Article Text

Abstract
Introduction We performed a meta-analysis to synthesise current evidence on amyloid-positron emission tomography (PET) burden and presumed preferential occipital distribution in sporadic cerebral amyloid angiopathy (CAA).
Methods In a PubMed systematic search, we identified case–control studies with extractable data on global and occipital-to-global amyloid-PET uptake in symptomatic patients with CAA (per Boston criteria) versus control groups (healthy participants or patients with non-CAA deep intracerebral haemorrhage) and patients with Alzheimer’s disease. To circumvent PET studies’ methodological variation, we generated and used ‘fold change’, that is, ratio of mean amyloid uptake (global and occipital-to-global) of CAA relative to comparison groups. Amyloid-PET uptake biomarker performance was then quantified by random-effects meta-analysis on the ratios of the means. A ratio >1 indicates that amyloid-PET uptake (global or occipital/global) is higher in CAA than comparison groups, and a ratio <1 indicates the reverse.
Results Seven studies, including 106 patients with CAA (>90% with probable CAA) and 138 controls (96 healthy elderly, 42 deep intracerebral haemorrhage controls) and 72 patients with Alzheimer’s disease, were included. Global amyloid-PET ratio between patients with CAA and controls was above 1, with an average effect size of 1.18 (95% CI 1.08 to 1.28; p<0.0001). Occipital-to-global amyloid-PET uptake ratio did not differ between patients with CAA versus patients with deep intracerebral haemorrhage or healthy controls. By contrast, occipital-to-global amyloid-PET uptake ratio was above 1 in patients with CAA versus those with Alzheimer’s disease, with an average ratio of 1.10 (95% CI 1.03 to 1.19; p=0.009) and high statistical heterogeneity.
Conclusions Our analysis provides exploratory actionable data on the overall effect sizes and strength of amyloid-PET burden and distribution in patients with CAA, useful for future larger studies.
- PET
- cerebral amyloid angioapathy
- intracerebral hemorrhage
- cerebralmicrobleeds
Statistics from Altmetric.com
Introduction
Sporadic cerebral amyloid angiopathy (CAA), a common degenerative small vessel disease of the brain, has received increasing attention in the stroke community due to its growing prevalence, clinical relevance and implications for antithrombotic decision-making.1 CAA is associated with cerebrovascular brain injury (both haemorrhagic and ischaemic) in older individuals and is an important contributor of spontaneous lobar intracerebral haemorrhage (ICH) as well as dementia.2 3 The pathological hallmark of the disease is progressive amyloid-β deposition affecting the cortical and leptomeningeal vessels. There is currently no specific disease-modifying treatment for CAA, but efforts are ongoing for early-phase trials (NCT01821118) with candidate approaches including inhibition of amyloid-β production and enhancement of its clearance.4
Despite an expanding spectrum in CAA MRI signatures, which are useful and commonly used for diagnosis within the validated Boston criteria (eg, strictly lobar cerebral microbleeds, cortical superficial siderosis),5 6 direct and early markers of vascular pathophysiology remain a key unmet need in the field. This, in part, is a potential barrier for large-scale clinical trials in the prevention or treatment of CAA. The approach of using CAA MRI lesions of brain focal damage is, by definition, limited in detecting non-specific indirect consequences of rather advanced CAA (ie, after the appearance of multiple haemorrhagic MRI markers).7 Positron emission tomography (PET) scanning with the amyloid radiotracer 11C-Pittsburgh compound B (PiB-PET) or 18F-florbetapir (florbetapir-PET)8 has been suggested to quantify the burden and distribution of cerebrovascular (in addition to parenchymal) amyloid-β deposits.9 10 PET-based amyloid imaging might be more closely representative of CAA’s underlying biology than putative MRI markers,11 and thus has been suggested as a potential diagnostic biomarker or even a surrogate marker in disease-modifying trials, to be validated and explored in future studies.4 However, most studies on amyloid PET biomarker validity in CAA include small numbers of participants and vary in methods. No comprehensive meta-analysis has assessed the overall performance and effect size of this promising method in quantifying CAA.
