Article Text

Abstract
Objective: To determine the proportion of platelets and fibrin in coronary thrombi.
Design: Immunohistochemical and morphometric means to examine the coronary arteries of 31 patients who died of acute myocardial infarction.
Results: Fresh thrombi were detected in the feeding arteries of infarction areas in 23 cases (74%) and were associated with plaque rupture in 18 (78%) and plaque erosion in 5 (22%). An immunohistochemical study showed that the thrombi consisted of a mixture of fibrin and platelets as well as some other types of blood cells. The fibrin and platelet positive areas in the thrombi associated with plaque rupture accounted for 74 (19)% and 35 (20)% (p < 0.01) and those associated with erosion accounted for 51 (6)% and 70 (21)%, respectively, of the total areas. Areas of positive immunoreactivity for tissue factor and C reactive protein were also significantly greater in ruptured than in eroded plaques.
Conclusion: These results indicate that the proportions of fibrin and of platelets differ in coronary thrombi on ruptured and eroded plaques. Higher proportions of tissue factor and C reactive protein contribute more significantly to thrombus formation on plaque rupture than on plaque erosion.
- thrombus
- acute myocardial infarction
- fibrin
- platelet
Statistics from Altmetric.com
Thrombus formation on disrupted atherosclerotic plaques plays a fundamental part in the development of acute coronary syndromes and in the progression of atherosclerosis.1 Coronary thrombosis occurs most often in lipid rich ruptured plaques, but eroded plaques lacking a superficial lipid core or that do not rupture are also often associated with acute coronary syndromes.2–6 The thrombogenicity of atherosclerotic lesions mostly depends on the nature and extent of the plaque components exposed to the circulating blood flow. Since platelet adhesion and aggregation are essential steps in haemostatic and thrombotic processes, the development of platelet rich thrombi has been regarded as a trigger of acute coronary syndromes.7,8 However, the effect of antiplatelet administration is quite variable in terms of reducing the incidence of death, myocardial infarction, or the need for further intervention.9–11 In addition, necropsy studies have shown that thrombi causing myocardial infarction contain not only platelets but also a large amount of fibrin, suggesting an increase in activation of the coagulation cascade during the event.12,13 We and others have shown that tissue factor expressed in atherosclerotic lesions is an important determinant of thrombogenicity that contributes to fibrin-rich thrombus formation after plaque disruption.14–17 However, the thrombus components that develop on plaque rupture and during erosion are unknown.
We therefore investigated immunohistochemically the nature of thrombi that developed on plaque rupture and erosion. We also measured the expression of tissue factor and C reactive protein (CRP), a non-specific marker of inflammation and a predictor of incident cardiovascular events, in disrupted coronary plaques from necropsies.18,19
METHODS
Selection of cases
We examined the hearts of 31 patients who had died of acute myocardial infarction within three days of onset. Necropsies were performed at Miyazaki Medical College Hospital and Miyazaki Prefectural Hospital. Acute myocardial infarction was defined as typical chest symptoms lasting over 30 minutes, ST-T wave changes or abnormal Q waves on ECG, and serum creatine kinase concentrations above twice the upper normal limit. Patients who had undergone coronary intervention were excluded from this study. This study protocol was approved by the ethics committee of Miyazaki Medical College.
Coronary artery evaluation
All hearts were initially examined while fresh and then fixed whole at the time of necropsy. The coronary arterial trees were gently perfusion fixed with 10% buffered formalin to prevent any distortion of coronary thrombi and were further immersed in the same fixative for 72 hours at room temperature. The major epicardial coronary arteries (left main, left anterior descending, left circumflex, and right coronary arteries) and their major branches (left diagonal and left obtuse marginal branches and posterior descending coronary artery) were cut transversely at 3 mm intervals (following decalcification if necessary). Segments with over 50% cross sectional luminal stenosis according to a visual inspection were histologically analysed.3 These segments were embedded in paraffin, cut into 4 µm thick sections, and then visualised by haematoxylin and eosin, Mallory azan, and elastica van Gieson staining.
