Article Text

Statistics from Altmetric.com
Introduction
Cerebral venous thrombosis (CVT) is a rare condition accounting for <1% of all strokes, with highly variable clinical presentations ranging from a headache to coma.1–4 Although MRI and MR venography have significantly improved early diagnosis, clinical outcomes after treatment remain mixed.5 6
The aims of this document include: (1) to review existing knowledge about the natural history, diagnostic methodology, and treatment modalities/techniques for CVT, and (2) to provide recommendations on management strategies for CVT using the best available evidence, but out of necessity, frequently relying on expert opinion concerning this rare disease. Recommendations follow the American College of Cardiology/American Heart Association (ACC/AHA) classification of recommendation/level of evidence and definition of classes and levels of evidence used in AHA/American Stroke Association (ASA) recommendations.7
Literature search
The Standards and Guidelines Committee of the Society of Neurointerventional Surgery (SNIS), a multidisciplinary society representing leaders in the field of endovascular therapy for neurovascular disease, prepared this document based on a comprehensive review of English language literature relating to the topic. A literature search using PubMed (US National Library of Medicine) and Ovid (Wolters Kluwer) databases was performed from January 1, 1980, through December 31, 2016. The following key words were used: [(sinus thrombosis) AND ((cerebral veins) OR (cranial sinuses) OR (heparin) OR (thrombectomy) OR (anticoagulation))]. A review of references provided in review articles and textbook chapters was also performed. Studies published in languages other than English were excluded.
Incidence/prevalence
The estimated incidence of adult CVT is 1.32 per 100 000 person-years. Among women aged between 31 and 50 years, the incidence is as high as 2.78 per 100 000 person-years.8 9 In children less than 18 years of age, the estimated incidence is 0.67 per 100 000 children per year, with neonates the most affected age group.10 Risk factors and conditions known to be associated with CVT are listed in table 1.8 11 Inherited hypercoagulability including protein C, protein S, antithrombin deficiencies and factor V Leiden or resistance to activated protein C are estimated to account for 25–35% of all occurrences of CVT.12 13 The use of oral contraceptives is associated with a four- to sevenfold increase in the risk of CVT.14 In addition, the risk of CVT in woman using oral contraceptives may increase nearly 35- fold if she is heterozygous for factor V Leiden.15 Around 15% of CVT cases occur in patients without identifiable risk factors or predisposing causes.8 16