We therefore performed a systematic review and meta-analysis to synthesise evidence on the overall strength of amyloid-PET in patients with symptomatic sporadic CAA versus control groups, in terms of both global cortical amyloid load and occipital-to-global regional distribution, the two main metrics that characterise amyloid PET in CAA suggested in the literature.12 Regarding comparison groups, we considered the recently proposed two-pronged diagnostic approach involving comparison to both healthy aged or deep non-CAA-related ICH controls, and subjects with probable Alzheimer’s disease (AD).12 13
Methods
This study was conducted in line with the Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy14 15 and with reference to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement, according to a prespecified protocol developed in-house and following a recentl systematic review on the topic.12
Search strategy, selection criteria and data extraction
We searched PubMed (without language restriction) from 1 January 2007 (when the first study on amyloid PET in CAA was published) until 12 June 2017 (updating a recent systematic search12) using a combination of keyword search and medical subject heading (MeSH) terms: (PET OR PiB OR pittsburgh OR ‘positron emission tomography’ OR florbetapir) AND (‘amyloid angiopathy’). Reference lists from all included articles, review papers on the topic and the authors’ own files were also searched for relevant studies in English.
We included studies reporting data on brain amyloid PET uptake in patients with symptomatic sporadic CAA versus controls and patients with AD. Sporadic CAA was defined according to the validated clinical-MRI Boston criteria5 16 17 and presented with either symptomatic lobar ICH or transient focal neurological episodes. The control groups consisted of healthy controls or patients presenting with non-CAA-related deep ICH. To be classified as non-CAA-related ICH, patients with deep ICH underwent brain MRI, including blood-sensitive sequences, for assessing cerebral microbleeds and rule out the presence of lobar microbleeds, indicative of CAA.5 A diagnosis of probable AD was given in studies including relevant groups based on the National Institute of Neurological and Communication Disorders-Alzheimer’s Disease and Related Disorders Association (NINCDS-ADRDA) criteria.18 Articles were excluded if they included CAA-related inflammation cases, only asymptomatic CAA cases suspected based on the presence of silent strictly lobar cerebral microbleeds or if they did not contain an appropriate non-CAA control group.
Two authors independently extracted data from all eligible studies on amyloid-PET imaging analysis methods, baseline information on comparison groups (ie, CAA cases, healthy controls, patients with deep ICH and AD), CAA clinical presentation, and reported global and regional amyloid-PET retention data, in distribution volume ratio (DVR) or standard uptake value ratio (SUVR) as applicable, in all groups.
Quality assessment of included studies
The methodological quality of each selected study was assessed using the revised QUADAS-2 (Quality Assessment Tool for Diagnostic Accuracy Studies) tool.19 ,20 21
Theoretical framework for the pooled analysis and statistical synthesis of results
The variability in amyloid-PET performance and assessment between laboratories, including different amyloid-PET tracers, PET imaging protocols, specific reconstruction algorithms and use of DVR versus SUVR, makes a traditional meta-analysis of standard mean differences of quantitative analysis results especially challenging.22 To circumvent these problems, we have adopted the approach of generating fold change, that is, the ratio of the mean amyloid uptake (global and regional separately) between groups of interest. We meta-analysed patients with CAA to control groups and patients with AD ratios for global and occipital-to-global amyloid-PET uptake where possible. Each ratio was generated within each individual study for every comparison of interest. A ratio above 1 indicates that amyloid-PET uptake is higher in the CAA patient population than comparison groups, and a ratio below 1 indicates the concentration is higher in comparison groups.
We consider as control groups to CAA cases both healthy elderly cohorts and elderly patients with hypertension-related deep ICH together, and then separately in sensitivity analyses. Based on a range of neuropathological and imaging data, it is hypothesised that the amyloid profile of elderly patients with deep ICH should be similar to elderly healthy controls, that is, similar incidence of incipient Alzheimer’s and vascular amyloid pathology.23 24 Two different amyloid PET tracers have been tested in CAA cohorts: 11C-PiB and 18F-florbetapir. Our analytic approach of using fold change makes pooling these studies together possible. In addition, the two tracers are expected to provide comparable data in the assessment of amyloid burden in this setting and using fold change, based on the following observations: (1) in vivo there is a perfect linear association between mean global cortical florbetapir-PET retention and PiB-PET uptake in patients with CAA (r=0.96, p<0.001), that is, florbetapir uptake matches the pattern and severity of PiB uptake25; and (2) PiB-PET has been validated against postmortem examination for selectively binding fibrillar amyloid-β.9
The SE of the ratio of the mean amyloid uptake values was calculated with the delta method.26–28 Random-effects meta-analysis with the method of DerSimonian and Laird29 with the estimate of heterogeneity (I2 test) taken from the inverse-variance model was performed in Stata V.13. Overall outcome measures were given as the ratio (effect size) of global cortical amyloid PET uptake between patients with CAA and control cohorts or patients with AD, and occipital-to-global amyloid PET uptake between CAA and AD cohorts, with corresponding 95% CIs. A p value of 0.05 or less was considered significant.
