Article Text

Abstract
Aneurysms of the distal lenticulostriate artery (LSA) are rare. Only 16 cases have been reported in the literature. Early detection and treatment of these aneurysms is also difficult because of their deep location, small size and angioarchitecture. We report two additional patients with aneurysms, arising from the distal LSA, who presented with deep intracerebral haemorrhage. The conclusions drawn from our experience and a comprehensive review of the literature include the following. (1) A distal LSA aneurysm should be considered in young (mean 38.5 years) and non-hypertensive (80%) patients with deep intracerebral haemorrhage. (2) These aneurysms are frequently very small (<5 mm). Therefore, they cannot be detected on initial angiograms in some cases. (3) These aneurysms have higher rates of associated vascular lesions. Deep intracerebral haemorrhage, even in those over the age of 50 years, can still be due to underlying, treatable structural abnormalities, and should not be dismissed as being a result of hypertension. In addition, a more comprehensive diagnostic approach seems to be warranted in younger patients and those without known hypertension.
Statistics from Altmetric.com
Deep intracerebral haemorrhage (ICH) associated with hypertension is common and may originate from a ruptured microaneurysm, arterial dissection of penetrating arteries or rupture of arteries that have degenerative changes from a pathological viewpoint.1 As cerebral angiography is not routinely performed in typical deep ICH, particularly in elderly patients,2 aneurysms are rarely discovered with conventional imaging either before or after haemorrhage.
To our knowledge, only 16 cases of aneurysm of the distal lenticulostriate artery (LSA) presenting as deep ICH have been reported in the English medical literature.3–18 We present an additional two cases in which a ruptured distal LSA aneurysm was documented by cerebral angiograms. In addition, we review the clinical and angiographic characteristics and treatment of distal LSA aneurysms. Diagnostic evaluation and treatment modalities of distal LSA aneurysms are highlighted.
CASE NO 1
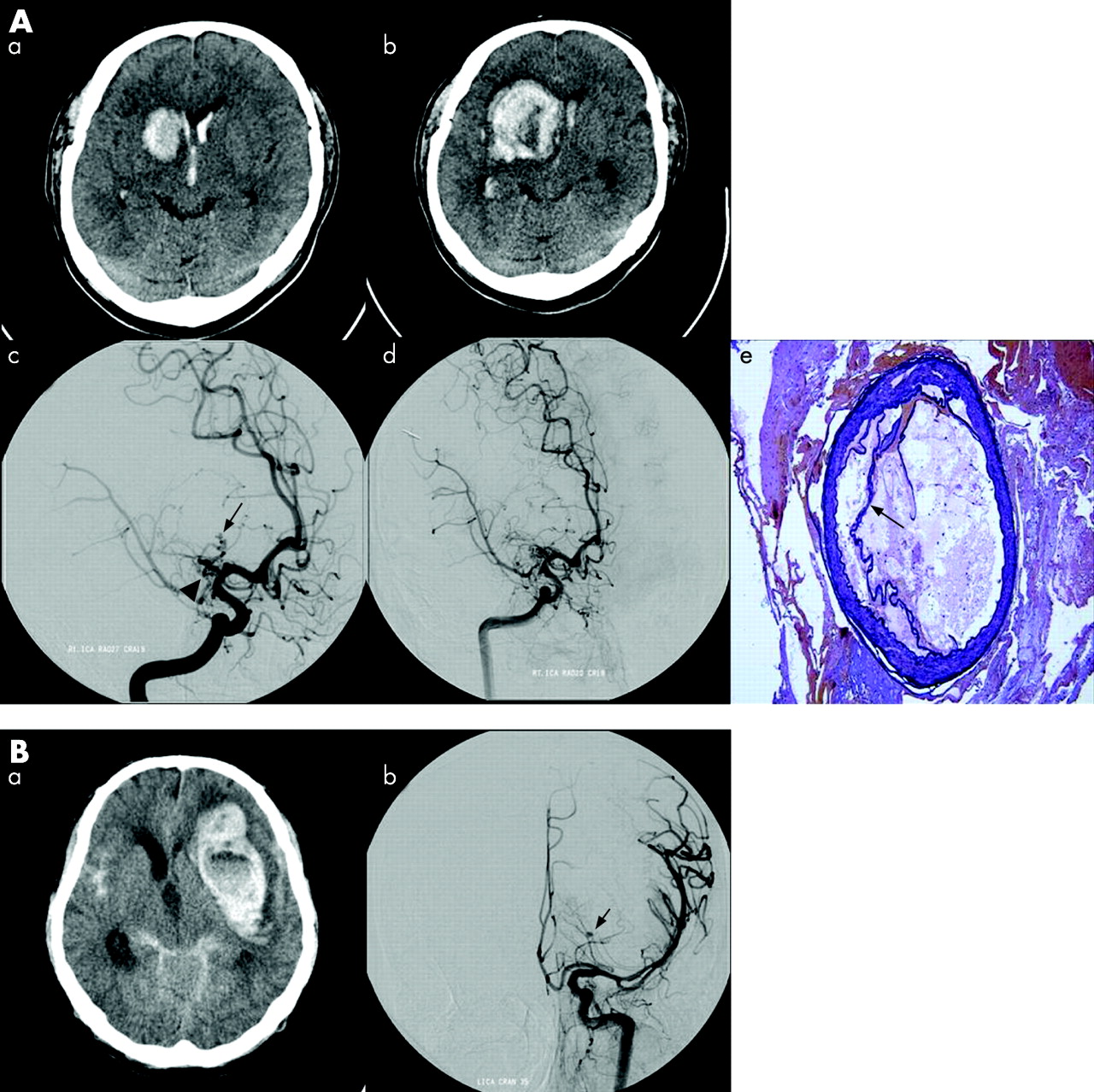
A 49-year-old man presented with sudden onset of headache and vomiting. The patient had no history of hypertension, infectious disease, heart disease, head injury or intravenous drug abuse. He was alert with no neurological deficit. His initial Glasgow Coma Scale (GCS) was 15. CT scan revealed right basal ganglia haemorrhage with intraventricular extension (fig 1A, a). Initially, conservative treatment was selected based on haematoma size and neurological condition. However, on day 14, the patient had sudden drowsiness and profound left sided weakness. He had dense facial droop on the left, antigravity strength in the left upper limb and no motor function in the left lower limb; his GCS was 10. Repeat CT scan demonstrated enlarged ICH compromising adjacent structures (fig 1A, b).