Major risk factors and conditions associated with cerebral venous thrombosis
Natural history
Data on the natural history of CVT are limited, as most studies reporting the clinical outcomes of CVT include patients treated with anticoagulation.17 Studies of the true natural history of CVT are available from the ‘pre-heparin’ era or from the placebo arms of the early randomized anticoagulation trials of CVT medical therapy.18–21 Outcomes of these studies are summarized in table 2. Mortality in the small populations of these studies ranged from 14% to 40% in patients who did not receive anticoagulation.
Studies reporting natural history of venous sinus thrombosis
Diagnosis and management
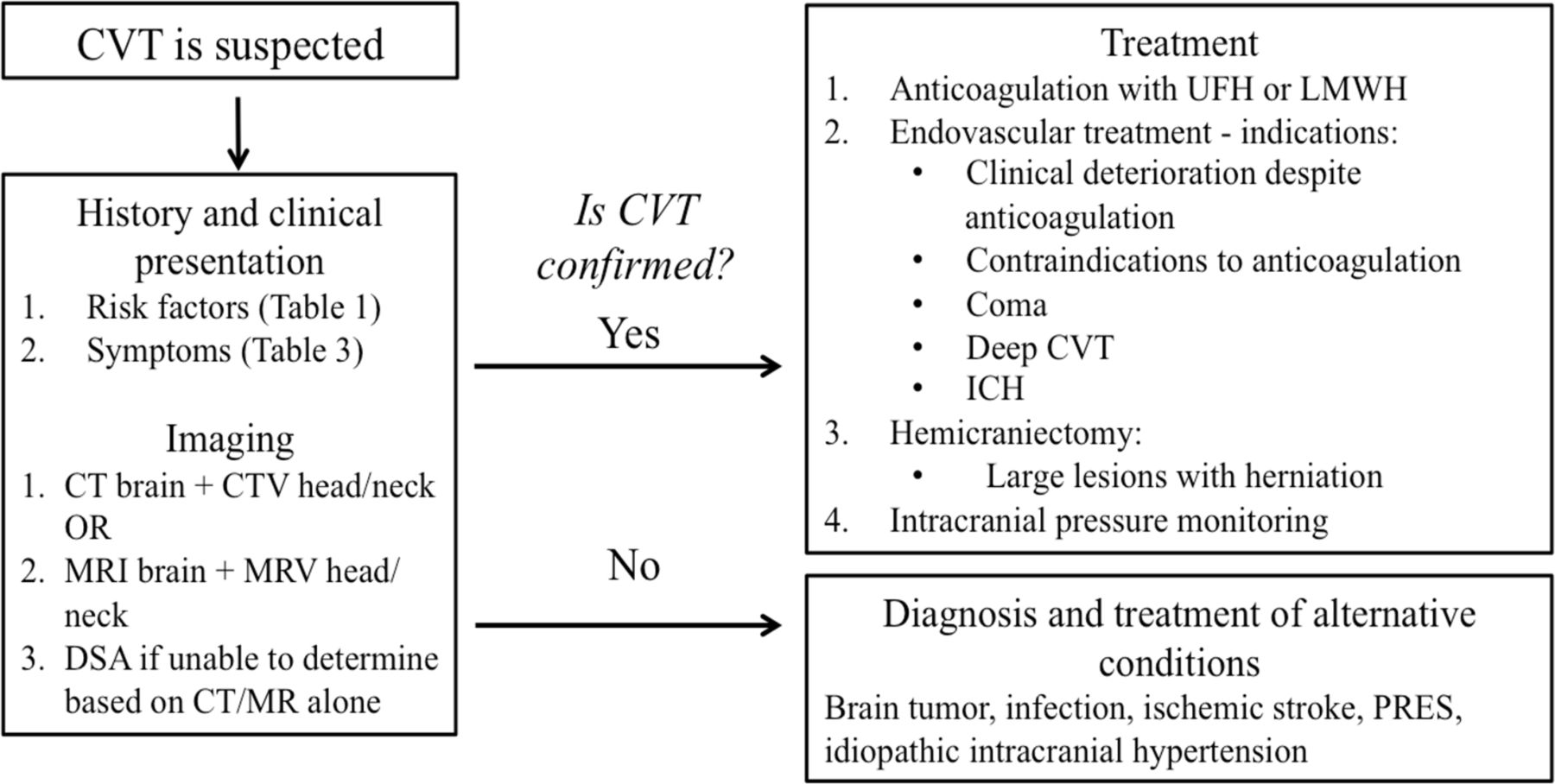
An algorithm for the diagnosis and management of CVT is shown in figure 1.

An algorithm for the diagnosis and management of CVT. CTV, CT venography; CVT, cerebral venous thrombosis; ICH, intracerebral hemorrhage; LMWH, low molecular weight heparin; MRV, magnetic resonance venography; PRES, posterior reversible encephalopathy syndrome; UHF, unfractionated heparin.
Clinical presentation
Clinical presentations of CVT are diverse, and are affected by the patient’s age, the interval between onset and hospitalization, location of thrombosis, and extent of the thrombosis.9 22 Common clinical signs and symptoms of CVT include headache, focal neurologic deficits, seizure, and diffuse encephalopathy, while rare symptoms include cavernous sinus syndrome and coma.4 Table 3 summarizes common presentations. The clinical significance and presentations of venous thrombosis depend on the location of the thrombosis and a patient’s venous anatomical disposition, especially collateral pathways. Thus, clinical presentation can be diverse and non-specific. For example, CVT should be excluded before making the diagnosis of idiopathic intracranial hypertension since CVT can present with the insidious development of papilledema.23 Crescendo-type progression of non-specific clinical presentations such as seizure or focal neurological deficit over a few days should raise a strong suspicion, and be followed with appropriate imaging studies for the diagnosis of CVT.22 Venous thromboembolism (deep vein thrombosis in the lower limbs or pulmonary embolism) may develop in patients with CVT.