Results
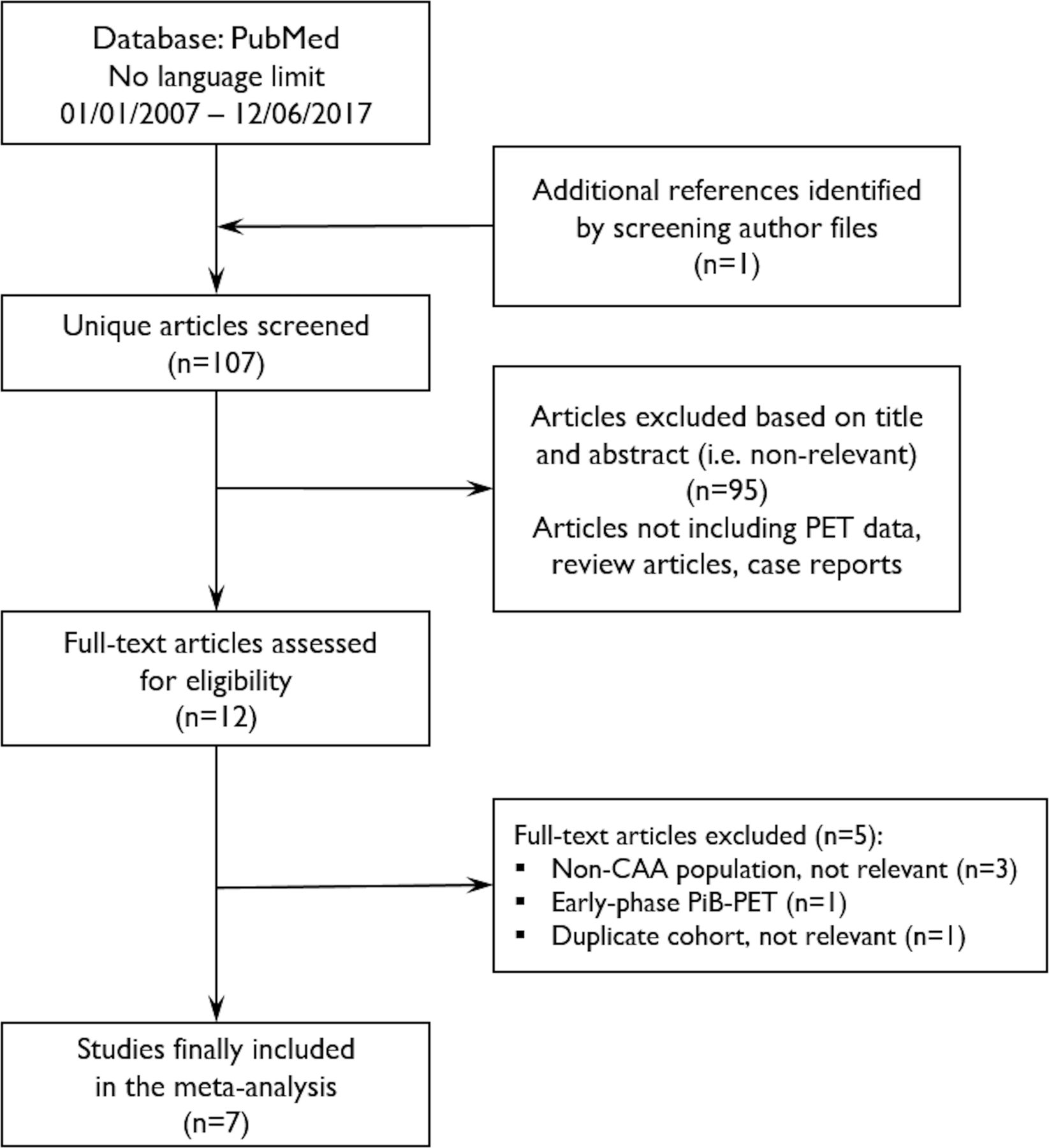
Our systematic search identified a total of 107 unique articles. After reviewing the full text of 12 potentially eligible papers, 7 studies were eligible for inclusion in the meta-analysis (see figure 1 for flow chart). Table 1 summarises key methodological aspects of included studies and relevant characteristics of each group. Five studies used PiB-PET13 30–34 and two studies florbetapir-PET.25 35 36 In all studies brain regions with structural damage were removed from the analysis. In five studies the CAA cohorts comprised only patients presenting with symptomatic lobar ICH,13 25 30 32 35 while the other two studies included different clinical presentations associated with CAA (eg, seizures, cognitive impairment and so on).31 33 Regarding control groups, four studies included healthy controls,13 31–33 while three studies included patients with spontaneous deep ICH presumed due to hypertensive small vessel disease.25 30 35 Patients with spontaneous deep ICH underwent brain MRI with blood-sensitive sequences for cerebral microbleeds assessment. All included deep ICH cases demonstrated no lobar microbleeds (a putative CAA imaging marker)—they were only allowed to have microbleeds restricted to deep brain areas, in line with the distribution of hypertensive arteriopathy. Hence, these patients had strictly deep haemorrhagic lesions, excluding the possibility of underlying advanced CAA.5 Controls had in general no cognitive complaints and normal Mini-Mental State Examination. In one study the cognitive status of health controls was not reported.33 In addition to control groups, three studies included separate AD cohorts,31–33 and in one study13 data on an AD group were available to us (table 1). In these studies, patients met the NINCDS-ADRDA criteria for probable AD.18 No specific details on any other supporting biomarker studies (eg, cerebrospinal fluid analysis) performed in patients with AD were provided in included studies. However, in two13 33 of the four studies that included AD groups, MRIs with blood-sensitive sequences were available and none of the patients with AD had lobar microbleeds to allow a diagnosis of suspected underlying advanced CAA added on AD.6 Table 2 shows the results of the quality assessment. In general, included studies were of moderate-to-high quality, with concerns mainly arising around patient selection, index test/presentation for CAA and report of full data (table 2). One of the studies did not have as primary aim to compare amyloid binding between CAA and control groups.33

