authors declare no conflicts of interest.
-
Ethics approval Regional Ethics Board of West Sweden, Gothenburg.
-
Provenance and peer review Not commissioned; externally peer reviewed.