Clinical presentations of cerebral venous thrombosis
Diagnostic imaging
CT
Neuroimaging findings of CVT are variable and multiple modalities may be required to assess both the venous vascular anatomy and parenchymal complications of edema, hemorrhage, and infarction. Non-contrast CT is non-specific and can be normal in up to 25% of patients.4 Classic signs of acute CVT on non-contrast CT of the head include an increase in attenuation (hyperdensity) of the occluded sinuses or cortical veins and cerebral edema (figure 2A).24 25 Intracerebral hemorrhage occurs in 9–39% and can present as parenchymal, intraventricular or subarachnoid hemorrhage.26–28 A wide range of non-contrast CT accuracy in diagnosing CVT has been reported: 30–100% for sensitivity and 83–100% for specificity. On contrast-enhanced CT, the empty delta sign characterized by an intraluminal filling defect may indicate a thrombus within the superior sagittal sinus.29 The empty delta sign is present in 4–28% of cases of CVT.28–30 Hemoglobin and hematocrit levels correlate with CT attenuation in cerebral venous sinuses, and their high levels may mimic CVT in certain conditions such as polycythemia.31 32 Two studies separately confirmed a Hounsfield unit >70 to be highly specific for acute CVT.31 33
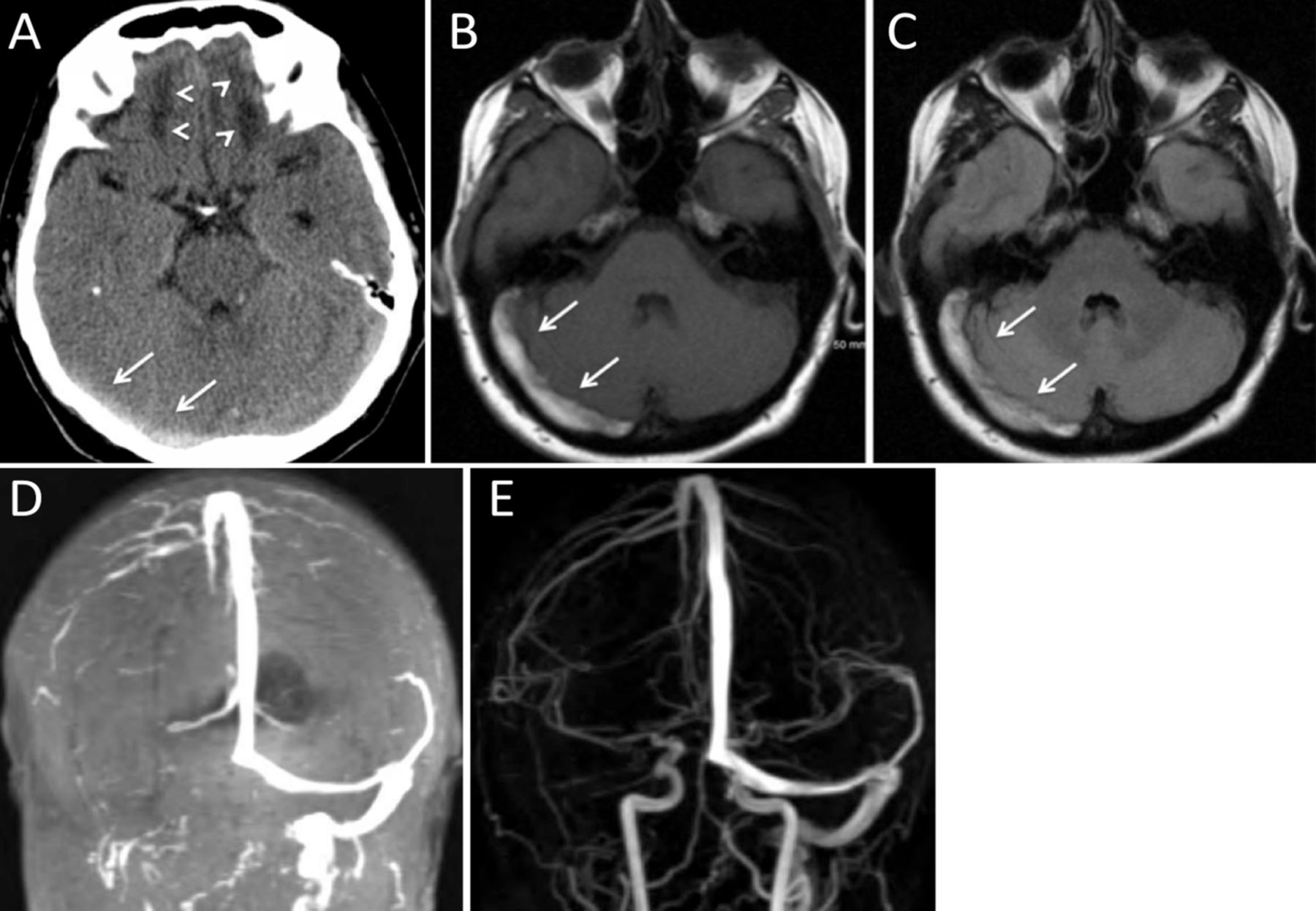
Right transverse sinus venous sinus thrombosis in a patient with head trauma. (A) Non-contrast CT of the head, axial view, shows a hyperintensity within the right transverse sinus (arrows) measuring >70 Hounsfield units, which is highly specific for acute thrombus. Bilateral frontal lobe hypodensities are consistent with the diagnosis of recent head trauma (arrowheads). (B) T1 and (C) FLAIR images of MRI brain performed 3 days after the initial head CT show an area of increased signal intensity within the right transverse sinus, consistent with subacute thrombus (arrows). (D) Time-of-flight MR venography and (E) contrast-enhanced MR venography demonstrate normal appearance of the superior sagittal sinus and left transverse sinus. No flow signal in the right transvers sinus and right internal jugular vein is seen.