Samples with coronary thrombi were separated based on the morphology of the underlying plaque as follows3,4: plaque rupture with a disrupted fibrous cap over a lipid core with an acute thrombus continuous to the lipid pool (fig 1A); and those with superficial erosion (without plaque rupture) in which an acute thrombus directly contacted the intimal plaque without a ruptured lipid pool (fig 2A). Lipid cores located deep within the unruptured plaques with superficial erosion did not communicate with the thrombus. Segments with luminal thrombi without rupture into the lipid core were serially step sectioned and stained (at every 20 µm for at least 1 to 2 cm) to determine whether the fibrous cap was ruptured.

Representative micrographs of plaque rupture with thrombus. (A) Thrombus on ruptured plaque (haematoxylin and eosin stain). Extensive necrotic core contains foamy macrophages and disrupted fibrous cap. Thrombus is composed of large amount of (B) fibrin and (C) platelets.

Representative micrographs of plaque erosion with thrombus. (A) Non-occlusive thrombus on eroded plaque (haematoxylin and eosin stain). Plaque is fibrous and without visible atheromatous component. Thrombus is composed of (B) fibrin and (C) platelet mixtures and is relatively more rich in platelets than in fibrin.
Coronary artery segments that contained acute thrombi determined by light microscopy (luminal collections of platelet, fibrin, or both, with or without trapped erythrocytes and white blood cells) were selected for immunohistochemical and morphometric evaluation. Deparaffinised sections were immunohistochemically stained with avidin-biotin complex and antibodies to fibrin (Takeda Chemical Industries, Ltd, Osaka, Japan),20 platelet glycoprotein IIb (CD41, DAKO Japan, Kyoto, Japan), tissue factor (Chemo-Sero-Therapeutic Research Institute, Kumamoto, Japan), CRP (DAKO Japan), macrophages (DAKO Japan), and smooth muscle cells (α smooth muscle actin, DAKO Japan). Sections were counterstained with haematoxylin. Positive and negative controls were included in parallel for every stain. The extent of immunoreactive areas of fibrin or platelet was quantified in at least 10 serial step sections from each necropsy sample with an image analysis system (SPICA-11, Nippon Avionics Co, Tokyo, Japan) and was expressed as the percentage of the total amount of thrombus area. We also evaluated areas positive for tissue factor or CRP in underlying plaques at rupture or erosion sites (in areas of 1 mm2).
Risk factors
The following risk factors for coronary artery disease were assessed from medical records and compared between cases of plaque rupture and of erosion: age, sex, hypertension, diabetes mellitus, hypercholesterolaemia, and smoking habit. The presence or absence of risk factors was determined as follows. Hypertension was considered to be present when long term treatment had been given or was required. Diabetes mellitus was defined by a previous physician’s diagnosis and treatment with insulin, oral hypoglycaemic agents, or diet. Hypercholesterolaemia was defined as a serum total cholesterol concentration of over 5.7 mmol/l. Current smokers were considered to have had a smoking habit.
Statistical analysis
Data are presented as mean (SD). Continuous variables were compared by analysis of variance and categorical variables were compared by the χ2 test (StatView software, version 5.0; SAS Institute, Cary, North Carolina, USA). A probability value of p < 0.05 was considered significant.
RESULTS
The mean (SD) age of the 24 men and seven women at the time of death was 68 (10) years (range 49–95 years). Twenty three of 31 (74%) had acute thrombi in the major epicardial coronary arteries (left anterior descending, seven; left circumflex, six; and right coronary artery, 10). Of the 23 acute thrombosed coronary artery plaques, 18 were plaque ruptures (78%, 16 men and two women) and five were superficial erosions (22%, four men and one woman) (figs 1A and 2A).
Thrombi on plaque rupture or erosion
The immunohistochemical study showed that all thrombi that developed on plaque rupture and erosion were composed of a mixture of fibrin and platelets. Fibrin was more abundant than platelets in thrombi on ruptured plaque (fig 1B, C). Image analysis showed an immunopositive area for fibrin that was significantly greater than that for platelets (table 1). In contrast, the thrombi on eroded plaques were relatively but not significantly richer in platelets than in fibrin (fig 2B, C, table 1). Foci of macrophages at the luminal surface adjacent to the thrombus were present in all 18 ruptured plaques (100%) versus three eroded plaques (60%). In contrast, smooth muscle cells were clustered at the luminal surface adjacent to the thrombus in all eroded plaques (100%) compared with four ruptured plaques (22%).