{kind=link}
As he was relatively young and had no risk factors for stroke, cerebral angiography was performed; it disclosed an occlusion of the proximal right middle cerebral artery and ipsilateral moyamoya-type vessels. Circulation to the right hemisphere distal middle cerebral territory was via collaterals from the leptomeningeal vessels of the right anterior and posterior cerebral arteries. A small aneurysm of the right middle cerebral artery distal to the lenticulostriate branch was also detected (fig 1A, c).
Treatment was indicated because of rapid haemorrhage growth and the propensity to bleed. The patient underwent urgent operation via a right frontotemporal craniotomy. A small corticotomy on the cortical surface was made and the haematoma gently evacuated. Spherical dilation of the distal LSA was identified. Excision of the aneurysm was successfully achieved without vessel sacrifice. Microscopic examination revealed a true aneurysm with continuous intimia, media and adventitia (fig 1A, e). The wall of the internal elastic lamina was depleted and there were no inflammatory changes. Thrombus within the dissected outer layer was noted.
The postoperative course was uneventful and the patient showed progressive neurological recovery. Cerebral angiography performed at 4 weeks showed complete aneurysm obliteration (fig 1A, d). The patient was discharged at 8 weeks after the first ictus. The patient showed complete recovery from dysarthria although the left upper hand power was still grade IV and lower limb power improved only up to grade IV.
CASE NO 2
A 24-year-old man had sudden onset of loss of consciousness and presented in a semicomatous state with bilateral decorticated posture; his GCS was 4. His left pupil was fully dilated and non-reactive. He had no history of hypertension, infectious disease, heart disease, head injury or intravenous drug abuse. CT scan revealed a massive deep ICH with subarachnoid (SAH) and intraventricular (IVH) haemorrhages (fig 1B, a). Cerebral angiograms disclosed a distal LSA aneurysm branching off the left carotid bifurcation (fig 1B, b). During catheter angiography, his right pupil began to dilate, and he was comatose; his GCS was 3. Emergency surgery was planned but deferred because of lack of family consent. Conservative treatment was selected, and the patient died 3 days after aneurysmal rupture.