MRI
The signal intensity of thrombus on MRI varies over time on T1- andT2-weighted sequences depending on the acuity of CVT (T1 isointensity and T2 hypointensity in the acute stage, and both T1 and T2 hyperintensity in the subacute stage; figure 2B, C).34 T2* gradient echo (GRE) and susceptibility weighted imaging (SWI) are highly accurate conventional MRI sequences in the diagnosis of CVT, owing to their sensitivity for susceptibility effects from hemorrhage/thrombus and blood oxygen level dependent imaging to delineate the venous anatomy, respectively.35 36 Heterogeneous MRI patterns are also observed with diffusion-weighted imaging (DWI) and calculated apparent diffusion coefficient (ADC) mapping in the evaluation for venous infarction in the setting of CVT.37 Although vasogenic edema is characterized by an increase in ADC values and is reversible, persistent lesions with restricted diffusion (low ADC values) are suggestive of cytotoxic edema and infarction, but reversibility can be seen in patients with seizures.38 Venous infarction patterns on MRI differ from arterial territory stroke and are often bilateral, helping distinguish CVT from arterial etiologies.39 Conventional MRI sequences including T1-, T2-, T2*-weighted GRE, SWI, fluid-attenuated inversion recovery (FLAIR), and DWI are more accurate than non-contrast CT, and have an overall sensitivity of 72–84% and specificity of 90–95% for the diagnosis of CVT.39 40 Contrast-enhanced 3D GRE T1-weighted imaging with capability of multiplanar imaging is even more accurate than conventional MRI sequences in detecting CVT (93% sensitivity and 100% specificity).40
CT and MR venography
Both CT venography (CTV) and MR venography (MRV) are highly accurate in diagnosing CVT when the two imaging modalities are compared directly with each other or with digital subtraction angiography (DSA).41–43 The choice of imaging is based on the assessment of the risk of ionizing radiation and iodinated contrast required for CTV versus contraindications to MRI such as the presence of implantable devices or metallic foreign bodies. The estimated sensitivity and specificity of CTV in diagnosing CVT is 75–100%.41 Two dimensional (2D) time-of-flight MRV does not require the use of gadolinium contrast. Depending on the plane of image acquisition, saturation and nulling of the venous signal can occur, leading to misdiagnosis of CVT with false-positive results for the extent of thrombus or failure to differentiate thrombus from dural sinus hypoplasia.44 45 Three-dimensional (3D) contrast-enhanced MRV is better than time-of flight MRV with multiplanar imaging in providing consistent visibility of the venous anatomy including the large dural venous sinuses, deep venous system, and smaller cortical veins, resulting in improved accuracy in diagnosing CVT (figure 2D).44 46 The reported sensitivity and specificity of 3D contrast-enhanced MRV are 93% and 100%, respectively.40
There are limited data on the value of perfusion imaging in the diagnosis and management of CVT. However, these studies are not included in the standard diagnostic imaging algorithm. Studies suggest that changes in cerebral blood flow and volume in CVT may be analogous to the ‘core and penumbra’ phenomenon in arterial ischemic stroke.47–49
Digital subtraction angiography
Digital subtraction angiography may show (1) non-visualization of dural sinus or cortical vein(s), (2) intraluminal filling defects, and (3) angiographic evidence of venous congestions such as engorgement of cortical veins, visualization of prominent medullary veins or reversal flow of cortical vein. In comparison with other non-invasive imaging methods, DSA can demonstrate both anatomical status and physiological response of each individual who develops CVT. The visualized physiological response, such as venous collateral pathways and altered venous phases of brain circulation, may explain, and provide some clues to, individual differences of patients with CVT. However, DSA has not been the main preferred modality for the diagnosis of CVT.22 Data from multicenter registries show that the imaging diagnosis of CVT is most commonly established with a combination of MRI and MRV (44–71%), whereas catheter angiography is needed in only 12–21% of cases to help establish the diagnosis.28 50 With continued advancements in the non-invasive imaging of CVT, it is expected that the role of DSA as a diagnostic tool will further decline. Studies comparing the accuracy of non-invasive CTV with DSA in the diagnosis of CVT have suggested that conventional angiography may be especially helpful in cases of CVT involving the cavernous sinus and the smaller deep veins, such as the internal cerebral veins, thalamostriate veins, and the basal vein of Rosenthal.51 52
Medical and surgical treatment
The goals of CVT management are to prevent the progression of venous thrombosis, re-establish venous flow, and manage underlying cause(s) of any prothrombotic state to prevent recurrence of CVT. Management of the underlying etiologies and prevention of CVT recurrence are beyond the scope of this document.