Flow chart of study selection in the main literature search. An additional supplementary search in the Web of Science database, using a similar search strategy, did not identify any additional relevant papers eligible for our meta-analysis. In addition, in a search of published abstracts from the International Stroke Conference and the European Stroke Organisation Conference (2014–2017), no other relevant studies were identified. CAA, cerebral amyloid angiopathy; PET, positron emission tomography; PiB-PET, 11C-Pittsburgh compound B-PET.
Characteristics of included studies on amyloid PET imaging in CAA
QUADAS-2 assessment of risk of bias for included studies
The seven studies pooled in meta-analysis included a total of 106 CAA cases (>90% with probable CAA), 138 controls (96 healthy elderly and 42 hypertensive deep ICH controls) and 72 patients with AD. We first meta-analysed data on global amyloid-PET uptake in patients with CAA versus all control groups. The global amyloid-PET ratio between patients with CAA to controls was above 1, with an average value of 1.18 (1.08–1.28) (p<0.0001) (figure 2A). The results of sensitivity analyses on amyloid-PET ratio in CAA versus healthy controls and versus patients with hypertensive deep ICH are shown in table 3. Global amyloid-PET uptake was lower in patients with CAA compared with patients with AD (figure 2B). Second, we meta-analysed reported data for occipital-to-global amyloid-PET uptake. Occipital-to-global amyloid-PET uptake ratio did not differ between patients with CAA and patients with deep ICH or healthy controls (figure 3A and table 3). One florbetapir-PET study did not provide the occipital-to-global uptake, but instead reported that occipital uptake was higher in patients with CAA versus patients with deep ICH after adjusting for global uptake.25 Post-hoc calculation of occipital-to-global amyloid-PET ratio and inclusion of these data in a sensitivity analysis did not change the effect size of our estimates (data not shown). By contrast, occipital-to-global amyloid-PET uptake ratio was above 1 in patients with CAA versus patients with AD, and had an average ratio of 1.10 (95% CI 1.03 to 1.19; p=0.009), but with high degree of statistical heterogeneity as assessed by the I2 test (figure 3B). The pooled results for all comparisons are systematically summarised in table 3.