Proportion of immunoreactive areas in thrombi and disrupted plaques
Tissue factor and CRP in plaques
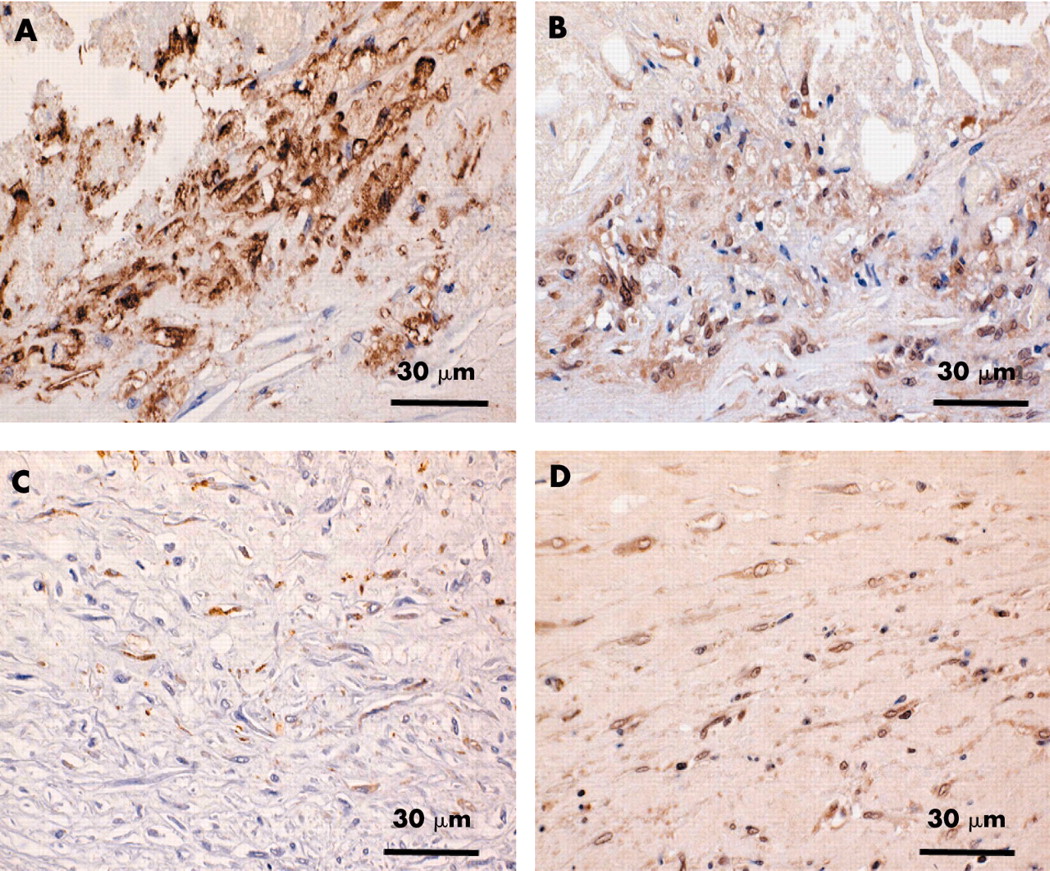
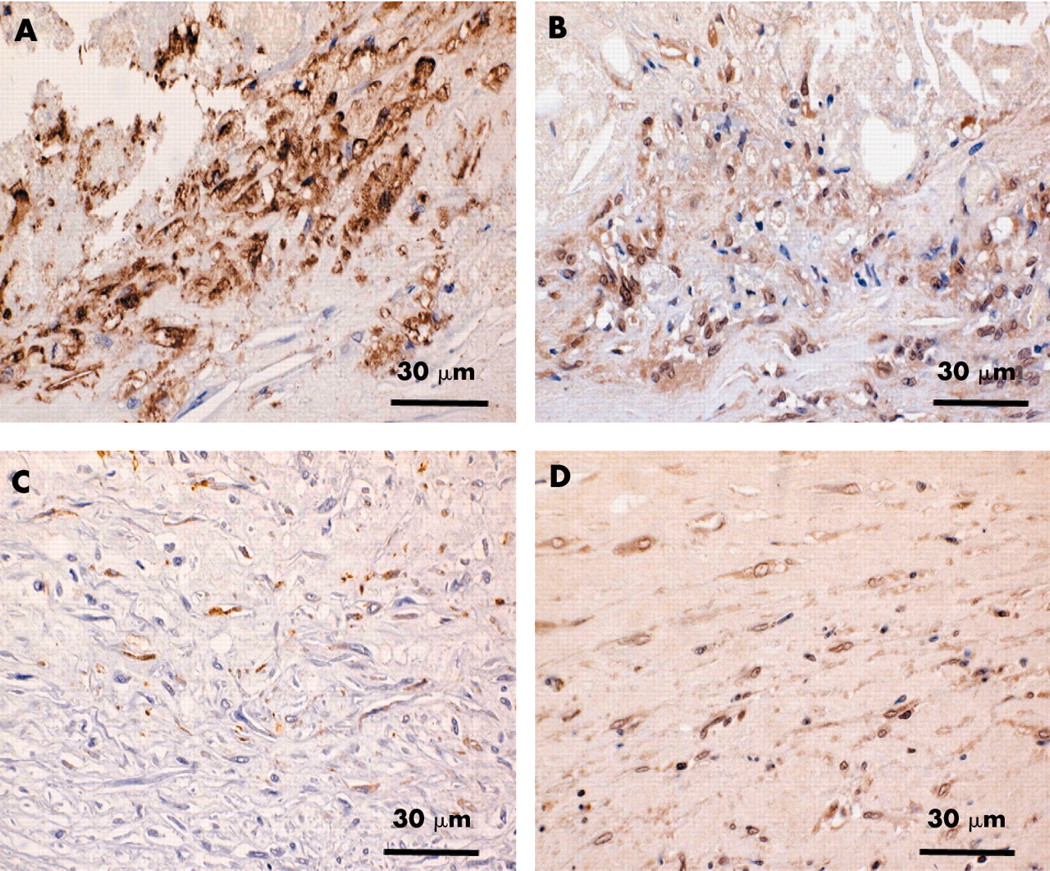
Underlying rupture was intensely immunoreactive for both tissue factor and CRP. Many foamy macrophages, smooth muscle cells, and extracellular matrix in the plaques were intensely positive for tissue factor and CRP (fig 3A, B). In contrast, smooth muscle cells and extracellular matrix in the eroded plaques were focally positive for tissue factor and CRP (fig 3C, D). The stained areas for these antigens were significantly greater in the plaques underlying rupture than those underlying erosion (table 1).
{kind=link}
{kind=link}
{kind=link}
Representative immunohistochemical micrographs of (A, B) ruptured and (C, D) eroded plaques. Ruptured plaque is intensely immunoreactive for (A) tissue factor and (B) C reactive protein. Eroded fibrous plaque is weakly stained for (C) tissue factor and (D) C reactive protein.
Risk factors
Age, sex, incidence of hypercholesterolaemia, diabetes mellitus, hypertension, and smoking did not differ significantly between plaque rupture and erosion (table 2).
Risk factors and types of disrupted plaques
DISCUSSION
The present study showed that the thrombi of ruptured plaques were more significantly rich in fibrin and that more tissue factor and CRP were expressed in ruptured than in eroded plaques.
Acute coronary thrombosis leading to acute myocardial infarction may arise from a difference in underlying plaque morphology, namely rupture and superficial erosion.2–6 In acute coronary death with coronary thrombosis, two necropsy studies have found plaque rupture in 75% of cases and that erosion accounted for the remainder.2,6 Kojima and colleagues5 found plaque rupture in 81% and erosion in 19% of Japanese patients who died of acute myocardial infarction.5 The findings of the present study agree with these previous results. In contrast, Farb and colleagues3 and Burke and associates4 have reported that 56% of such deaths are associated with plaque rupture and 44% with erosion. In addition, they found plaque erosion in 69% of women who died of sudden ischaemic heart disease.3,4 These reports emphasised a high rate of plaque erosion, especially among young or premenopausal women. Because of the very limited number of women in the present study, we could not evaluate the influence of sex on plaque morphology. A necropsy study by Kojima and colleagues5 found plaque erosion in 31% of the Japanese women studied, indicating potential race differences in the incidence of this condition.