Systemic anticoagulation has been regarded as the first-line treatment,4–6 while surgical and neurointerventional procedures, such as ventriculostomy, decompressive surgery, intrasinus thrombolysis, and/or mechanical thrombectomy, are usually reserved for patients who do not respond to anticoagulation therapy.5 6 22 53 However, in a multicenter prospective study (International Study on Cerebral Vein and Dural Sinus Thrombosis), even with anticoagulation therapy, about 13% of patients with CVT either died or were dependent.50 Thus, there is a clear need for further therapeutic advancement. Neurointerventional procedures such as thrombectomy might improve clinical outcomes while maintaining safety for a selected group of patients with CVT.11 54–57
Anticoagulation
Two randomized controlled trials have investigated the efficacy of anticoagulation therapy. The first, a randomized, blinded placebo-controlled study in patients with aseptic dural sinus thrombosis using intravenous unfractionated heparin (UFH) was stopped after enrollment of the initial 20 patients because of a significant difference in outcome between the heparin and placebo group favoring UFH.18 In that trial, heparin was started with a 3000 IU intravenous bolus followed by continuous infusion until the initial partial thromboplastin time (PTT) doubled but did not exceed 120 s, with a target PTT of 80–100 s. The beneficial effects of heparin were seen after 3 days and up to 3 months. However, this trial was criticized for several reasons, including the small sample size and delayed enrollment into the study, which might have excluded severely ill patients and unvalidated outcome measurements employed in the study.58 The second trial compared subcutaneous nadroparin based on body weight versus placebo and demonstrated safety but failed to show statistically significant improvements in clinical outcomes.19 The nadroparin used in this trial was 180 anti-factor Xa IU/kg per 24 hours administered by two daily subcutaneous injections. A meta-analysis and systematic review of these two trials showed fewer dead or dependent patients with anticoagulation but failed to reach conventional statistical significance.6 59 Nevertheless, because of the relative safety of intravenous heparin therapy, and favorable statistical trends in the previous clinical trials, full anticoagulation remains first-line treatment for CVT regardless of the presence of intracerebral hemorrhage.60
There is no high level of evidence about which type of heparin results in a better clinical outcome in acute CVT. However, a systematic review of prior randomized trials and case series suggests that low molecular weight heparin is preferred over UFH.59 61 62 Regardless of anticoagulation therapy, coma, intracranial hemorrhage, and thrombosis of the deep cerebral venous system on admission were associated with unfavorable outcome.50 63
Intracranial pressure monitoring and management
Transcranial Doppler imaging has been used to non-invasively estimate intracranial pressure (ICP) in CVT.64 However, there is also evidence that the pulsatility index that is used as a surrogate marker of ICP in this method may not be accurate.65 Conflicting data exist for the role of external ventricular drainage or ventriculoperitoneal shunts in patients with CVT.66 67 These procedures can also be complicated by risks of anticoagulation.
Hemicraniectomy
Decompressive craniectomy and hematoma evacuation are typically reserved for patients with CVT with large parenchymal lesions causing herniation.68–70 Surgical intervention can result in a good functional outcome even in the most severe cases of CVT.69 70 Early surgery (within 12 hours of admission), and younger patients are predictors of good outcome after decompressive craniectomy.68 There are no data to guide when to choose hemicraniectomy over endovascular management, or when and how to combine them in treating patients with severe thrombosis.