Forest plot of the main meta-analyses. Patients with CAA to control groups (A) and patients with CAA to patients with AD (B) global amyloid-PET ratios. Individual study ratios and their corresponding 95% CIs are indicated by filled squares. The size of the square indicates the weight of each study. The averaged ratio and 95% CI are indicated by the diamonds. The solid line indicates a ratio of 1, and the dotted line indicates the average ratio for each meta-analysis. A ratio above 1 indicates that amyloid-PET uptake is higher in the CAA patient population than comparison groups, and a ratio below 1 indicates the concentration is higher in comparison groups. AD, Alzheimer’s disease; CAA, cerebral amyloid angiopathy; HC, healthy controls; ICH, intracerebral haemorrhage; PET, positron emission tomography; RoM, ratio of means (ie, fold change, effect size).

{kind=link}
{kind=link}
{kind=link}
Forest plot of the main meta-analyses. Occipital-to-global amyloid-PET ratios in patients with CAA versus control groups (A) and patients with CAA compared with patients with AD (B). Individual study ratios and their corresponding 95% CIs are indicated by filled squares. The size of the square indicates the weight of each study. The averaged ratio and 95% CI are indicated by the diamonds. The solid line indicates a ratio of 1, and the dotted line indicates the average ratio for each meta-analysis. A ratio above 1 indicates that amyloid-PET uptake is higher in the CAA patient population than comparison groups, and a ratio below 1 indicates the concentration is higher in comparison groups. AD, Alzheimer’s disease; CAA, cerebral amyloid angiopathy; PET, positron emission tomography; RoM, ratio of means (ie, fold change, effect size).
Summary of pooled RoM results of the main and subgroup meta-analyses regarding global and occipital-to-global regional assessment of amyloid tracer brain uptake in key comparison groups
Discussion
Our meta-analysis brings together pooled estimates on all available evidence regarding amyloid-PET uptake in CAA, contributing to the rapidly growing biomarker literature in the field. It demonstrates that symptomatic CAA (without dementia) is, at the group level, associated with higher global amyloid-PET burden compared with non-demented healthy controls of similar age and patients presenting with spontaneous deep ICH (related to the other major small vessel disease type, ie, “hypertensive arteriopathy”). Compared with patients with AD, patients with CAA show somewhat intermediate levels of global amyloid-PET retention, with relative occipital predominance. It is important to note that these findings are derived from a limited number of studies and should be considered exploratory and hypothesis-generating.
Amyloid-PET imaging has been an exciting advancement for the CAA field. As recently discussed in a critical review,12 it provided a window to understand the pathophysiological mechanisms of the disease, including the relationship of amyloid burden with important haemorrhagic and non-haemorrhagic MRI manifestations and large-scale brain alterations of CAA. The increased amyloid-PET uptake in patients with symptomatic CAA-ICH demonstrated here is consistent with previous reports, and most likely reflects ligand binding to cerebrovascular amyloid, in line with neuropathological data. Amyloid-PET imaging is thus a unique direct putative molecular biomarker of CAA in vivo, and has been suggested as a candidate surrogate marker for patient selection and monitoring treatment effects in future early-phase anti-amyloid trials in the field by a recent consensus panel of experts.4 One of the hurdles in summarising the totality of evidence on amyloid imaging and thus biomarker utility in CAA studies is the different methods for undertaking and analysing amyloid-PET across sites. We have overcome this variability in our meta-analysis by using ratios of the means (ie, fold change) of CAA to relevant control groups. Of note, the healthy controls used in most included studies were elderly participants (ie, >65 years old), and some of these cases inevitably show substantial amyloid tracer uptake, likely reflecting underlying incipient AD.37–40 This potentially leads to underestimation of the fold change in global amyloid-PET burden when the group of patients with CAA is compared with elderly healthy participants. Only one study13 correctly used an additional sample of young (<55 years of age) healthy controls to avoid this caveat.