DISCUSSION
The literature has reported 16 previous cases of distal LSA aneurysm (table 1). Although a small number, this series displays interesting features—namely, younger mean age of presentation than sporadic saccular intracranial aneurysms, no female predominance and higher rates of associated vascular lesions. The eight male and 10 female patients were aged 2 months to 69 years (mean 38.5 years). A history of hypertension was associated in only 2 (20%) of 10 patients. ICH, SAH and IVH occurred in isolation or in combination. As a result, there were five possible intracranial haemorrhage types: isolated ICH (four patients, 23.5%), isolated IVH (one patient, 5.9%), ICH and IVH (eight patients, 47.0%), ICH and SAH (two patients, 11.8%) and a combination of all three (two patients, 11.8%). Associated diseases included moyamoya or moyamoya-like disease (six patients), arteriovenous malformation (one patient), systemic lupus erythematosus (one patient) and brain tumour (one patient). These aneurysms were frequently very small (<5 mm). Therefore, they cannot be detected on initial angiograms in some cases.13 16 Most of the aneurysms originated from the lateral LSA territories.
Five of 18 patients were treated conservatively. One patient underwent haematoma removal only, and the distal LSA aneurysm did not rebleed for 8 years.10 The other 12 patients were treated surgically to prevent recurrent bleeding. Surgical interventions included extirpation of the aneurysm in six cases, neck clipping in three, proximal clipping in two and endovascular embolisation with N-butyl cyanoacrylate in one case. Microscopic examination was performed in seven cases; all revealed true aneurysms.6 8 12 Clinical outcomes were good in seven patients, fair in seven, poor in one and death in three. Two of five patients who underwent conservative management alone died. Surgical mortality rate was 7.7%.
One of the major management tasks is to find out whether the haemorrhage is secondary to underlying structural vascular abnormality, such as arteriovenous malformation and aneurysm, so that appropriate treatment can be carried out to prevent rebleeding. Deep ICH is commonly associated with pre-existing hypertension in the elderly population. Because catheter angiography is an invasive procedure, carrying a low but definite risk,19 it is not routinely performed in typical deep ICH, especially in elderly patients.2 However, even in the presence of pre-existing hypertension, as much as 36% in a series of 144 autopsy cases showed a specific structural lesion causing the massive brain haemorrhage.20 Some authors have suggested that in hypertensive patients with deep ICH, catheter angiography is not indicated,21 whereas others have recommended that catheter angiography should be considered for all patients with spontaneous ICH, regardless of the site or history of hypertension.22
Our literature review of distal LSA aneurysm with deep ICH found only two patients with pre-existing hypertension (20%). These patients were relatively young (mean 38.5 years) but 5 (27.8%) of 18 patients were older than 50 years. Our study demonstrated that deep ICH, even in those older than 50 years of age, can still be due to underlying, treatable structural abnormalities, and should not be dismissed as being due to hypertension. In common with our literature review, a more comprehensive diagnostic approach seems to be warranted in younger patients and those without known hypertension.
The most appropriate treatment of LSA aneurysm remains controversial because of the small patient numbers and uncertain natural history. Conservative treatment and careful follow-up angiography seem appropriate for lesions consistence with pseudoaneurysm, whereas direct surgery could be considered in typical saccular aneurysms. Treatment is clearly indicated for increasing aneurysm size and to prevent rebleeding.
These distal LSA aneurysms cannot usually be clipped without sacrificing the parent artery because of the fragile nature and very small size of the parent artery. Although occlusion of the proximal segment most probably results in contralateral hemiplegia, this procedure may well be tolerated on the distal segment because of the rich anastomotic network.23 Although many authors have trapped the parent artery and resected these aneurysms without further neurological damage, we believe that whenever possible, this artery should be preserved.
Deep ICH can hide the parent artery, and proximal control cannot be obtained at an early stage. In addition, detection of these aneurysms may be difficult because of the deep location in the basal ganglia and small size of the aneurysm. For this purpose, the use of frameless stereotactic guidance may be very useful for these small aneurysms which are frequently embedded in the brain tissue.17 Also, intraoperative angiography can confirm successful aneurysm obliteration and provide immediate feedback to the surgical team.
REFERENCES
Footnotes
This study was supported by a faculty research grant from Yonsei University College of Medicine for 2006.
Competing interests: None.
- Abbreviations:
- GCS
- Glasgow Coma Scale
- ICH
- intracerebral haemorrhage
- IVH
- intraventricular haemorrhage
- LSA
- lenticulostriate artery
- SAH
- subarachnoid haemorrhage