Endovascular management
Indications
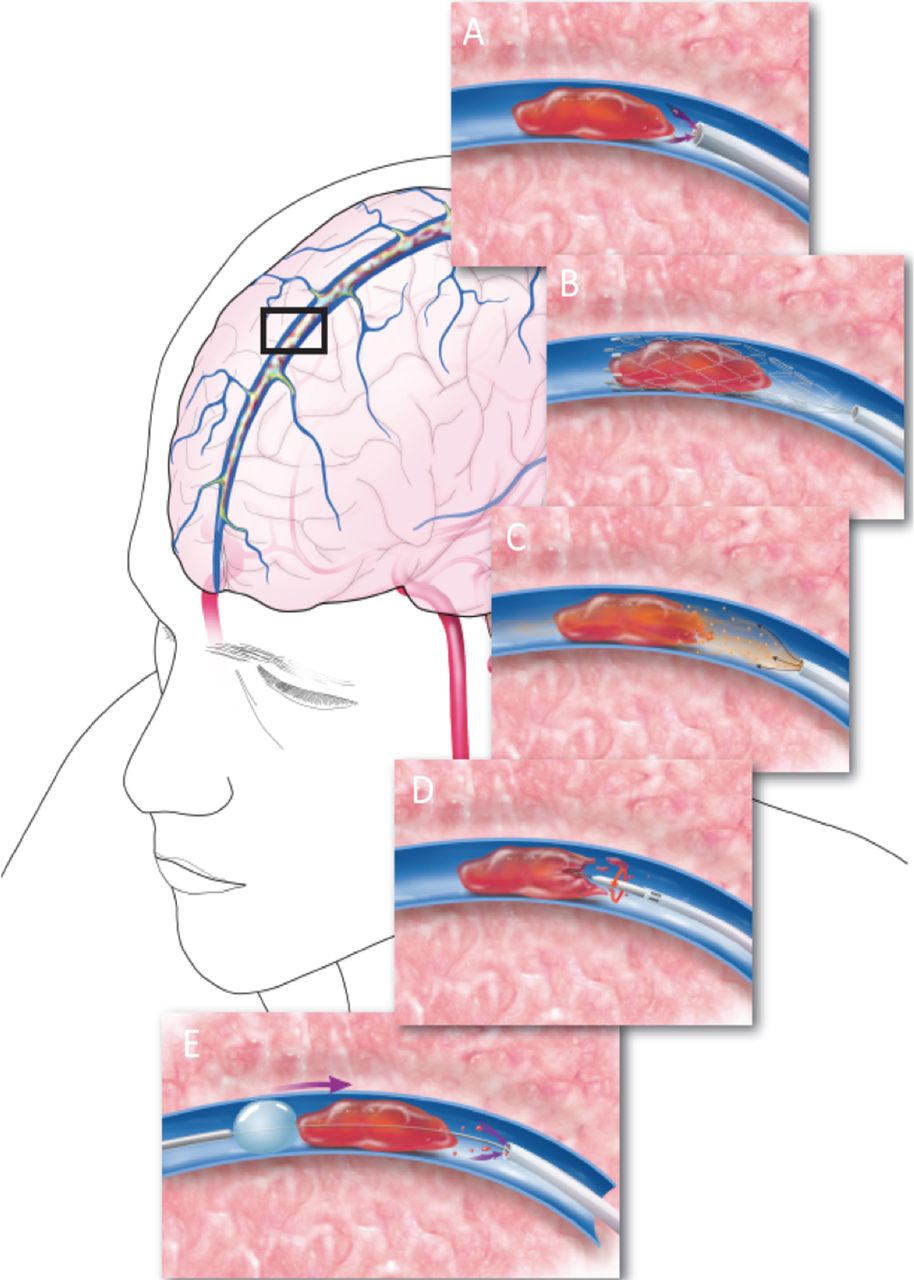
Neurointerventional procedures for CVT management are considered in patients with clinical deterioration or progression of intracerebral hemorrhage/venous infarction despite anticoagulation, severe stupor, comatose presentations, deep CVT, posterior fossa involvement or major contraindications to anticoagulation, such as bleeding disorders, thrombocytopenia (<100×109/L), or recent GI hemorrhages.18 20 63 However, exact indications for neurointerventional procedures require further validation. There is insufficient evidence to determine which approach and/or device provides the optimal restoration of venous outflow in CVT.71 72 An illustration of the different approaches to endovascular therapy for CVT is shown in figure 3.