Pooled estimates presented here can also inform the discussion on the potential diagnostic utility of amyloid-PET in CAA. The main focus in CAA studies has been on whole cortex average amyloid-PET uptake. Based on global ratio results across studies, amyloid PET imaging can help rule out advanced CAA if negative,13 either compared with healthy controls or with patients with hypertensive deep ICH. However, since amyloid-PET tracers label both cerebrovascular and parenchymal amyloid-β, differentiating CAA from AD is challenging. Based on postmortem data documenting that the occipital lobe is most frequently and severely affected by CAA, higher occipital-to-global amyloid-PET ratio has been adopted in the field as molecular signature of CAA versus AD. Our results show that this concept might be ill-defined, derived only from three studies including a handful of patients, with overall low effect size and high degree of uncertainty. One of the larger PiB-PET studies in CAA33 did not include data on occipital predominance of amyloid tracer retention level in CAA versus AD, which would have been useful to further explore this hypothesis. Furthermore, our meta-analysis showed no significant occipital-to-global predominance of amyloid-PET in CAA versus deep ICH. One study comparing distribution ratios in CAA versus age-matched healthy controls reported no significant differences.13 While the expected difference in amyloid-PET uptake burden and distribution in CAA versus AD is to some degree present, overall we suggest that more definitive conclusions require validation in larger prospective studies. Other regional patterns, including upper convexity amyloid-PET burden11 and early-phase amyloid-PET imaging, should also be studied as they seem to hold promise.41
The main limitation of our meta-analysis is the overall small number of cases derived from convenient samples, reflecting the limited availability of amyloid-PET data in the field. Patients with CAA had different characteristics, disease duration and severity, representing important selection and disease spectrum bias. A key issue intrinsic to amyloid imaging is the possibility of patients with CAA having different burden of cerebrovascular amyloid deposition and incipient AD pathology, and a proportion of elderly healthy controls and patients with deep ICH having incipient AD and/or CAA pathology.13 Within this context, it is important to note that the groups of patients with CAA in the included studies did not have dementia (or significant cognitive impairment) and overall demonstrated less amyloid PET burden compared with the AD populations. However, patients with symptomatic CAA, especially those presenting with lobar ICH, often develop dementia (incidence at 1 year reported in recent studies: 23.4%, 95% CI 14.6% to 33.3%),42 or have at least some degree of cognitive impairment.43 Hence, the clinical selection of non-demented CAA in included studies may seem to predict the decreased amyloid PET burden of these patients with relatively ‘pure’ CAA compared with the AD populations, underestimating the true effect sizes. This effectively represents spectrum bias and does not provide definite evidence of the amyloid-PET biomarker performance in a realistic clinical setting. Our results cannot thus be generalised to all unselected patients with CAA, but only apply to groups similar to those examined in the pooled studies, that is, largely presenting with sentinel CAA clinical phenotypes. More definitive evidence from carefully conducted studies in consecutive series of patients with symptomatic CAA is clearly needed. Of note, patients with AD also often demonstrate a high prevalence of CAA (in addition to parenchymal amyloid), if examined meticulously at histopathology, but it is usually mild to moderate.44 By contrast, in CAA with lobar ICH, a well-defined symptomatic phenotype of the disease, underlying CAA pathology is quite severe.45 Quite reassuringly, in two of the four studies13 33 that included an AD comparison group, none of the patients demonstrated lobar cerebral microbleeds (see table 1), a putative marker of the presence of advance CAA.