Clinical and experimental animal studies have provided evidence of the role of plaque disruption and acute thrombus formation in the onset of acute coronary events.7,21 The most widely accepted hypothesis is that plaque disruption activates circulating platelets by exposing the subendothelium to blood circulation and that subsequent platelet adhesion and aggregation result in obstructive thrombus formation.7,8 On the basis of this hypothesis, antagonists for the platelet glycoprotein IIb/IIIa receptor, which is a final common pathway of platelet aggregation, have been tested in randomised, placebo controlled trials of acute coronary syndromes and in percutaneous coronary intervention. For patients undergoing percutaneous revascularisation, these agents have reduced the incidence of death, myocardial infarction, and the need for urgent reintervention.9,10 However, trials of glycoprotein IIb/IIIa receptor antagonists for patients with acute coronary syndromes have yielded more modest or less apparent benefits,11 which raises the notion of a different mechanism of thrombus formation on plaque disruption. Necropsy studies of acute myocardial infarction have shown that only 15% of occlusions consist of pure platelet thrombus, whereas 85% of occlusive thrombi are largely composed of fibrin as well as platelets.13 We have also shown that all of the thrombi detected at plaque disruption sites consisted of a mixture of fibrin and platelets and that fibrin was more abundant in thrombi on ruptured plaque. These findings indicate that antiplatelet treatment may have variable effects on acute coronary events and suggest that a combination of antiplatelet and anticoagulant agents would be more favourable. Recent clinical studies have shown that aspirin in combination with anticoagulants is more effective than aspirin alone in reducing the incidence of serious cardiovascular events and death after acute coronary events, although the risk of bleeding is increased.22,23
Tissue factor immunoreactivity was more prominent in ruptured than in eroded plaques. Consistently expressed mainly in macrophages and smooth muscle cells of plaques, tissue factor induces procoagulant activity in atherosclerotic lesions.14,16,24 Evidence suggests that increased activity of the tissue factor mediated coagulation cascade significantly contributes to thrombus formation at plaque disruption sites. The presence of abundant tissue factor in ruptured plaques is considered to contribute to fibrin-rich thrombus formation. Plasma concentrations of tissue factor are significantly increased in patients with ischaemic heart diseases.25 Meanwhile, a crucial role of circulating tissue factor in the process of thrombus formation has been proposed26 and the present study found positive tissue factor immunoreactivity in thrombi (data not shown), which supports this notion.
In the underlying plaque associated with rupture, CRP immunoreactivity was significantly more abundant than in that associated with erosion. Previous reports have associated CRP with a risk of future ischaemic heart diseases.18,19 In addition, CRP mRNA and protein are expressed within atheromatous plaques, being primarily localised to macrophages and extracellularly within the lipid core.27,28 Although we could not examine serum CRP concentrations in our necropsy cases, Burke and colleagues29 found a positive correlation between the intensity of CRP staining and serum concentrations of CRP. However, the importance of CRP to plaque rupture and thrombosis remains unclear. A functional significance to these pathological findings has been suggested by co-localisation with components of the complement system within atherosclerotic plaques.30 Indeed, CRP can actively stimulate the classic complement pathway and enhance phagocytic activity as an important mediator of innate immunity.31 Within atherosclerotic plaques, CRP mediated opsonisation may be important for low density lipoprotein uptake by macrophages and foam cell formation.32 In vitro studies have shown that CRP enhanced the expression of adhesion molecules in endothelial cells and induced high concentrations of tissue factor expression in monocytes.33,34 These lines of evidence suggest that abundant CRP deposition within plaques contributes not only to the regulation of the inflammatory process but also to thrombus propagation.
Study limitations
Because the present study examined a small number of cases, especially of women, we could not evaluate the inherent bias in the selection of patients for necropsy. It is difficult to draw firm conclusions regarding the differences between the findings on rupture and on erosion, since the eroded plaques were found in only five patients as opposed to 18 with ruptured plaques. In addition, the information source for risk factors was limited to a single postmortem collection and the duration of risk factor exposure was not available. Information regarding risk factor modification (for example, aspirin, hormone replacement therapy, and statin use) was often incomplete.
Acknowledgments
We thank Drs Tohru Hayashi (Miyazaki Prefectural Miyazaki Hospital) and Akira Ishihara (Miyazaki Prefectural Nobeoka Hospital) for providing permission to review their necropsy cases. This study was supported by Grants-in-Aid for Scientific Research (No 14570153) and for the 21st Century COE program (Life Science) from The Ministry of Education, Science, Sports, and Culture, Japan, and by a grant from the Terumo Foundation, Japan.