{kind=link}
{kind=link}
{kind=link}
Illustration showing reported methods for venous sinus thrombectomy. These include (A) direct aspiration using an ADAPT technique, (B) mechanical thrombectomy with stent retrievers, (C) direct thrombolysis with local injection of thrombolytics, (D) clot disruption with Angiojet irrigation, (E) and mechanical suction with balloon-stabilized aspiration.
Procedural techniques
Arterial and venous access
A 4 or 5 French arterial sheath is typically sufficient for arterial access to perform diagnostic cerebral angiography. The venous phase, including the delayed venous phase, can confirm the location and extent of sinus occlusion as well as venous collateral pathways. For femoral venous access, a 6F long sheath will accommodate most thrombectomy devices, though a 7F or 8F sheath can be used to capture larger clot burdens with a larger catheter system. The guiding catheter or guide sheath is often placed in the internal jugular vein but if necessary can be delivered as far distally as the transverse sinus or torcular confluence. Also, an intermediate catheter can be used through the sheath, which can facilitate additional stability for endovascular devices. Direct access into the internal jugular vein provides alternative venous access, but access site thrombosis may compromise cerebral venous drainage if the contralateral jugular bulb is not adequate.
Pharmacological thrombolysis
Vines and Davis first performed intravenous pharmacological thrombolytic therapy for CVT using urokinase.73 Scott et al reported the first local urokinase infusion using an endovascular technique in 1988.74 Since then, there have been many reports using various thrombolytic agents with excellent to good clinical outcome.75–81 In cases of extensive CVT, following local intrasinus delivery of an initial bolus of a thrombolytic agent, a microcatheter can be placed within the affected sinus for a continuous drip. Continuous intrasinus alteplase infusion can be delivered at the rate of 1–2 mg/hour, and repeat angiography may be performed within 12–24 hours to measure the response to local thrombolysis to determine when discontinuation of such therapy is appropriate.82–83 The pharmacological thrombolysis technique can be combined with other thrombectomy techniques.
Direct aspiration thrombectomy
Analogous to arterial thrombectomy, large-bore distal aspiration catheters are now increasingly used for direct thrombus aspiration in CVT.84 This approach may be used alone or in conjunction with stent retriever thrombectomy.72 85– 86
Stent retriever thrombectomy
A variety of approaches to stent retriever thrombectomy combined with other endovascular modalities have been reported. A stent retriever may be used alone as treatment or in combination with local pharmacological thrombolysis.87–88 A stent retriever may also be used as an anchor while the distal access (aspiration) catheter is passed back and forth to aspirate the thrombus.89 Alternatively, a stent retriever and thrombus are removed into the aspiration catheter or as a unit into the large proximal guide sheath under ongoing continuous aspiration.90 This allows the thrombus to be captured by both aspiration and stent retriever devices.
Balloon thrombectomy
In this approach, a balloon is placed past the thrombus within the affected sinus/sinuses, inflated and retracted back toward the aspiration or guide sheath. This approach can be further combined with local pharmacological thrombolysis for effective removal and to prevent large pulmonary emboli. Fogarty 3 or 4F balloon catheters are ideal to match the larger size of the dural sinuses for effective and efficient thrombectomy, but other lower profile, compliant and semicompliant neurovascular balloon microcatheters have also been successfully used for this approach.91 92
Balloon angioplasty and stenting
Angioplasty and stenting are used as rescue therapy when other more traditional modes of thrombectomy fail.93 Angioplasty/stenting as a first-line endovascular treatment of CVT has not been evaluated.
AngioJet
AngioJet (MEDRAD Inc, Warrendale, Pennsylvania, USA) uses hydrodynamic thrombolytic action through high-velocity saline jets.94 The aspiration force draws the thrombus debris to the catheter inflow zone where it is evacuated from the body through the catheter.
Owing to the stiffness and bulkiness od the AngioJet, many operators have used the device for the initial partial recanalization of thrombosed dural venous sinuses. In a systematic review of 185 cases of CVT treated with mechanical thrombectomy, AngioJet use was associated with lower rates of complete recanalization and a lower chance of good outcomes than the use of other thrombectomy devices.56
Periprocedural details
In nearly all patients with CVT systemic heparinization will be initiated before the start of the endovascular thrombectomy thus requiring serial activated clotting time (ACT) measurements and adjustment of bolus doses of systemic heparin in the angiography suite. Intravenous heparin is administered to achieve an ACT of 250–300 s during endovascular therapy. Effective anticoagulation is essential for procedural success in patients undergoing interventional therapy, and adequate postprocedural anticoagulation is important for preventing re-occlusion postoperatively.