Apart from 11C- PiB, several 18F-labelled amyloid PET ligands have been developed and used in the detection of AD-related amyloid burden, including 18F-FDDNP, 18F-flumetamol, 18F-florbetapir and 18F-florbetaben.18 46 18F is considerably more convenient for widespread clinical use given its half-life of 110 min as compared with 20 min for 11C. However, so far only 11C- PiB and 18F-florbetapir have been used in CAA studies. Like 11C-PiB, 18F-florbetapir (ie, AV-45) has high in vitro affinity for fibrillar Aβ but none for tau aggregates.47 Comparison between in vivo 18F-florbetapir binding and postmortem amyloid-β burden in a large sample of elderly subjects scanned within 2 years of death showed highly correlated distributions, indicating 18F-florbetapir is a valid in vivo amyloid deposition marker.8 48 Direct comparison between 11C- PiB and 18F-florbetapir in cognitively normal-aged subjects and patients with mild cognitive impairment or probable AD has shown strong correlation.49 However, particularly given the potential overlap between CAA and AD, the issue of specificity of amyloid PET ligands for parenchymal versus vascular amyloid is important.11 12 11C-PiB binds to both parenchymal and vascular amyloid-β and thus cannot differentiate parenchymal from vascular amyloid deposits.50 Although to our knowledge no data are available regarding the vascular amyloid binding of 18F-florbetapir, likely it does not have any specificity either, its chemical structure being similar to 11C- PiB. Thus, differentiating PiB-PET or florbetapir-PET signal caused by CAA versus other kinds of amyloid deposits is currently impossible.51 52 Therefore, developing a molecular imaging tracer specific for cerebrovascular amyloid would be a game-changer for the field, allowing for directly detecting and following CAA pathology in vivo. Of note, there is absence of natural history data on rate of vascular amyloid progression, captured in amyloid-PET studies in CAA.12 Accordingly, active research has recently focused on PET tracers able to selectively detect CAA versus parenchymal amyloid-Aβ plaques, and effectively 18F-labelled or 68Ga-labelled ligands targeting amyloid-β aggregates on cerebral vessels have been developed.53 Although these promising PET tracers may provide useful tools for selective diagnosis of CAA, recent reports of their relatively poor brain penetration54 have somewhat dampened enthusiasm regarding their potential clinical use. Active research in this field is ongoing. A lead compound (among other candidate CAA-selective compounds) was recently reported at the fifth International CAA Conference (2016, Boston, Massachusetts, USA) to show potentially higher affinity for CAA lesions than amyloid-β parenchymal plaques by two-photon imaging in transgenic mice.55 It is highly plausible that specific CAA ligands tracer uptake distribution might differ more markedly between AD and CAA (and probably between other comparison groups, such as healthy elderly and deep ICH) than using PiB or florbetapir, although presently no tracer is at the stage of testing in the clinical setting. Of note, a single-photon emission CT tracer with selective binding to vascular amyloid has also been recently reported56 but has not been made clinically available yet.
Despite our fold change analytic approach, the pooled estimates were based on group-level rather than individual-level data and might still naturally depend on the exact method used to derive PET data. These issues would be expected to bias against significant differences in amyloid-PET profile in CAA versus comparison groups, rather than the observed differences. This limitation might, in part, explain the moderate-to-high statistical heterogeneity of the pooled estimates in our analyses. The I2 tests ranged between 69% and 94% and this substantial heterogeneity can also be observed in the forest plots by the non-overlapping CIs across some studies. Other potential reasons for heterogeneity in the results probably relate to pooling small studies of convenience patient samples, selection bias as detailed above, less established and validated PET protocols (as no consensus exists in the CAA field, especially for quantitative analysis), and confounding preanalytical cohort factors. In the methodological quality assessed using QUADAS-2 characteristics, three of the seven studies had scores consistent with risk of bias. These were mainly related to inadequacies in patient selection and omissions in reporting. In fact, another major finding of our paper can be considered the lack of systematic clinical studies of amyloid-PET in large consecutive patients and control groups in the CAA field, which leaves many questions unanswered.12
In light of the above well-appreciated considerations, our results will have to be interpreted with caution. Notwithstanding limitations, our analysis provides actionable data on the likely overall effect sizes and strength of the association of amyloid-PET burden and distribution in CAA, which might be useful for future studies.4 As more data become available on the topic, we are planning to further this work, including updates of our estimates and comparisons with the effect sizes of other advanced CAA biomarkers.
References
Footnotes
Contributors AC: statitical analysis, study concept and design, systematic review, data collection, analysis, write-up. KF: systematic review, data collection, critical revisions. H-HT: data collection, critical revisions. L-KT: data collection, critical revisions. R-FY: data collection, critical revisions. J-CB: study concept and design, systematic review, data collection, write up.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice Since this paper was first published online the author Hsin-Hsi Tsai has updated their affiliation from the Martinique University Hospital to the Department of Neurology, National Taiwan University Hospital, Taipei, Taiwan.