Goals of endovascular therapy
Recanalization, either complete or partial, is associated with improved outcomes of CVT in comparison with patients with no recanalization, although the quality of data is limited by the small sample sizes in the studies that reported such an association.95–96 The goal of endovascular therapy is to re-establish anterograde venous outflow in the targeted sinus(es) to alleviate malignant venous congestion/hypertension and prevent its associated complications.
Summary of recommendations
Imaging
A combination of MRI/MRV or CT/CTV studies should be performed in patients with suspected CVT (class I; level of evidence C).
DSA as a diagnostic modality is indicated in cases of suspected CVT when the diagnosis of CVT cannot be reliably established with non-invasive imaging alone (class IIa; level of evidence C).
Medical and surgical treatment
Anticoagulation with unfractionated heparin or low molecular weight heparin is reasonable in patients with CVT (class IIa; level of evidence C).
Decompressive craniectomy may be considered in patients with large parenchymal lesions causing herniation or intractable intracranial hypertension (class IIb; level of evidence C).
Endovascular therapy
Endovascular therapy may be considered in patients with clinical deterioration despite anticoagulation, or with severe neurological deficits or coma (class IIb; level of evidence C). The duration of anticoagulation therapy before declaring it to be a ‘failure’ and proceeding with endovascular therapy is unknown.
There is insufficient evidence to determine which endovascular approach and device provides the optimal restoration of venous outflow in CVT. In many cases, a variety of treatment approaches is required to establish sinus patency.
Acknowledgments
We would like to acknowledge the contribution of Tom Dolan in providing the medical illustration for Figure 2.
References
Footnotes
Contributors S-KL was the primary author and was responsible for overseeing construction of the document outline, gathering of evidence, and drafting of the manuscript. He also contacted our guest author (MGB) as a topic expert, and sought her input. MM made major contributions to the manuscript draft, and supplemented entire sections of the text. He also participated in discussions about the outline and organization of the text. SWH provided review and additional text to the manuscript. JTF acted as a representative of the Board of the Society of NeuroInterventional Surgery, and provided commentary and editing on behalf of the Board and of the Society as a whole. MGB was the invited topic expert, whose knowledge and experience in venous thrombosis disease provided vital international perspective. JFF, as senior author, was responsible for organizing the writing group, overseeing the outline construction, facilitating communication between the writing group and the Standards and Guidelines Committee, drafting and editing of the manuscript, and submission/proofing for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer This literature review (“Review”) is provided for informational and educational purposes only. Adherence to any recommendations included in this review will not ensure successful treatment in every situation. Furthermore, the recommendations contained in this review should not be interpreted as setting a standard of care, or be deemed inclusive of all proper methods of care or exclusive of other methods of care reasonably directed to obtaining the same results. The ultimate judgment about the propriety of any specific therapy must be made by the physician and the patient in light of all the circumstances presented by the individual patient, and the known variability and biological behavior of the medical condition. This review and its conclusions and recommendations reflect the best available information at the time it was prepared. The results of future studies may require revisions to the recommendations to reflect new data. SNIS does not guarantee the accuracy or completeness of the review and assumes no responsibility for anyinjury or damage to people or property arising out of, or related to, any use of this review or for any errors or omissions.
Competing interests JFF is an equity interest holder for Fawkes Biotechnology, LLC, and a consultant for Stream Biomedical. SWH is a consultant for Medina and Neuravi, and has research contracts with Stryker Neurovascular, Siemens, MicroVention Terumo. JTF has research grants from Stryker and Microvention, equity interest in Endostream, Cerebrotech, and The Stroke Project, and has consulted for Stryker and Penumbra. MM is a consultant for Toshiba (Canon) Medical. All other authors report no relevant conflicts of interest.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators T Abruzzo, B Albani, SA Ansari, AS Arthur, M Bain, B Baxter, KR Bulsara, M Chen, G Dabus, D Frei, CD Gandhi, MS Hussain, MV Jayaraman, Y Kayan, RP Klucznik, T Leslie-Mazwi, WJ Mack, RA McTaggart, PM Meyers, J Mocco, AT Patsalides, CJ Prestigiacomo, GL Pride, Jr, RM Starke, PJ Sunenshine.